
Journal of Orthopedics & Rheumatology
Download PDF
Case Report
*Address for Correspondence: Takatomo Mine, MD, Department of Orthopaedic Surgery, National Hospital Organization, Kanmon Medical Center, 1-1 ChofuUshirodaSimonoseki, Yamaguchi 752-8510, Japan, Tel: +81-83-2411199; Fax: +81-83-2411301; minet@kanmon-mc2.hosp.go.jp
Citation: Mine T, Ihara K, Kawamura H, Kuriyama R, Date R. Painful Patellar Partita Complicated with Intraarticular Ganglion. J Orthopedics Rheumatol. 2016; 3(1): 3.
Copyright © 2016 Mine T, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Orthopedics & Rheumatology | ISSN: 2334-2846 | Volume: 3, Issue: 2
Submission: 30 May, 2016 | Accepted: 06 July, 2016| Published: 11 July, 2016
Keywords: Patellar partita; Ganglion cyst; Arthroscopy

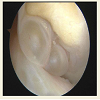
Arthroscopic examination identified cysts lying anterior to the proximal third of the PCL in the region between the ACL and PCL (Figures 2 and Figure 3). These cysts were tightly attached to the PCL and could not be separated by probing. The ACL was slightly compressed laterally and deformed. The cysts were excised arthroscopically in a piecemeal fashion.
Painful Patellar Partita Complicated with Intraarticular Ganglion
Takatomo Mine*, Koichiro Ihara, HiroyukiKawamura, Ryutaro Kuriyama and Ryo Date
- 1Department of Orthopaedic Surgery, National Hospital Organization, Kanmon Medical Center, Yamaguchi, Japan
*Address for Correspondence: Takatomo Mine, MD, Department of Orthopaedic Surgery, National Hospital Organization, Kanmon Medical Center, 1-1 ChofuUshirodaSimonoseki, Yamaguchi 752-8510, Japan, Tel: +81-83-2411199; Fax: +81-83-2411301; minet@kanmon-mc2.hosp.go.jp
Citation: Mine T, Ihara K, Kawamura H, Kuriyama R, Date R. Painful Patellar Partita Complicated with Intraarticular Ganglion. J Orthopedics Rheumatol. 2016; 3(1): 3.
Copyright © 2016 Mine T, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Orthopedics & Rheumatology | ISSN: 2334-2846 | Volume: 3, Issue: 2
Submission: 30 May, 2016 | Accepted: 06 July, 2016| Published: 11 July, 2016
Abstract
Painful patellar partita complicated with intraarticular ganglion cysts arising from the cruciate ligament is difficult to diagnose from the symptoms alone. In the patient reported here, knee pain was caused by patellar partita and by cysts attached anteriorly to the posterior cruciate ligament (PCL). The fragment of the bipartite patella was excised, and the cysts were resected arthroscopically in a piecemeal fashion. Knee pain and limitation of motion both resolved after surgery. We hypothesize that the pain and restricted range of motion were caused by both the bipartite patella and impingement of the ganglion cysts between the anterior cruciate ligament (ACL) and PCL. In particular, sudden onset of vague pain in this patient was likely to be due to impingement of the ganglion cyst between the ACL and PCL.Keywords: Patellar partita; Ganglion cyst; Arthroscopy
Introduction
Patellar partita is a well-known disease among young athletes. Bipartite patella has long been noted as a cause of anterior knee pain. In most patients with symptomatic patella partita, improvement is achieved by conservative management. On the other hand, a ganglion cyst is rarely encountered within the cavity of the knee joint and the prevalence of intraarticular ganglion was reported to be 0.2%-1.3% on knee magnetic resonance imaging [1-3]. A ganglion may be asymptomatic, but can also cause considerable morbidity and present with pain or mechanical symptoms. The main treatment for patellar partita and ganglion of the knee joint is surgical excision. Here we report a case of knee pain caused by bipartite patella associated complicated with an intraarticular ganglion.Case Report
A 29-year-old man has had right knee pain since junior high school. The pain usually occurred while climbing stairs or doing hard exercise. Marked exacerbation of his knee pain suddenly occurred 2 months ago. For one week, his pain had been exacerbated by knee motion and while walking. He could not flex and extend his left knee completely. The Marked exacerbation of the symptoms had appeared twice in a month, but he could perform normal activities easily when symptoms were absent. There was no history of trauma to the knee. The symptoms had resolved when he presented to hospital.Physical examination revealed no knee effusion, quadriceps atrophy, or joint line tenderness. Tenderness and percussion pain were present in superolateral portion of the patella. The patella compression test was positive. The range of motion was full. The results of Lachman’s test, the anterior drawer test, and the posterior drawer test were normal. McMurray’s test did not cause pain or a clicking sound. The knee pain was reproduced on forced knee extension and flexion.
