


Abstract
Background: Long-term functional outcomes of supracondylar elbow fractures (SCEF) have not been well documented in the literature. We retrospectively evaluated functional outcomes of pediatric SCEF using the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire.
Methods: We retrospectively reviewed the outcomes of patients who presented to our tertiary care pediatric emergency department with SCEF between January 2005 and December 2009. We reviewed their charts to assess several clinical parameters, including age, sex, Gartland classification of SCEF, weight, comorbidities, treatment intervention, physiotherapy and the extremity involved. The DASH questionnaire was administered in 2012. We performed a multiple linear regression analysis to determine the significance of these clinical parameters as they related to the DASH score for functional outcome.
Results: We included 94 patients with SCEF in our review. Pediatric SCEF had good functional outcomes based on the DASH questionnaire (mean score 0.77 ± 2.10). We obtained the following DASH scores: 0.45 ± 2.20 for type I, 1.09 ± 1.70 for type II and 1.43 ± 2.40 for type III fractures. There was no statistical difference in functional outcome, regardless of sex (p = 0.07), age at injury (p = 0.96), fracture type (p = 0.14), weight (p = 0.59), right/left extremity (p = 0.26) or surgery (p = 0.52).
Conclusion: Our results demonstrate that good functional outcomes can be expected with pediatric SCEF based on the DASH questionnaire, regardless of age at injury, sex, weight, right/left extremity or surgical/nonsurgical intervention, provided satisfactory reduction is achieved and maintained.
Pediatric supracondylar elbow fractures (SCEF) are a common occurrence in children. These fractures are commonly extra-articular, unlike adult SCEF. Return of elbow motion after treatment of supracondylar humeral fracture in children has been well documented in the literature.1 However, the return of elbow range of motion and function is usually measured as an objective parameter, such as a return of normal range of arc motion in the sagittal plane (flexion and extension).1 Long-term functional outcome using standardized tools has not been well documented in the literature. One study analyzed the correlation between the values of a modified Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire and change of elbow function after SCEF of the humerus.2 However, the study addressed only flexion SCEF, which represents a small percentage of pediatric SCEF. The authors concluded that the value of a modified DASH questionnaire correlates with objective indicators of elbow function after flexion SCEF in children. A standardized functional outcome tool, such as the well-validated DASH questionnaire, has been instrumental in measuring functional disability.
Bot and colleagues3 evaluated the clinimetric quality of 16 self-administered shoulder disability questionnaires, including DASH, the Shoulder Pain and Disability Index and the American Shoulder and Elbow Surgeons Standardised Shoulder Assessment Form. For clinimetric purposes, the DASH questionnaire received the best ratings.3 Thus, we chose the DASH questionnaire, as it is a region-specific standardized functional outcome tool that is well validated has been important in measuring functional disability.
The purpose of the present study was to provide a retrospective, longitudinal evaluation of functional outcome in a large population of children treated for pediatric SCEF, using the DASH for standardized measure of outcome. A secondary goal was to determine whether factors such as age at injury, sex, weight, right or left extremity, Gartland fracture type and surgical versus nonsurgical intervention could predict long-term functional outcomes.
Methods
We retrospectively reviewed the cases of children with SCEF who presented to our tertiary care pediatric emergency department between January 2005 and December 2009. We reviewed their charts for several parameters, including age, sex, classification of fracture severity, weight, comorbidities, operative or nonoperative treatment intervention, postoperative physiotherapy and associated nerve injury. A DASH questionnaire was administered in 2012 by the parents of the patients with the child present; if they were old enough, the patients completed the questionnaire themselves under a parent’s supervision. We chose to remove the sex-related question to make the questionnaire more age appropriate. The optional work module was not used, but the optional sports/performing arts module was.
The DASH score is scaled between 0 and 100. Higher scores indicate worse function, and lower scores indicate better function relating to upper-extremity disability.
Our inclusion criteria for joining the study were isolated extension SCEF in patients younger than 13 years at the time of injury, closed injury and consent to join the study (obtained from parents). The exclusion criteria were poly-trauma, flexion type SCEF, ipsilateral injury requiring surgery, iatrogenic neurologic injury, reinjury to the same elbow within the study period, metabolic bone disease, condyle, epicondyle fractures and transphyseal fractures that had been reported as SCEF. We chose to exclude the flexion type SCEF owing to the small number (1.2%) of patients with this condition.
