
It is rare for the talonavicular joint to dislocate entirely without the subtalar joint dislocating or the tarsal bones collapsing. Despite being a rare injury, favorable long-term outcome can be achieved with CT CT-based better assessment and closed management.
Dr. Nilesh S Sakharkar, Department of Orthopaedics, Government Medical College and Hospital, Nagpur - 440 003, Maharashtra, India. E-mail: orthodrnilesh@gmail.com
Introduction: Medial swivel type of talonavicular dislocation is a very rare injury; caused by high-velocity trauma. This injury occurs due to forceful adduction of the forefoot without inversion of the foot; causing talonavicular joint to dislocate medially while calcaneum swivels under the talus with intact talocalcaneal interosseous ligament and calcaneocuboid joint.
Case Report: We report a case of 38-year-old male who had medial swivel injury to his right foot, sustaining a high-velocity road traffic accident with no other injuries.
Conclusion: The occurrences, features, reduction maneuver, and follow-up protocol of medial swivel dislocation rare injury have been presented. Even though it is a rare injury, good outcomes are still achievable with proper evaluation and treatment.
Keywords: Medial swivel dislocation, talonavicular joint, subtalar subluxation.
Midtarsal dislocations of the foot and ankle are very rare injuries and occur mainly due to the high-energy trauma. Incidence is estimated to be around 3.6/100,000/year [1]. Strong tendinous and ligamentous structures surrounding the bony components of the midfoot account for fracture-disclocations rather than pure dislocations [2]. Main and Jowett gave the classification for midtarsal injuries depending on the mechanism of injury [3]. Swivel type of injury refers to an isolated dislocation of the talonavicular joint with calcaneum getting swiveled beneath the talus, that is, subtalar subluxation, with intact introsseous ligament and intact calcaneocuboid joint [3, 4, 5, 6]. These injuries are very rare and occur due to severe adduction or abduction of the forefoot with the axis being an intact introsseous ligament [3]. We report a case of medial swivel dislocation of talonavicular joint without associated fracture caused by high-energy trauma causing severe adduction of forefoot, its management, and its follow-up.
A 38-year-old male patient presented to the emergency department with history of high-energy road traffic accident, with injury to his right foot. He had pain and swelling over the medial aspect of the foot with being unable to bear weight and with typical equinovarus deformity. Neurovascular deficit was not found. He denied of any medical history of diabetes mellitus, inflammatory arthropathy, or any other medications. Routine radiographs of the ankle and foot in anteroposterior, lateral, and oblique views were taken which showed medial dislocation of the talonavicular joint with subtalar subluxation without any associated fracture (Fig. 1).  Radiographs did not show any evidence of Charcot or inflammatory arthritis. CT scan was done which showed intact calcaneocuboid joint with no fracture; and subluxated subtalar joint with medial dislocation of the talonavicular joint (Fig. 2).
Radiographs did not show any evidence of Charcot or inflammatory arthritis. CT scan was done which showed intact calcaneocuboid joint with no fracture; and subluxated subtalar joint with medial dislocation of the talonavicular joint (Fig. 2). 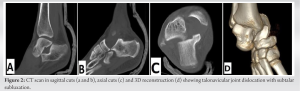 Under spinal anesthesia, close reduction was attempted by flexing the knee joint so as to relax the gastrosoleus complex, with ankle in maximum plantar flexion and axial traction given to the calcaneum with counter traction at knee joint. Deformity was first exaggerated by adducting the forefoot and then reduction attempted by forceful abduction of the forefoot and simultaneous medial pressure applied to the head of the talus and lateral pressure over the dislocated navicular; maintaining the traction and counter traction (Fig. 3).
Under spinal anesthesia, close reduction was attempted by flexing the knee joint so as to relax the gastrosoleus complex, with ankle in maximum plantar flexion and axial traction given to the calcaneum with counter traction at knee joint. Deformity was first exaggerated by adducting the forefoot and then reduction attempted by forceful abduction of the forefoot and simultaneous medial pressure applied to the head of the talus and lateral pressure over the dislocated navicular; maintaining the traction and counter traction (Fig. 3). 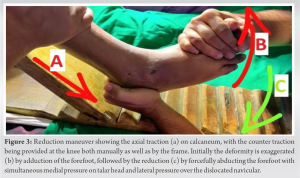 Successful reduction was appreciated by the click with correction of the deformity and confirmed under the image intensifier (Fig. 4).
Successful reduction was appreciated by the click with correction of the deformity and confirmed under the image intensifier (Fig. 4).  During the stress examination, the reduction was maintained; thus, no internal fixation was attempted and the leg was immobilized in below knee cast for 4 weeks (Fig. 5).
