
Abstract
Background
Malnutrition commonly affects patients with esophageal cancer and has the potential to negatively influence treatment outcomes. The aim of this study was to investigate the impact of early (preoperative) jejunostomy tube feeding (JTF) in nutritionally ‘high risk’ patients receiving multimodal therapy for esophageal cancer.
Methods
Patients were selected to undergo early JTF during neoadjuvant chemoradiotherapy (nCRT) in accordance with European Society for Clinical Nutrition and Metabolism (ESPEN) and Enhanced Recovery after Surgery (ERAS®) Society guidelines. Clinical outcomes were compared with patients who received routine JTF from the time of esophagectomy. Body composition was determined from computed tomography (CT) images acquired at diagnosis, after nCRT, and ≥ 3 months after surgery.
Results
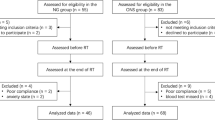
In total, 81 patients received early JTF and 91 patients received routine JTF. Patients who received early JTF had lower body mass index (BMI; 26.1 ± 4.6 vs. 28.4 ± 4.9; p = 0.002), greater weight loss, and worse performance status at diagnosis. Groups were otherwise well-matched for baseline characteristics. Rate of re-intubation (8.8% vs. 1.1%; p = 0.027), pulmonary embolism (5.0% vs. 0.0%; p = 0.046), and 90-day mortality (10.0% vs. 1.1%; p = 0.010) were worse in the early JTF group; however, overall survival was equivalent for both the early and routine JTF groups (p = 0.053). Wide variation in the degree of preoperative muscle loss and total adipose tissue loss was observed across the entire study cohort. Relative preoperative muscle and adipose tissue loss in patients with early and routine JTF was equivalent.
Conclusions
In patients determined to be at ‘high risk’ of malnutrition, early JTF may prevent excess morbidity after esophagectomy with an associated relative preservation of parameters of body composition.



Similar content being viewed by others


References
Anandavadivelan P, Lagergren P. Cachexia in patients with oesophageal cancer. Nat Rev Clin Oncol. 2016;13(3):185–98.
Elliott JA, Doyle SL, Murphy CF, et al. Sarcopenia: prevalence, and impact on operative and oncologic outcomes in the multimodal management of locally advanced esophageal cancer. Ann Surg. 2017;266(5):822–30.
Low DE, Allum W, De Manzoni G, et al. Guidelines for perioperative care in esophagectomy: enhanced recovery after surgery (ERAS) society recommendations. World J Surg. 2019;43(2):299–330.
Weimann A, Braga M, Carli F, et al. ESPEN guideline: Clinical nutrition in surgery. Clin Nutr. 2017;36(3):623–50.
Mueller C, Compher C, Ellen DM, American Society for Parenteral and Enteral Nutrition Board of Directors. A.S.P.E.N. clinical guidelines: Nutrition screening, assessment, and intervention in adults. JPEN J Parenter Enteral Nutr. Jan 2011;35(1):16-24.
Markar SR, Karthikesalingam A, Low DE. Enhanced recovery pathways lead to an improvement in postoperative outcomes following esophagectomy: Systematic review and pooled analysis. Dis Esophagus. 2015;28(5):468–75.
Low DE, Alderson D, Cecconello I, et al. International consensus on standardization of data collection for complications associated with Esophagectomy: Esophagectomy Complications Consensus Group (ECCG). Ann Surg. 2015;262(2):286–94.
Prado CM, Lieffers JR, McCargar LJ, et al. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: A population-based study. Lancet Oncol. 2008;9(7):629–35.
Tsujimoto H, Hiraki S, Takahata R, et al. Laparoscopic jejunostomy for obstructing upper gastrointestinal malignancies. Mol Clin Oncol. 2015;3(6):1307–10.
Ben-David K, Kim T, Caban AM, Rossidis G, Rodriguez SS, Hochwald SN. Pre-therapy laparoscopic feeding jejunostomy is safe and effective in patients undergoing minimally invasive esophagectomy for cancer. J Gastrointest Surg. 2013;17(8):1352–8.