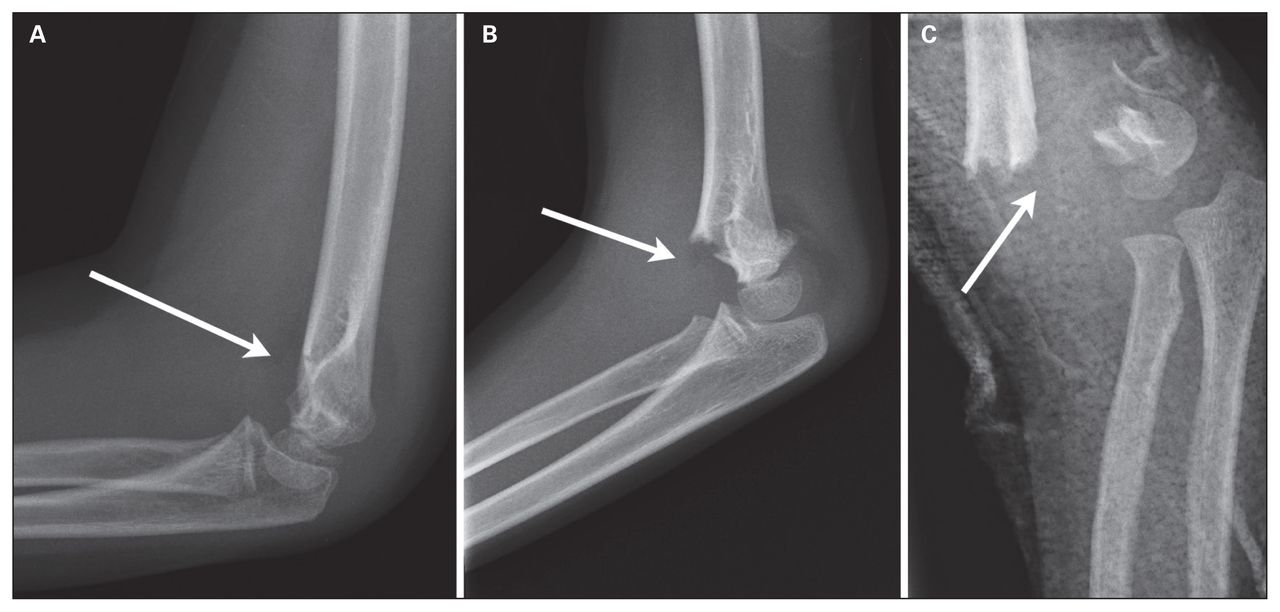
Three fellowship-trained pediatric orthopedic surgeons independently reviewed the radiographs and grouped the patients according to the Gartland classification,4 which is widely used in the literature. In the Gartland classification system, type I fractures are essentially nondisplaced. Type II fractures are displaced with a variable amount of angulation, but more importantly, the posterior cortex of the humerus is intact. Type III fractures are completely displaced, with no cortical continuity (Fig. 1). A κ value for interobserver agreement was then calculated.

Types of supracondylar fractures. A) type I supracondylar fracture with a posterior fat pad sign, B) type II supracondylar fracture with an intact posterior hinge, C) type III supracondylar fracture with no cortical continuity. Arrows delineate fracture lines.
