





Abstract
A 52-year-old man noted large amounts of bloody sputum and visited our hospital. Chest X-ray showed a mass shadow in the right upper lung field. He was diagnosed with squamous cell carcinoma (SCC). Although he was not aware of symptoms other than the bloody sputum, his blood chemistry showed a high total serum protein level of 10.6 g/dl. Further analysis of serum immunoglobulin revealed a markedly high immunoglobulin G (IgG) level, but an abnormally low level of immunoglobulin A (IgA) and immunoglobulin M (IgM). Serum immunoelectrophoresis detected IgG-λ monoclonal protein; therefore, we suspected the coexistence of multiple myeloma, amyloidosis, benign macroglobulinemia, or benign monoclonal gammopathy. Since the patient continued to expectorate large amounts of bloody sputum every day, and his anemia progressed, right upper lobectomy and lymph node dissection were performed on a semi-emergent basis without preoperative bone marrow examination. On thoracotomy at the level of the fifth intercostal space, the fifth and sixth ribs were partially resected posteriorly, and the resected ribs were submitted for pathological examination. The postoperative pathological diagnosis was SCC of the lung (p-T2N0M0, stage IB). Pathological examination of the ribs revealed IgG-λ myeloma. Herein, we report a patient with lung cancer in whom multiple myeloma was definitively diagnosed from rib specimens resected at thoracotomy.
1. Introduction
Multiple myeloma usually manifests systemic symptoms that make it difficult to diagnose. The detection of monoclonal (M)-protein is a sensitive screening test for multiple myeloma. However, since M-protein is also detected in benign diseases, such as benign monoclonal gammopathy, bone marrow examination is usually performed to establish the diagnosis. In this patient, the rib specimens resected at thoracotomy for lung cancer surgery were submitted for pathological examination, which provided a definitive diagnosis of multiple myeloma. We report the case with a review of the literature.
2. Case report
A 52-year-old man noted large amounts of bloody sputum in October 2008, and visited our hospital. Chest X-ray showed a mass shadow in the right upper lung field. He underwent a computed tomography (CT)-guided needle biopsy, and was diagnosed with squamous cell carcinoma (SCC). His past medical history was unremarkable. He had smoked two packs of cigarettes per day for 30 years. He was in good health except for the chief complaint.
Chest X-ray showed a well-defined mass of 3 cm in diameter in the right upper lung field (Fig. 1a ). Chest CT also revealed a 30-mm lobulated, heterogeneous, irregularly bordered mass in S1 of the right lung (Fig. 1b). A ground-glass appearance suggestive of hemorrhage was observed around the tumor (Fig. 1b). Blood chemistry showed a high total serum protein level of 10.6 g/dl. Serum immunoglobulin analysis revealed an abnormally high immunoglobulin G (IgG) level of 6377 mg/dl (normal range, 680–1620 mg/dl), but an abnormally low level of immunoglobulin A (IgA) at 4 mg/dl (normal range, 84–438 mg/dl) and immunoglobulin M (IgM) at 2 mg/dl (normal range, 57–288 mg/dl). β-2 microglobulin was also elevated to 3.6 mg/l (normal range, 0.9–1.9 mg/l). Serum immunoelectrophoresis detected an IgG-λ M-protein. The tumor markers NSE, CYFRA, CEA, and SCC were within normal limits. As preoperative examinations, imaging studies, including bone scintigraphy, positron emission tomography (PET), chest X-ray, chest CT, abdominal CT, and brain CT, revealed no metastases to other organs, or bone lesions anywhere.
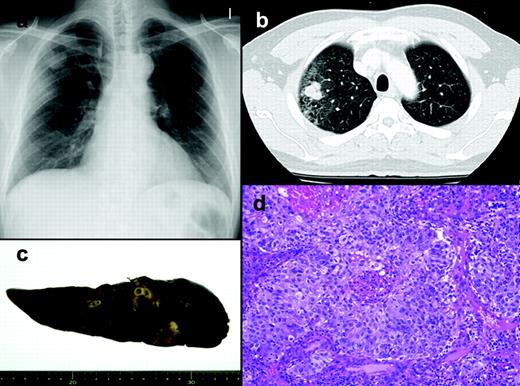
Radiological and pathological findings of the lung cancer. (a) Preoperative chest X-ray. (b) Preoperative chest CT. (c) Macroscopically, the lung cancer contained a hemorrhagic area. (d) Histology of the lung cancer showing squamous differentiation.
Since the patient continued to expectorate large amounts of bloody sputum every day, and his anemia progressed, a right upper lobectomy with hilar and mediastinal lymph node dissection was performed on a semi-emergent basis without preoperative bone marrow examination. On thoracotomy at the level of the fifth intercostal space, the fifth and sixth ribs were partially resected posteriorly, and the resected ribs were submitted for pathological examination. The resected ribs showed no gross abnormalities. The lung cancer which measured 33×27×20 mm, was yellowish with an irregular margin, and contained a hemorrhagic area (Fig. 1c). The postoperative pathological diagnosis was SCC of the lung (p-T2N0M0, stage IB) (Fig. 1d). However, pathological examination of the ribs showed that the bone marrow was hypercellular, with a cellularity of approximately 80% (Fig. 2a ). Cells of three lineages were identified, with diffuse proliferation of plasma cells (Fig. 2b). The plasma cells had relatively uniform nuclei with dispersed chromatin. Immunohistochemically, the plasma cells expressed CD38 and more IgG and λ-light chain than IgA, IgM and κ-light chain (Fig. 2c–f). These findings led to a diagnosis of IgG-λ myeloma.