During the stress examination, the reduction was maintained; thus, no internal fixation was attempted and the leg was immobilized in below knee cast for 4 weeks (Fig. 5). 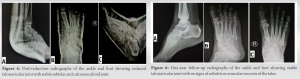 After 4 weeks, the cast was removed and stability was again checked on stress views. Found to be stable, physiotherapy of the ankle and subtalar joint was initiated with partial weight-bearing. After 6 weeks post-trauma, full-weight-bearing was started. At 1 year follow-up, the patient had full range of motion with no radiological evidence of instability, arthritis, or avascular necrosis (Fig. 6).
After 4 weeks, the cast was removed and stability was again checked on stress views. Found to be stable, physiotherapy of the ankle and subtalar joint was initiated with partial weight-bearing. After 6 weeks post-trauma, full-weight-bearing was started. At 1 year follow-up, the patient had full range of motion with no radiological evidence of instability, arthritis, or avascular necrosis (Fig. 6).
The midtarsal joints include the talonavicular and calcaneocuboid joints lying in a transverse plane. Main and Jowett [3] gave the classification for the midtarsal injuries depending on the mechanism of injury and displacement [3, 7]. Medial and lateral injuries were further classified as fracture, sprain, fracture-subluxation/dislocation, and swivel dislocation (Table 1). The incidence of swivel injuries in their series was found to be 12% [3]; with medial being more common and easier to reduce than the lateral counterpart. Lateral injuries are found to be associated with the impacted fracture of the calcaneocuboid joint (nut cracker fracture) [8]. Swivel injuries differ from subtalar injuries as the deforming forces act more anteriorly in the former [7, 8]. Ip and Lui suggested that concomitant ligamentous injuries carry worse prognosis than pure dislocations [9]. Swivel injuries as a whole are more easy than dorsal or subtalar dislocations due to disruption of tough ligamentous structures and loss of plantar ligament integrity in the later [10, 11]. Early diagnosis and prompt treatment helps to minimize difficult reduction, compartment syndrome, avascular necrosis of the talus, and post-traumatic arthritis [12]. Our case was a medial swivel dislocation of TNJ without any fracture. It is important to distinguish between the medial swivel injury and medial subtalar dislocation. Medial subtalar dislocation is reduced by traction and eversion of the ankle, while medial swivel dislocation reduces by traction and abduction of the forefoot with simultaneous lateral pressure over the head of the talus. Obstruction to close reduce subtalar dislocation can be due to interposition of the tendon of tibialis posterior or interlocking or impaction of the fracture fragment of talus or navicular, which is not seen in swivel injuries, while causes of failure to close reduce swivel injuries include: 1) Buttonholing of the talar head through the extensor retinaculum or extensor digitorium brevis or talonavicular ligament or joint capsule and 2) interposition of extensor digitorium brevis or deep peroneal nerve or dorsalis pedis artery or fracture fragments between the talus and navicular [13, 14]. Various treatment modalities have been advocated by the authors which include: (1) closed reduction without internal fixation, (2) closed reduction with internal fixation, (3) open reduction with internal or external fixation, and (4) amputation. However, multiple attempts for closed reduction can compromise the surrounding soft-tissue structures and can lead to necrosis [13]. Thus, most of the authors have advocated the use of open reduction and internal fixation so as to prevent the risk of vascular compromise [10, 15, 16, 17]. Richter et al. advocate open reduction and internal fixation for all dislocations of TNJ to prevent the risk of vascular compromise [17]. Main and Jowett recommended closed reduction with or without k-wire fixation and immobilization for medial swivel injuries [3]. Williams et al. recommended closed reduction without internal fixation in a single case report of medial swivel injury due to low energy trauma [18]. Pehlivan et al. reported a single case of medial swivel injury managed with open reduction and percutaneous fixation with small residual functional deficit and lateral column pain only on long distance ambulation; on long-term follow-up [19]. Some early complications include: (1) skin necrosis, (2) neurovascular deficit, and (3) compartment syndrome. These complications are found in 0–10% of cases [20]. Some late complications include: (1) avascular necrosis of the talus, (2) osteoporosis, and (3) post-traumatic arthritis. Early diagnosis and prompt intervention help in preventing these complications. Furthermore, keeping the foot in non-weigh-bearing is essential for good outcomes whether closed or open reduced [4, 18, 21].
Talonavicular dislocation of swivel type is a rare injury; caused by high-energy trauma. Our case had medial swivel injury due to high-velocity trauma without associated fracture and was able to reduce it in a closed manner with the reduction maintained in stress views, and was thus not fixed internally and was immobilized. We recommend an attempt of closed reduction to have an anatomic reduction, failing to which open reduction should be attempted with or without internal fixation. The present case was reported due to its rarity and also because the dislocation was reduced by closed means with excellent outcomes.
