
Abstract
Background
During the last two decades, significant advancements in the treatment of laryngeal cancer have occurred. Although survival of head and neck cancer patients has improved over time, the temporal trend of laryngeal cancer survival is an area of controversy.
Methods
From 2004 to 2016, 77,527 patients who had laryngeal cancer treated with curative intent in the United States were identified in the National Cancer Database. Relative and observed survival rates were assessed for temporal trends. Multinomial logistic regression investigated the relationship between American Joint Committee on Cancer (AJCC) stage and increasing calendar year.
Results
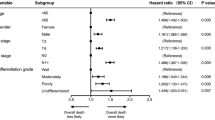
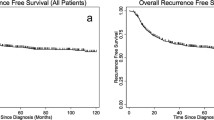
No significant improvement in 2- or 5-year observed survival (OS) or relative survival (RS) was observed. The 5-year RS ranged from 61.72 to 63.97%, and the 5-year OS ranged from 54.26 to 56.52%. With each increasing year, the proportion of stage 4 disease increased, with risk for stage 4 disease at the time of diagnosis increasing 2.2% annually (adjusted odds ratio [aOR], 1.022; 95% confidence interval [CI], 1.017–1.028; p < 0.001). This increase was driven by a 4.7% yearly increase in N2 disease (aOR, 1.047; 95% CI, 1.041–1.053; p < 0.001), with an annual 1.2% increase in T3 disease (aOR, 1.012; 95% CI, 1.007–1.018; p < 0.001) and a 1.2% increase in T4 disease (aOR, 1.012; 95% CI, 1.005–1.018; p < 0.001).
Conclusion
Despite advances in the field, laryngeal cancer survival in the United States is not improving over time. This may be due to an increase in the proportion of stage 4 disease, driven primarily by increasing nodal disease. To achieve survival improvement commensurate with scientific and technologic advances, efforts should be made to diagnose and treat laryngeal cancer at earlier stages to prevent further stage migration.