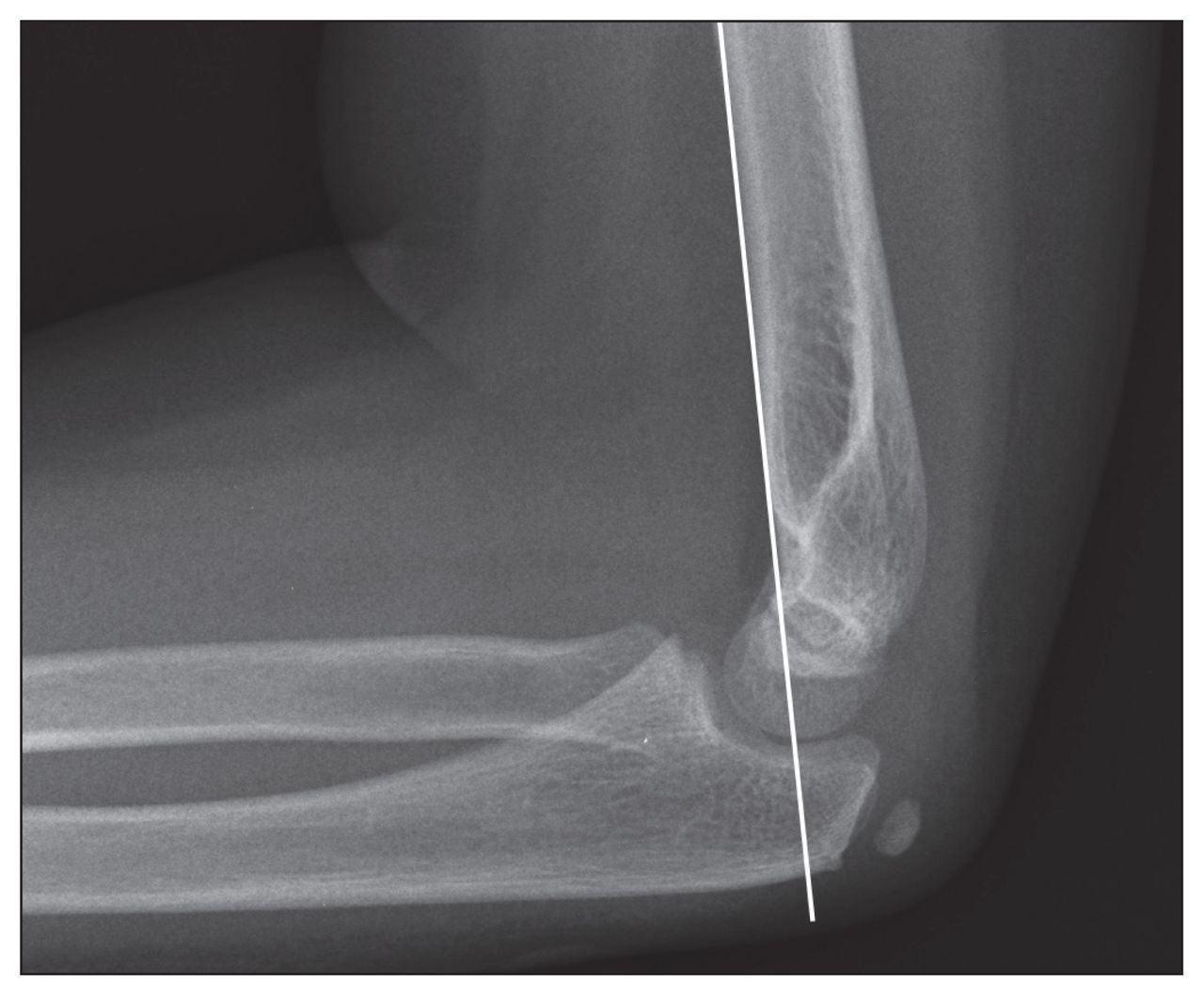
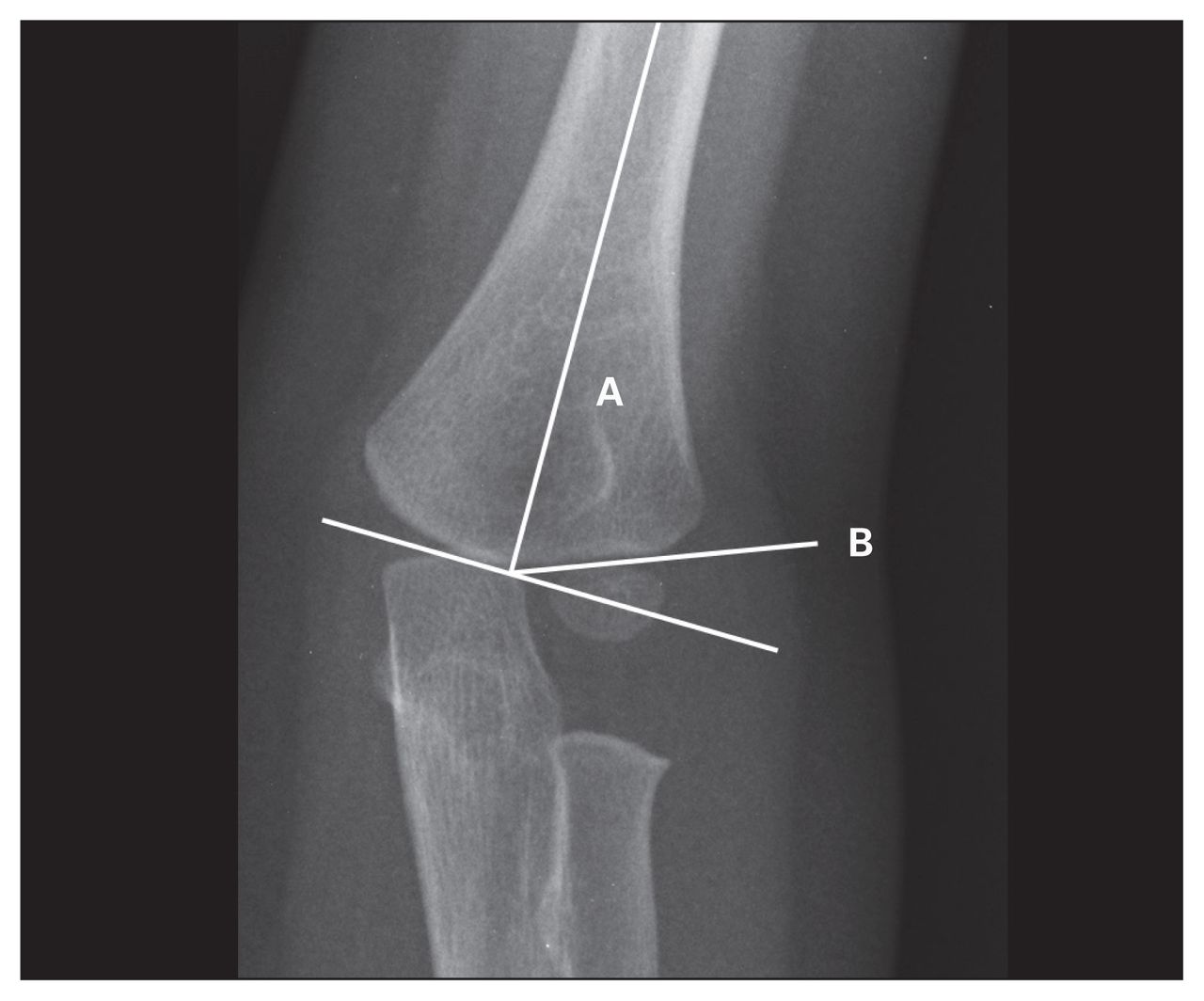
The pediatric orthopedic surgeons in our tertiary care centre treated patients either operatively or nonoperatively based on the degree of angulation and displacement (displacement of the anterior humeral line [Fig. 2] and alteration of the Baumann angle [Fig. 3]).

Anterior humeral line, drawn in line with the anterior humeral shaft, should intersect the middle of capitellum.

Baumann angle: (A) Angle between long axis of humeral shaft and (B) growth plate of lateral humeral condyle.
The anterior humeral line should intersect the middle third of the capitellum on lateral radiographs. A Baumann angle within 5° of the uninjured side was considered acceptable. This was the radiographic measure of coronal plane deformity. The normal physiologic tilt of the capitellum on the humerus is about 30° anteriorly; reduction was not required if this physiologic angulation was 20° or more and if the anterior humeral line intersected the middle third of the capitellum on lateral radiographs in extension type SCEF. Type I fractures were treated nonoperatively. Type II fractures were treated operatively or nonoperatively depending on the amount of angulation and displacement. Type II fractures that failed closed reduction based on the radiographic parameters mentioned previously were treated operatively. All type III fractures were treated operatively. Patients who were managed operatively underwent closed reduction and percutaneous pinning using Kirschner wires under fluoroscopy. If reduction could not be obtained with closed reduction, open reduction and percutaneous pinning was performed.