Radiographs showed bipartite patella affecting the superolateral portion of the patella. CT showed unhealed fragment of bipartite patella.
Magnetic resonance imaging revealed oedema and bone cyst within the bipartite fragment. And magnetic resonance imaging revealed oval well-demarcated cystic mass (15 mm × 15 mm × 24 mm) anterior to the proximal third of the PCL, with the ligament being flattened and deformed by the mass. The ACL was compressed laterally and deformed too. The mass showed low signal intensity on T1-weighted images (Figure 1A), while it had a uniform high signal intensity on T-2 weighted images (Figure 1B).
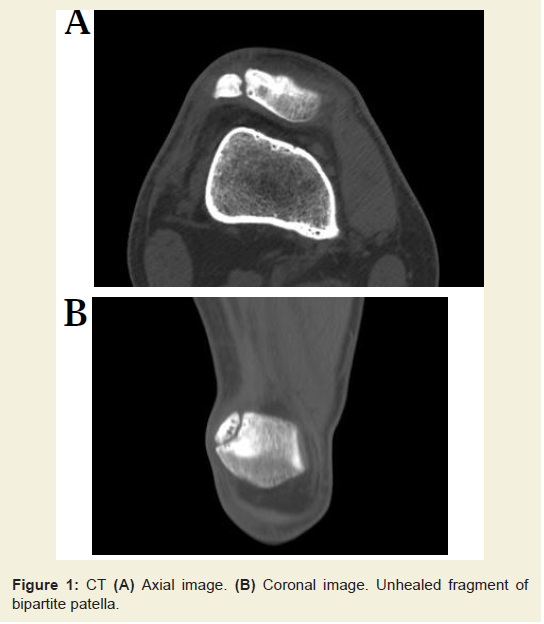
Figure 1: CT (A) Axial image. (B) Coronal image. Unhealed fragment ofbipartite patella.
Pathological examination revealed cystic spaces with walls composed of collagen fibers without an epithelial lining, findings consistent with a ganglion cyst.
His pain on knee motion disappeared after surgery. The patient was asymptomatic and displayed a full range of knee motion when reviewed 12 months postoperatively.