Jenkinson AD, Lim J, Agrawal N, Menzies D. Laparoscopic feeding jejunostomy in esophagogastric cancer. Surg Endosc. 2007;21(2):299–302.
Cespedes Feliciano EM, Kroenke CH, Meyerhardt JA, et al. Association of systemic inflammation and sarcopenia with survival in nonmetastatic colorectal cancer: Results from the C SCANS study. JAMA Oncol. 2017;3(12):e172319.
Ebadi M, Martin L, Ghosh S, et al. Subcutaneous adiposity is an independent predictor of mortality in cancer patients. Br J Cancer. 2017;117(1):148–55.
Palmela C, Velho S, Agostinho L, et al. Body composition as a prognostic factor of neoadjuvant chemotherapy toxicity and outcome in patients with locally advanced gastric cancer. J Gastric Cancer. 2017;17(1):74–87.
Rangel EL, Rios-Diaz AJ, Uyeda JW, et al. Sarcopenia increases risk of long-term mortality in elderly patients undergoing emergency abdominal surgery. J Trauma Acute Care Surg. 2017;83(6):1179–86.
Boshier PR, Heneghan R, Markar SR, Baracos VE, Low DE. Assessment of body composition and sarcopenia in patients with esophageal cancer: A systematic review and meta-analysis. Dis Esophagus. 2018;31(8).
Järvinen T, Ilonen I, Kauppi J, Salo J, Rasanen J. Loss of skeletal muscle mass during neoadjuvant treatments correlates with worse prognosis in esophageal cancer: a retrospective cohort study. World J Surg Oncol. 2018;16(1):27.
Reisinger KW, Bosmans JW, Uittenbogaart M, et al. Loss of skeletal muscle mass during neoadjuvant chemoradiotherapy predicts postoperative mortality in esophageal cancer surgery. Ann Surg Oncol. 2015;22(13):4445–52. https://doi.org/10.1245/s10434-015-4558-4.
Paireder M, Asari R, Kristo I, et al. Impact of sarcopenia on outcome in patients with esophageal resection following neoadjuvant chemotherapy for esophageal cancer. Eur J Surg Oncol. 2017;43(2):478–84.
Yip C, Goh V, Davies A, et al. Assessment of sarcopenia and changes in body composition after neoadjuvant chemotherapy and associations with clinical outcomes in oesophageal cancer. Eur Radiol. 2014;24(5):998–1005.
Acknowledgments
The authors are grateful to Abha Dunichand-Hoedl, Technologist at the University of Alberta, for support in the analysis of CT images using Slice-O-matic. This study was partly funded through a Wilske Pioneer Award from the Benaroya Research Institute (Virginia Mason Medical Center) and National Institute for Health and Care Research (NIHR) Imperial Biomedical Research Centre (Imperial College London). PB is the recipient of the 2017 Joint Royal College of Surgeons (England)/Ryan Hill Research Fellowship and is an NIHR Clinical Lecturer at Imperial College London. FK is the recipient of the 2018 Ryan Hill Research Fellowship, and FP is the recipient of the 2019 Ryan Hill Research Fellowship.
Funding
NIHR Imperial Biomedical Research Centre and Benaroya Research Institute.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Piers R. Boshier, Fredrik Klevebro, Amy Schmidt, Shiwei Han, Wesley Jenq, Francesco Puccetti, Maarten F.J. Seesing, Vickie E. Baracos, and Donald E. Low have no commercial interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Boshier, P.R., Klevebro, F., Schmidt, A. et al. Impact of Early Jejunostomy Tube Feeding on Clinical Outcome and Parameters of Body Composition in Esophageal Cancer Patients Receiving Multimodal Therapy. Ann Surg Oncol 29, 5689–5697 (2022). https://doi.org/10.1245/s10434-022-11754-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-022-11754-3