Patients were seen by the pediatric orthopedic surgeons for scheduled follow-up visits. They were seen 10–14 days postoperatively for a cast change, wound check and radiographs to ensure displacement had not occurred. Displacement was measured using the anterior humeral line and the relationship with the capitellum. Alignment was considered acceptable if the anterior humeral line intersected the middle third of the capitellum on lateral radiographs. Patients were seen for pin removal and cast change at 4 weeks postoperative and again for final cast removal, radiographs and range of motion check at 6 weeks postoperative. At the 3-month follow-up, patients were seen to assess the need for physiotherapy and to check range of motion.
The patients who received closed reduction or who sustained a nondisplaced or minimally displaced SCEF not requiring closed reduction were casted and seen in clinic at 2 weeks postinjury for a cast check and radiographs and at 4 weeks for cast removal, radiographs and range of motion check.
Three fellowship-trained pediatric orthopedic surgeons followed all patients to ensure fracture healing, as seen radiographically. One of us (A.I.) independently reviewed all the radiographs to ensure that reductions were maintained and that fractures had healed.
Statistical analysis
Mean DASH scores were then calculated based on sex, right or left extremity, weight, intervention (operative v. nonoperative) and age at time of injury. A multiple linear regression analysis was then performed, and we considered results to be significant at p < 0.05.
Results
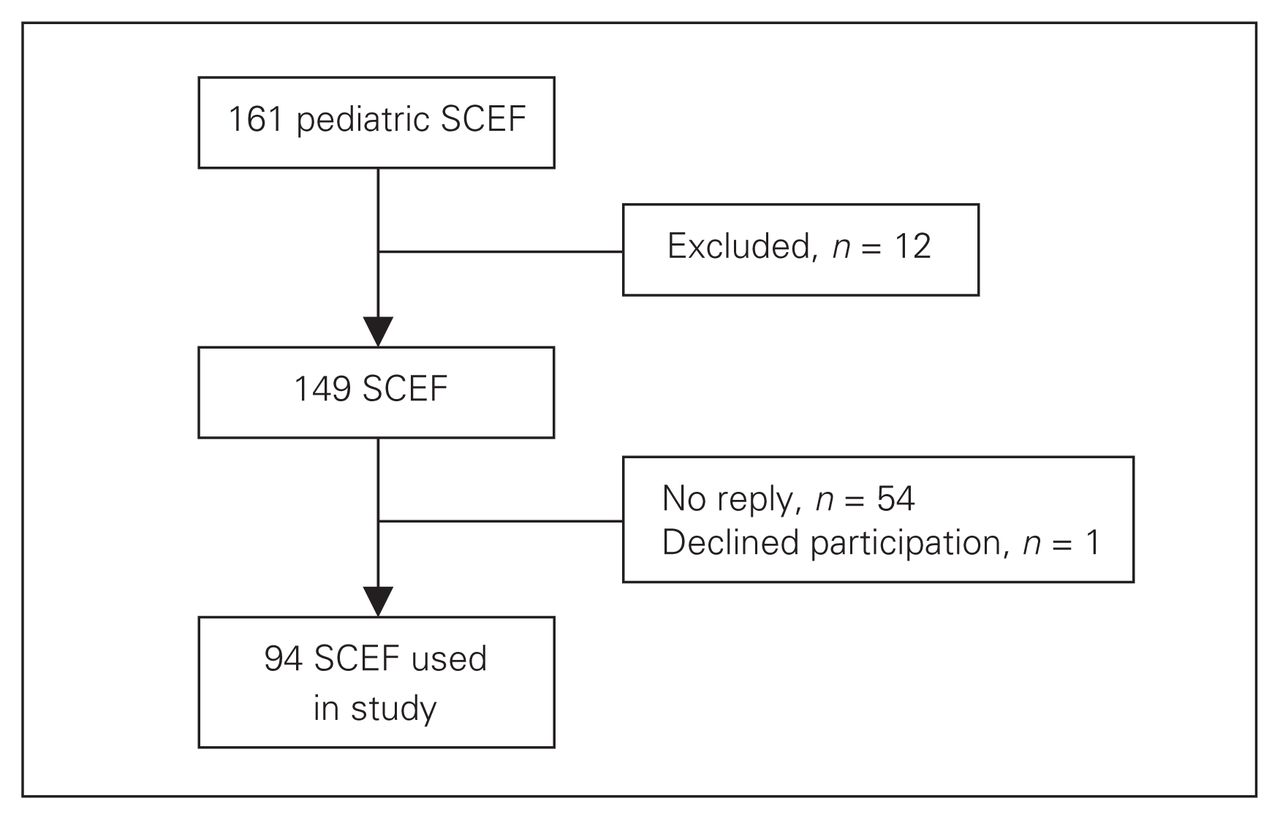
A total of 158 patients with 161 SCEF were eligible to participate in our study. Ten patients were excluded, as they did not meet the inclusion criteria. Fifty-four patients did not respond because they had moved away or changed phone numbers without providing an update in the medical record system, and 1 patient declined participation, leaving 94 patients for analysis (Fig. 4). Patients who did not reply or declined participation had a similar distribution in terms of type of SCEF compared with our study group (Table 1).