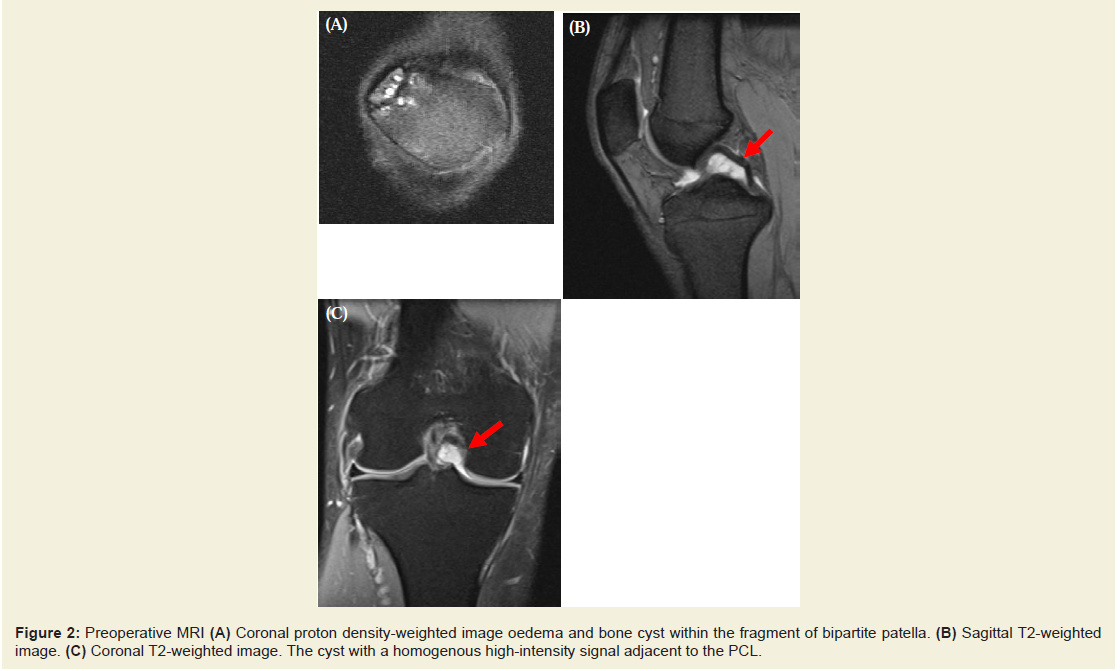
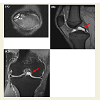
Figure 2: Preoperative MRI (A) Coronal proton density-weighted image oedema and bone cyst within the fragment of bipartite patella. (B) Sagittal T2-weighted image. (C) Coronal T2-weighted image. The cyst with a homogenous high-intensity signal adjacent to the PCL.

Figure 3: Arthroscopic view from an anterolateral portal. Intraoperative view of the ganglion located between the ACL and PCL.
Discussion
Patella partita is known as a developmental anomaly of ossification. The incidence of bipartite patella has been reported to be 0.2-1.7% [4-7], but only 1-2% of these anomalies are symptomatic [8]. Weaver reported two characteristic modes of symptom onset, which were gradual onset during sporting activities or sudden onset after an injury [8]. Symptomatic bipartite patella is observed in young athletes who participate in strenuous sports. The most common symptom is pain at the separated fragments during sporting activities. In adults, bipartite patella occasionally becomes symptomatic following a minor injury. However, our patient had no history of trauma. His symptoms were vague pain and limitation of ROM. We hypothesize that the pain and restriction of motion were not only caused by the bipartite patellae, but also by impingement of his ganglion cysts between the ACL and PCL.The prevalence of intraarticular cystic knee masses (mostly as incidental findings) was reported to be up to 1.3% on MRI and 0.6% by arthroscopy [1-3,9]. Ganglion cysts of the cruciate ligaments not only expand outward along the fibers (anterior to the ACL and posterior to the PCL), but also expand between the two cruciate ligaments (inter-cruciate distension) and are sometimes interspersed within the fibers [3,10-13]. Symptoms and signs that can be caused by an intraarticular ganglion cyst include pain, swelling, joint line tenderness, a positive meniscus injury sign, and limitation of the range of motion [14]. The influence on the range of motion appears to be related to the location of the cyst. Cysts mainly located anterior to the cruciate ligaments tend to limit extension of the knee, whereas those mainly located posterior to the cruciate ligaments tend to limit knee flexion [2,15,16]. However, the limitation of motion cannot be completely explained by the location of the cyst alone. Kim suggested that changes in the shape and dimension of the ganglion cyst with knee motion and posture stimulated nerve endings in the stretched synovial membrane, thereby provoking knee pain and limiting flexion and extension [17]. In this case, the symptoms had appeared twice in a month, but he could perform normal activities easily when symptoms were absent. The reason of this phenomenon cannot be explained by the location of the cyst and changes in the shape and dimension of the cyst. We considered the symptoms were caused by impingement of ganglion cysts between the ACL and PCL.