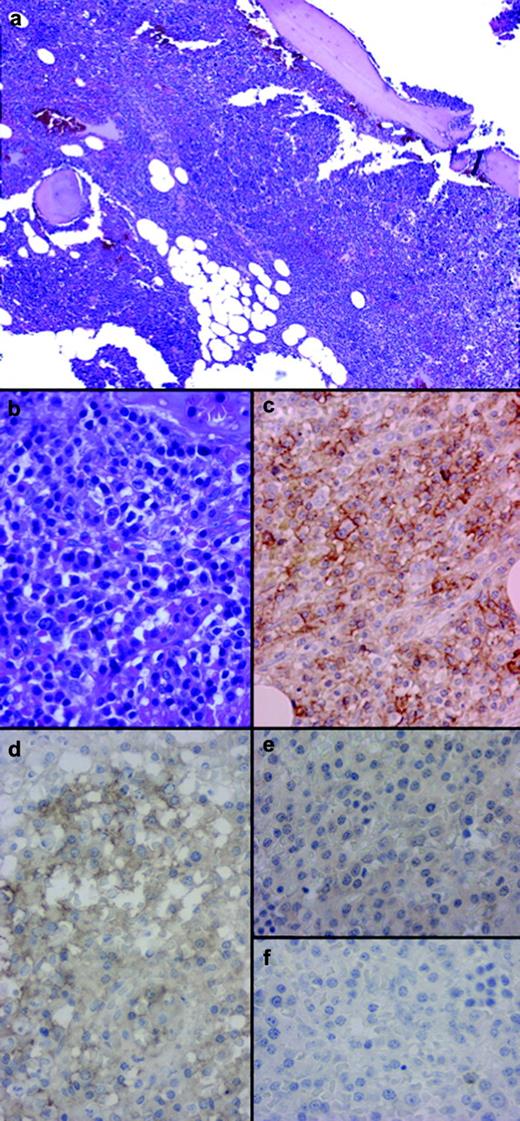
Pathological examination of the ribs. (a) Low magnification view of the bone marrow showed hypercellularity. (b) High magnification view of the bone marrow showed diffuse infiltration of plasma cells. (c) Immunohistochemically, plasma cells were positive for CD38. (d–f) Immunohistochemically, most of tumor cells in bone marrow were positive for IgG staining (d), but negative for IgA staining (e) and IgM staining (f).
The patient's postoperative course was uneventful. After surgery, he produced no bloody sputum and his anemia markedly improved. The preoperative anemia was retrospectively thought to be due not to multiple myeloma, but to persistent bleeding from the lung cancer. He received high-dose dexamethasone therapy from January 2009, and to date has been following a favorable course. He will also be followed-up for the recurrence of lung cancer on an outpatient basis.
3. Discussion
Multiple myeloma is characterized by the neoplastic proliferation of a single clone of plasma cells producing a monoclonal immunoglobulin [1]. The exact cause of multiple myeloma is unknown. The theory that multiple myeloma is likely to be associated with specific solid cancers, such as lung cancer is no longer considered valid, and no common occupational or environmental carcinogens have been identified [2–4].
In the present case, the initial high level of total serum protein suggested multiple myeloma. Generally, findings suggestive of multiple myeloma include bone pain, an increased serum protein concentration, hypercalcemia, anemia and acute renal failure, and so on [1]. The most important diagnostic finding of multiple myeloma is the presence of M-protein in the serum or urine, noted in 93% of patients [5]. In the present patient, M-protein was detected in the serum. The serum β-2 microglobulin level is reported to be elevated (>2.7 mg/l) in 75% of patients at the time of diagnosis [5], which was the case in this patient. Those with high β-2 microglobulin levels show poor survival [3]. A prolonged delay before diagnosis is associated with a significant impact on the clinical course of multiple myeloma [6]. There is a need to raise awareness of the presentation of this condition.
As a rule, multiple myeloma has a rather low metabolic activity, and PET/CT with 18-fluoro-deoxyglucose is insensitive to diffuse bone marrow infiltration in multiple myeloma, because the local cell density is too low [7, 8]. In this patient, no solid plasma cell tumors were observed anywhere in the body. Since he had diffuse plasma-cell bone marrow infiltration, PET/CT showed no abnormalities. The definitive diagnosis of multiple myeloma usually requires bone marrow aspiration or biopsy. The bone marrow contained 10% or more plasma cells in 96% of patients with multiple myeloma [5], as observed in the present patient. When performing lung cancer surgery, partial rib resection is a frequent, routine surgical procedure in lung cancer surgery. We demonstrated that multiple myeloma can be diagnosed from resected rib specimens. The results suggest that, when operable lung cancer patients require semi-emergent surgery, it is possible to lessen the burden on the patient and efficiently and reliably diagnose multiple myeloma by partially resecting the ribs at the time of surgery and submitting them for pathological examination.
Since bone scintigraphy has a low sensitivity in myeloma, it is not used to diagnose the disease or to determine the therapeutic response [1, 3]. In the postoperative follow-up of lung cancer, a hot spot on bone scintigraphy indicates a strong likelihood of a metastasis of lung cancer in view of the detection sensitivity. However, in practice, the clinical course should be comprehensively evaluated for the diagnosis. If it is difficult to differentiate multiple myeloma from bone metastasis of lung cancer, a definitive diagnosis may require biopsy.
The overall five-year survival rate of patients treated for multiple myeloma was reported to be approximately 30% [3]. Since the operative curability of the lung cancer in this patient seemed high, the multiple myeloma is being aggressively treated. He received high-dose dexamethasone therapy, and has been following a favorable course. We are considering thalidomide therapy depending on the future clinical course of the disease [9, 10].

{kind=link}
{kind=link}