Enrolment of eligible patients. SCEF = supracondylar elbow fractures.
Distribution of supracondylar elbow fracture
Of the 94 patients included in the study (Table 2), 54 (57%) were male and 40 (43%) were female. We subdivided patients by fracture type: 53 (56.4%) had type I, 26 (27.7%) had type II and 15 (15.9%) had type III fractures; 2 (2.1%) had flexion type SCEF. Patients were further subdivided by sex, right or left extremity, weight, intervention (operative v. nonoperative) and age at time of injury (Table 2). There was a higher incidence of SCEF in boys (57%) than in girls, and the left elbow was more commonly injured than the right elbow (61.7%). The mean age of patients with type I SCEF was 70 months, type II was 74 months, type III was 83 months and Flexion type SCEF was 73.5 months (Table 2).
Patient demographics
A multiple linear regression analysis was performed to determine the significance of the clinical parameters as they related to the DASH score for functional outcome. There was no statistical difference in functional outcome using the DASH score regardless of sex (p = 0.07), age at injury (p = 0.96), type of fracture (p = 0.14), weight (p = 0.59), right or left extremity (p = 0.26) or surgery (p = 0.52; Tables 3 and 4).
Mean dash scores and standard deviation
Multiple linear regression analysis
Using the optional module (sports/performing arts), there was no statistical difference in functional outcome regardless of sex (p = 0.33), age at injury (p = 0.90, type of fracture (p = 0.62), weight (p = 0.99), or right or left extremity (p = 0.28; Table 5).
Multiple linear regression analysis of sports/performing arts module
Our interobserver agreement to indicate the reproducibility of the classification was calculated using weighted Fleiss κ, with κ representing the proportion of agreement among the orthopedic surgeons beyond that expected by chance. A value of 0 indicates what would be expected by chance and a value of 1 indicates perfect agreement. A value less than 0 is an indication that agreement is less than what is expected by chance.5 Our calculated κ score was 0.76, which represents good interobserver reliability (Table 6).
Interpretation of κ, Landis and Koch (1997)
Discussion
Supracondylar elbow fractures are common in children. The Gartland classification has been widely used for classication of pediatric SCEF. Ideally, a fracture classification system should be both prognostic and provide a guide to clinical management. Our study demonstrated no statistical difference in functional outcomes across all pediatric SCEF despite Gartland classification. There were no significant differences between other parameters, such as sex, right or left extremity, weight, intervention (operative v. nonoperative) and age at time of injury and their correlation with functional outcomes. These types of fractures, regardless of several parameters, tend to have good functional outcomes based on the DASH score, provided that satisfactory reduction is maintained by either surgical or nonsurgical (cast) means and that the technique of reduction and subsequent treatment course is uncomplicated.
The pediatric orthopedic surgeons at our institution still use the Gartland classification; however, for clinical decision making, degree of displacement is used. For example, not all Gartland type II SCEF were treated operatively; based on degree of displacement/intersection of the anterior humeral line and capitellum (Fig. 3) and the Baumann angle (Fig. 4) as well as on failure of closed reduction, patients were treated operatively or nonoperatively. There was no significant difference in DASH scores (p = 0.52) between patients treated operatively and those treated nonoperatively. This does not mean that surgery is not important in the management of pediatric SCEF; adequate reduction is important to the functional outcome. Inadequate reduction can lead to potential functional long-term problems.6 Garland type II SCEF is not an indication for surgery. The degree of displacement should guide management, as SCEF tend to do well if adequate reduction is obtained and maintained and if it follows an uncomplicated course. A study by Heal and colleagues7 further supports this, as they also conclude that pediatric SCEF should be treated based on the degree of displacement rather than the Gartland classification.