Similar content being viewed by others

References
Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med. 2003;349:2091–8. https://doi.org/10.1056/NEJMoa031317.
Forastiere AA, Ismaila N, Lewin JS, et al. Use of larynx-preservation strategies in the treatment of laryngeal cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J Clin Oncol. 2017;36:1143–69. https://doi.org/10.1200/JCO.2017.75.7385.
Wolf GT, Bellile E, Eisbruch A, et al. Survival rates using individualized bioselection treatment methods in patients with advanced laryngeal cancer. JAMA Otolaryngol Neck Surg. 2017;143:355–66.
Susko MS, Lazar AA, Dhar S, et al. Improved tumor control related to radiotherapy technological development for hypopharyngeal cancer. Laryngoscope. 2021;131:E452–8. https://doi.org/10.1002/lary.28726.
Daly ME, Le Q-T, Jain AK, et al. Intensity-modulated radiotherapy for locally advanced cancers of the larynx and hypopharynx. Head Neck. 2011;33:103–11. https://doi.org/10.1002/hed.21406.
Kouloulias V, Thalassinou S, Platoni K, et al. The treatment outcome and radiation-induced toxicity for patients with head and neck carcinoma in the IMRT era: a systematic review with dosimetric and clinical parameters. Biomed Res Int. 2013;2013:401261. https://doi.org/10.1155/2013/401261.
Ozer E, Alvarez B, Kakarala K, Durmus K, Teknos TN, Carrau RL. Clinical outcomes of transoral robotic supraglottic laryngectomy. Head Neck. 2013;35:1158–61. https://doi.org/10.1002/hed.23101.
Dziegielewski PT, Kang SY, Ozer E. Transoral robotic surgery (TORS) for laryngeal and hypopharyngeal cancers. J Surg Oncol. 2015;112:702–6. https://doi.org/10.1002/jso.24002.
Forastiere AA, Maor M, Weber RS, et al. Long-term results of Intergroup RTOG 91–11: a phase III trial to preserve the larynx-induction cisplatin/5-FU and radiation therapy versus concurrent cisplatin and radiation therapy versus radiation therapy. J Clin Oncol. 2006;24(18 Suppl):5517. https://doi.org/10.1200/jco.2006.24.18_suppl.5517.
Hoffman HT, Porter K, Karnell LH, et al. Laryngeal cancer in the United States: changes in demographics, patterns of care, and survival. Laryngoscope. 2006;116(9 Suppl. 2):1–13. https://doi.org/10.1097/01.mlg.0000236095.97947.26.
Olsen KD. Reexamining the treatment of advanced laryngeal cancer. Head Neck. 2010;32:1–7. https://doi.org/10.1002/hed.21294.
Wolf GT. Reexamining the treatment of advanced laryngeal cancer: the VA laryngeal cancer study revisited. Head Neck. 2010;32:7–14. https://doi.org/10.1002/hed.21296.
Megwalu UC, Sikora AG. Survival outcomes in advanced laryngeal cancer. JAMA Otolaryngol Head Neck Surg. 2014;140:855–60. https://doi.org/10.1001/jamaoto.2014.1671.
Boffa DJ, Rosen JE, Mallin K, et al. Using the National Cancer Database for outcomes research: a review. JAMA Oncol. 2017;3:1722–8. https://doi.org/10.1001/jamaoncol.2016.6905.
Huang SH, O’Sullivan B. Overview of the 8th-edition TNM classification for head and neck cancer. Curr Treat Options Oncol. 2017;18:40. https://doi.org/10.1007/s11864-017-0484-y.
Dickman PW, Hills M. Estimating and modelling relative survival. Stata J. 2013;vv:1–25.
Shah JP, Karnell LH, Huffman HT, et al. Patterns of care for cancer of the larynx in the United States. Arch Otolaryngol Head Neck Surg. 1997;123:475–83. https://doi.org/10.1001/archotol.1997.01900050021002.
Champion GA, Piccirillo JF. The impact of computed tomography on pretherapeutic staging in patients with laryngeal cancer: demonstration of the will Rogers’ phenomenon. Head Neck. 2004;26:972–6. https://doi.org/10.1002/hed.20071.
Hillner BE, Tosteson AN, Song Y, et al. Growth in the use of PET for six cancer types after coverage by Medicare: additive or replacement? J Am Coll Radiol. 2012;9:33–41. https://doi.org/10.1016/j.jacr.2011.06.019.
Tatar G, Cermik TF, Karagoz Y, et al. The value of whole-body contrast-enhanced 18F-FDG PET/CT imaging in the diagnosis and staging of patients with laryngeal carcinoma. Nucl Med Commun. 2018;39:334–42.
Contrera KJ, Hair BB, Prendes B, et al. Clinical versus pathologic laryngeal cancer staging and the impact of stage change on outcomes. Laryngoscope. 2020;131:559–65. https://doi.org/10.1002/lary.28924.
Morgensztern D, Ng SH, Gao F, Govindan R. Trends in stage distribution for patients with non-small cell lung cancer: a National Cancer Database survey. J Thorac Oncol. 2010;5:29–33. https://doi.org/10.1097/JTO.0b013e3181c5920c.
Xiao R, Ward MC, Yang K, et al. Increased pathologic upstaging with rising time to treatment initiation for head and neck cancer: a mechanism for increased mortality. Cancer. 2018;124:1400–14. https://doi.org/10.1002/cncr.31213.
Wasif N, Etzioni D, Habermann EB, et al. Racial and socioeconomic differences in the use of high-volume commission on cancer-accredited hospitals for cancer surgery in the United States. Ann Surg Oncol. 2018;25:1116–25. https://doi.org/10.1245/s10434-018-6374-0.
Kompelli AR, Li H, Neskey DM. Impact of delay in treatment initiation on overall survival in laryngeal cancers. Otolaryngol Neck Surg Off J Am Acad Otolaryngol Neck Surg. 2019;160:651–7. https://doi.org/10.1177/0194599818803330.
Naghavi AO, Echevarria MI, Strom TJ, et al. Treatment delays, race, and outcomes in head and neck cancer. Cancer Epidemiol. 2016;45:18–25. https://doi.org/10.1016/j.canep.2016.09.005.
Mahal BA, Inverso G, Aizer AA, Bruce Donoff R, Chuang S-K. Impact of African-American race on presentation, treatment, and survival of head and neck cancer. Oral Oncol. 2014;50:1177–81. https://doi.org/10.1016/j.oraloncology.2014.09.004.
Ragin CC, Langevin SM, Marzouk M, Grandis J, Taioli E. Determinants of head and neck cancer survival by race. Head Neck. 2011;33:1092–8. https://doi.org/10.1002/hed.21584.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
There are no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Fig. S1
Pathologic N stage distribution. Pathologic N2 disease increased from 2004 through 2013 before decreasing from 2014 to 2016. A similar trend in N1 disease was observed, whereas N0 disease decreased from 2004 through 2015 before increasing in 2016. (TIFF 3387 kb)
Rights and permissions
About this article

Cite this article
Li, M.M., Zhao, S., Eskander, A. et al. Stage Migration and Survival Trends in Laryngeal Cancer. Ann Surg Oncol 28, 7300–7309 (2021). https://doi.org/10.1245/s10434-021-10318-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-021-10318-1