Suicide is a national public health concern that affects thousands of US individuals and families, with repercussions that reverberate through entire communities. In 2019, there were 47,500 US deaths by suicide, which accounted for about 1 death every 11 minutes.1 Suicide remains the tenth leading cause of death in the United States and has been part of the top 12 leading causes of death since 1975.2 Unfortunately, this trend has worsened; suicide rates have increased by 35% from 1999 to 2018.3 One particularly vulnerable population is US veterans who accounted for 13.8% of all suicide deaths in 2018.4 Among veterans, the suicide death average increased from 16.6 per day in 2005 to 17.6 in 2018.4 Furthermore, veterans experiencing homelessness are 5 times more likely to attempt suicide and 2.5 times more likely to have suicidal ideation compared with veterans without a history of homelessness.4 Suicide is a significant issue among veterans experiencing homelessness: Veterans account for about 11% of the overall US homeless population.5
Recent data suggest opportunities for suicide risk assessment in the primary care setting. A study from the Veterans Health Administration (VHA) Office for Suicide Prevention found that in 2014 an average of 20 veterans died by suicide every day and 6 of the 20 (30%) on average used VHA services within the prior year.6 Similarly, a review of 40 studies on suicide found that 45% of suicide victims had contact with their primary care practitioner (PCP) within 1 month of suicide, and 75% of victims had contact within the year of suicide.7 An analysis of depression screening in 2008/2009 using Patient Health Questionnaire-2 (PHQ-2) or Patient Health Questionnaire-9 (PHQ-9) at 3 large western US Department of Veterans Affairs (VA) medical centers found that 55% were screened for depression.8 The VA has made suicide prevention a top priority and supports the established US goal of reducing annual suicide deaths by 20% by 2025.9 Given key opportunities for suicide risk assessment in the primary care setting, the VHA Office of Mental Health and Suicide Prevention implemented a national, standardized process for suicide risk assessment on October 1, 2018.10,11
The VA approach to suicide screening, evaluation, and documentation has evolved over time. Between October 2018 and December 2020, the process was augmented to include 3 stages embedded into the electronic health record (EHR): a primary screen (PHQ-2 with Item 9 from the PHQ-9 [PHQ-2+I9]), a secondary screen (Columbia-Suicide Severity Rating Scale [C-SSRS]), and a tertiary screen (Comprehensive Suicide Risk Evaluation [CSRE]). The primary screen consisted of the depression screening using the PHQ-2 with the addition of I9 asking about suicidal ideation. The secondary screening, or C-SSRS, included 8 questions to elaborate on suicidal ideation, intent, plan, and any history of suicidal attempts or preparatory behaviors. The tertiary screen consisted of the CSRE, a questionnaire developed internally by the VA in 2018 to further evaluate the veteran’s suicidal thoughts, attempts, warning signs, risk factors, protective factors, and reasons for living. The goal of the screenings was to identify veterans at risk of suicide, assess risk severity, and to individually tailor risk mitigation strategies for safe disposition. These risk categories were developed by the regional Mental Illness Research, Education and Clinical Center, which suggested treatment strategies, such as hospitalization or close outpatient follow-up.12,13
The Homeless Patient Aligned Care Team (HPACT) clinic at the West Los Angeles VA Medical Center (WLAVAMC) in California, one of the largest VA homeless clinics in the country and 1 of 7 national VA Office of Academic Affiliation Centers of Excellence in Primary Care Education training programs implemented the standardized tools for suicide risk screening and quality improvement (QI). The HPACT clinic is an interprofessional team, including primary care, mental health, social work, pharmacy, and peer support, that is adjacent to the WLAVAMC general primary care clinics. The team collaboratively addresses both medical and psychosocial needs of veterans with a focus on the Housing First Model, an approach that prioritizes ending homelessness while addressing all factors associated with veterans' health and well-being. After 1 year of stable housing, veterans graduate to the WLAVAMC general primary care clinics.
Given the vulnerability of veterans experiencing homelessness, the clinic leadership identified suicide risk screening as a high priority initiative and created a taskforce to oversee effective implementation of clinic screening efforts. An interprofessional team of nurse practitioners (NPs), pharmacists, physicians, psychologists, social workers (SWs), and trainees formed to improve screening efforts and use the QI principles to guide analysis and intervention. The team wrote the following SMART (Specific, Measurable, Achievable, Relevant, and Time-bound) Aim statements: (1) ensure > 90% of eligible patients receive a primary screen; (2) ensure > 90% of positive primary I9 screens receive subsequent screenings within 24 hours; and (3) increase staff comfort and familiarity using the screening tools. This article examines the results of the screening initiative 1-year postimplementation, describes difficulties faced, and suggests strategies that might be used to overcome those challenges.
Methods
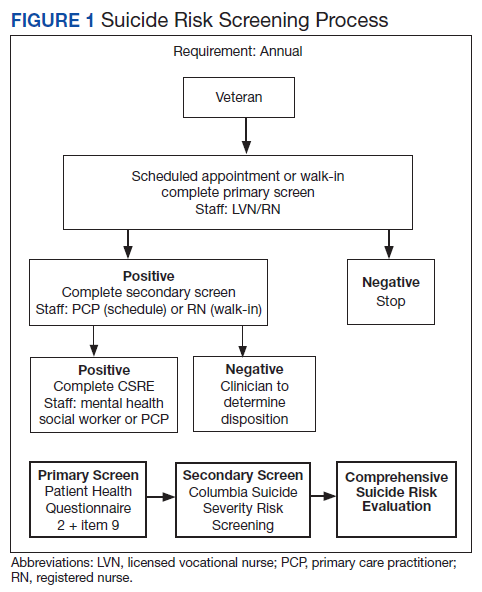
This QI analysis was exempt from institutional review board review. Prior to the standardized national suicide risk assessment rollout of October 1, 2018, the QI team met to review and understand the workflow to be implemented into the HPACT clinic. To describe the initial screening process, the new suicide risk assessment consisted of primary, secondary, and tertiary screens that would warrant subsequent intervention by clinicians if positive (Figure 1). The primary screen included the PHQ-2+I9 questionnaire (PHQ-2 for depression and I9 for suicidal ideation). If either were positive, follow-up questionnaires were required. Of note, patients with a prior depression diagnosis, cognitive impairment defined at a severity of moderate or greater based on clinician evaluation and judgement, or life expectancy < 6 months were exempt from screening because, by definition, they had theoretically already been screened and classified as under surveillance.
A positive I9 response prompted a secondary screen using C-SSRS. A positive secondary screen prompted a tertiary screen using CSRE. If the PHQ-2 screening was positive but I9 was negative, the standard follow-up depression clinical reminder was used. Any clinical staff member could perform the primary screen, including licensed vocational nurses (LVNs), registered nurses (RNs), and SWs in any setting (eg, emergency department, primary care, inpatient services). The secondary and tertiary screens required completion by a licensed clinician. RNs were able to perform the secondary screen but not the tertiary screen.
The HPACT clinic serves approximately 3000 patients by 50 staff and trainees divided into 2 teams. LVNs and RNs were tasked to conduct the primary screen as part of their initial clinic check-in. If the primary screen was positive for scheduled patients, LVNs notified a PCP to complete the secondary screen. For unscheduled patients, RNs conducted a primary screen and, if positive, a secondary screen. If the secondary screen was positive, a tertiary screen was performed by mental health practitioners or SWs, or PCPs if the former were unavailable. SWs, mental health practitioners, and PCPs were colocated in the clinic, which allowed for safe and convenient warm handoffs between clinicians.