In the same study, based on a calculated κ score of 0.54, Heal and colleagues7 concluded that there was a moderate interobserver agreement with the Gartland classification, with poor agreement over type I extension SCEF, fair to moderate agreement with type II and good to very good agreement with type III using κ scores. Our interobserver agreement to indicate the reproducibility of the classification was calculated using weighted Fleiss κ, which represents the proportion of agreement among the orthopedic surgeons beyond that expected by chance. In contrast to Heal and colleagues,7 our calculated score was 0.76, which indicates substantial or good agreement among the orthopedic surgeons, bearing in mind that the calculated κ scores could also be due to chance.
Our study showed no statistical difference in the functional outcome based on the Gartland classification. Pediatric SCEF, if treated appropriately based on degree of displacement and adequacy/maintenance of closed reduction tend to do well despite the classification of fracture with little to no functional limitation of day-to-day activities or associated pain. In the sports/ performing arts module, there was also no statistical difference in mean DASH score among the groups (Table 4), regardless of age, weight, right or left extremity, sex, intervention (operative v. nonoperative) or Gartland classification of severity. These patients also tend to function well with no significant limitation in sports or performing arts (Table 5).
Spencer and colleagues1 demonstrated the effect of age and severity of fracture (determined by those requiring operative intervention) on the recovery of elbow motion, with patients older than 5 years demonstrating a 3%–9% lower relative arc of motion at the follow-up points than younger patients and a slower recovery in motion in those who had more severe fractures requiring surgical intervention. We studied whether there were any functional differences between these groups using the DASH questionnaire and found that despite the findings of Spencer and colleagues,1 there was no statistical difference in functional outcome regardless of age or operative or nonoperative intervention (p = 0.52) based on multiple linear regression analysis.
Limitations
The limitations of our study include the fact that it was retrospective and, in some cases, the parents filled out the DASH questionnaire based on their perceptions of their children’s functioning. Another limitation is the validity of this questionnaire in this age group. Although the DASH questionnaire has not yet been formally validated in this age group, multiple studies have used the DASH questionnaire in pediatric populations.8–11 There is also a possibility for skewed data given that 54 patients did not respond and 1 declined participation. Thus, given our small sample size, there is a chance that we missed the difference in DASH scores among the groups. We did not perform a subgroup analysis on the fractures treated with open reduction, as the numbers would be small and we would have therefore been unable to make firm statistical conclusions; however, this was not the primary focus of our study and represents a potential future area of research. Despite the small number at follow-up, we reviewed the charts of all 149 patients who were eligible for participation in the study to identify any adverse outcomes or the need for further therapy or intervention. There were none identified from our chart review. We also reviewed the surgeon’s notes at subsequent follow-ups.
To our knowledge, our study is the first to attempt to identify risk factors for poor functional outcomes using a standardized measure of outcome in a large group of children with all types of extension SCEF. Our study further provides a longitudinal evaluation of functional outcome in a large population of children treated for pediatric SCEF fracture using the DASH for standardized measure of outcome.
Conclusion
Return of range of motion after an isolated pediatric SCEF has been well documented in the literature. We found that overall, most parents and patients reported no functional interference with normal social activities, sports or performing arts, activities of daily living (including self-care), and no functionally limiting symptoms, regardless of age at injury, sex, weight, right or left extremity, operative or nonoperative intervention or Gartland classification, provided that satisfactory reduction is maintained by either surgical or nonsurgical (cast) means and that the means of reduction and treatment course are not complicated. Perhaps adequate reduction is more important than simply treatment of fracture type.
Acknowledegments
We thank Minnie Parsons for her help in the assembling of patient data, ensuring we had the necessary documentation to meet the ethics board requirements and printing and distributing the DASH questionnaire.
Footnotes
Presented as a poster at the annual meetings of the Canadian Orthopaedic Association 2013, Controversies in Rheumatology & Autoimmunity 2013 and the Orthopaedic Trauma Association 2013.
Competing interests: None declared.
Contributors: All authors designed the study. A.D. Isa acquired the data, which all authors analyzed. A.D. Isa and A. Furey wrote the article, which all authors reviewed and approved for publication.
- Accepted January 6, 2014.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.