For an accurate diagnosis and treatment planning, a CT-based examination is needed. If a diagnosis is made early, closed reduction is the treatment that might be done. Relative longer time of immobilization requires for ligaments to heal.
References
- 1.Van Dorp KB, De Vries MR, Van der Elst M, Schepers T. Chopart joint injury: A study of outcome and morbidity. J Foot Ankle Surg 2010;49:541-5. [Google Scholar]
- 2.Ross PM, Mitchell DC. Dislocation of the talonavicular joint: Case report. J Trauma 1976;16:397-401. [Google Scholar]
- 3.Main BJ, Jowett RL. Injuries of the midtarsal joint. J Bone Joint Surg Br 1975;57:89-97. [Google Scholar]
- 4.Powell E, LaBella M. Swivel-type dislocation of the talonavicular Joint: A case report. Foot Ankle Online J 2011;4:3. [Google Scholar]
- 5.Inal S, Inal C. An unusual variety of simultaneous fracture dislocation pattern: Medial swivel dislocation of talonavicular joint with displaced fractures of the fourth and fifth metatarsals. J Foot Ankle Surg 2013;52:501-4. [Google Scholar]
- 6.Datt N, Rao AS, Rao DV. Medial swivel dislocation of the talonavicular joint. Indian J Orthop 2009;43:87-9. [Google Scholar]
- 7.Rockwood CA, Green DP, Bucholz RW, Heckman JD. Fractures in Adults. 5th ed., Vol. 2. Philadelphia, PA: Lippincott Williams and Wilkins; 2000 . p. 2124-5. [Google Scholar]
- 8.Pillai A, Chakrabarti D, Hadidi M. Lateral swivel dislocation of the talonavicular joint. Foot Ankle Surg 2006;12:39-41. [Google Scholar]
- 9.Samolada E, Fotiades H, Christoforides J, Pournaras J. Talonavicular dislocation and nondisplaced fracture of the navicular. Arch Orthop Trauma Surg 2005;125:59-61. [Google Scholar]
- 10.Miller CM, Winter WG, Bucknell AL, Jonassen EA. Injuries to the midtarsal joint and lesser tarsal bones. J Am Acad Orthop Surg 1998;6:249-58. [Google Scholar]
- 11.Ip KY, Lui TH. Isolated dorsal midtarsal (Chopart) dislocation: A case report. J Orthop Surg (Hong Kong) 2006;14:357-9. [Google Scholar]
- 12.Gaddy B, Perry CR. Chopart dislocation: A case report. J Orthop Trauma 1993;7:388-90 [Google Scholar]
- 13.Ricci WM, Bellabarba C, Sanders R. Transcalcaneal talonavicular dislocation. J Bone Joint Surg Am 2002;84:557-61. [Google Scholar]
- 14.Tucker DJ, Burian G, Boylan JP. Lateral subtalar dislocation: Review of the literature and case presentation. J Foot Ankle Surg 1998;37:239-62. [Google Scholar]
- 15.Richter M, Thermann H, Huefner T, Schmidt U, Goesling T, Krettek C. Chopart joint fracture-dislocation: Initial Open reduction provides better outcome than closed reduction. Foot Ankle Int 2004;25:340-8. [Google Scholar]
- 16.Garofalo R, Moretti B, Ortolano V, Cariola P, Solarino G, Wettstein M, et al. Peritalar dislocations: A retrospective study of 18 cases. J Foot Ankle Surg 2004;43:166-72. [Google Scholar]
- 17.Richter M, Wippermann B, Krettek C Schratt HE, Hufner T, Thermann H. Fractures and fracture dislocations of the midfoot: Occurrence, causes and long-term results. Foot Ankle Int 2001;22:392-8. [Google Scholar]
- 18.Williams DP, Hanoun A, Hakimi M, Ali S, Khatri M. Talonavicular dislocation with associated cuboid fracture following low-energy trauma. Foot Ankle Surg 2009;15:155-7. [Google Scholar]
- 19.Pehlivan O, Akmaz I, Solakoglu C, Rodop O. Medial peritalar dislocation. Arch Orthop Trauma Surg 2002;122:541-3. [Google Scholar]
- 20.Kotter A, Wieberneit J, Braun W, Rüter A. The Chopart dislocation. A frequently underestimated injury and its sequelae. A clinical study. Unfallchirurg 1997;100:737-41. [Google Scholar]
- 21.Bosman WM, Prakken FJ, Pijls BG, Ritchie ED. Lateral talonavicular dislocation after low-energy trauma. BMJ Case Rep 2013;2013:bcr210200692. [Google Scholar]