Our patient had two types of pain, with one being the usual pain on stair climbing that is caused by bipartite patella and the other being sudden vague pain that interfered with ADL. We hypothesize that the first type of pain was caused by his bipartite patella, while the vague pain and limitation of motion were due to impingement of ganglion cysts between the ACL and PCL. The pain and limitation of knee motion caused by the ganglion cysts seemed to be relatively more severe than that due to the patellar deformity.
References
- Bui-Mansfield LT, Youngberg RA (1997) Intraarticular ganglion of the knee: prevalence, presentation, etiology and management. AJR Am J Roentgenol 168: 123-127.
- Nokes SR, Koonce TW, Montanez J (1994) Ganglion cysts of the cruciate ligaments of the knee: recognition on MR images and CT-guided aspiration. AJR Am J Roentgenol 162: 1503.
- Pawlas R, Szlachta Z (1994) Arthroscopic diagnostics and treatment for cysts of the anterior cruciate ligament. Chir Narzadow Ruchu Ortop Pol 59: 227-230.<
- Bourne MH, Bianco AJ Jr (1990) Bipartite patella in the adolescent: results of surgical excision. J Pediatr Orthop 10: 69-73.
- Green WT Jr (1975) Painful bipartite patellae. A report of three cases. Clin Orthop Relat Res: 197-200.
- Ishkawa H, Sakurai A, Hirata S, Ohno O, Kita K, et al. (1994) Painful bipartite patella in young athletes. The diagnostic value of skyline views taken in squatting position and the results of surgical excision. Clin Orthop Relat Res: 223-228.
- Oohashi Y, Koshino T, Oohashi Y (2010) Clinical features and classification of bipartite or tripartite patella. Knee Surg Sports Traumatol Arthrosc 18: 1465-1469.
- Weaver JK (1977) Bipartite patellae as a cause of disability in athlete. Am J Sports Med 5: 137-143.
- Kang CN, Kim DW, Kim DJ, Kim SJ (1999) Intra-articular ganglion cysts of the knee. Arthroscopy 15: 373-378.
- Deutsch A, Veltri DM, Altchek DW, Potter HG, Warren RF, et al. (1994) Symptomatic intraarticular ganglia of the cruciate ligaments of the knee. Arthroscopy 10: 219-223.
- Garcia A, Hodler J, Vaughn L, Haghighi P, Resnick D (1991) Case report 677. Intraarticular ganglion arising from the posterior cruciate-ligament. Skeletal Radiol 20: 373-375.
- Girgis FG, Marchall JL, Monajem A (1975) The cruciate ligaments of the knee joint. Anatomical, functional and experimental analysis. Clin Orthop Relat Res: 216-231.
- Sevilla CA (1996) Ganglion of the anterior cruciate ligament presented as a knee mass. Am J Orthop (Belle Mead NJ) 25: 46-48.
- Krudwig WK, Schulte KK, Heinemann C (2004) Intra-articular ganglion cysts of the knee joint: a report of 85 cases and review of the literature. Knee Surg Sports Traumatol Arthrosc 12: 123-129.
- Muckle DS, Monahan P (1972) Intra-articular ganglion of the knee: report of two cases. J Bone Joint Surg Br 54: 520-521.
- Sumen Y, Ochi M, Deie M, Adachi N, Ikuta Y (1999) Ganglion cysts of the cruciate ligaments detected by MRI. Int Orthop 23: 58-60.
- Kim RS, Kim KT, Lee JY, Lee KY (2003) Ganglion cysts of the posterior cruciate ligament. Arthroscopy 19: E36-E40.