
Abstract
Background
The treatment for papillary thyroid cancer (PTC) has become more conservative, but still no specific guidelines exist for managing isthmic PTC. This study analyzed the outcomes from isthmusectomy in single isthmic PTC and compared it with those for patients who previously had undergone a total thyroidectomy.
Methods
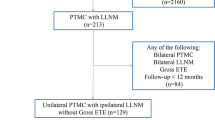
An isthmusectomy with prophylactic central compartment neck dissection (pCCND) was planned for a single isthmic PTC between 2014 and 2018 (isthmusectomy group). For cases with gross extrathyroidal extension (ETE) or multiple nodal metastasis, the procedure was converted to a total thyroidectomy. The study analyzed the characteristics and outcomes of the isthmusectomy group. Additionally, the results were compared with those of the isthmusectomy-feasible group who met the eligibility criteria for isthmusectomy among total thyroidectomies performed between 2009 and 2013.
Results
Of the 90 patients in the isthmusectomy group, 81 received isthmusectomy and 9 had conversion to a total thyroidectomy. Microcarcinoma occurred in 72 cases and gross ETE in 3 cases. One patient showed occult satellite cancer, and seven patients showed more than five metastatic nodes. Transient hypocalcemia developed in five and patients and permanent hypocalcemia in one patient with total thyroidectomy. Of 46 patients who began hormone replacement postoperatively, 13 completely stopped taking medication during the follow-up period. Metachronous PTC was diagnosed for one patient 12 months after isthmusectomy. The isthmusectomy group and the isthmusectomy-feasible group showed similar clinicopathologic properties including multifocality, ETE, and nodal metastasis. However, the isthmusectomy group showed significantly less transient or permanent hypocalcemia and thyroid hormone dependency.
Conclusions
Isthmusectomy with pCCND may be a feasible alternative for properly selected isthmic PTC, resulting in a better quality of life than total thyroidectomy.
Similar content being viewed by others


References
Li G, Lei J, Peng Q, et al. Lymph node metastasis characteristics of papillary thyroid carcinoma located in the isthmus: a single-center analysis. Med Baltim. 2017;96:e7143.
Vasileiadis I, Boutzios G, Karalaki M, Misiakos E, Karatzas T. Papillary thyroid carcinoma of the isthmus: total thyroidectomy or isthmusectomy? Am J Surg. 2018;216:135–9.
Lee YS, Jeong JJ, Nam KH, Chung WY, Chang HS, Park CS. Papillary carcinoma located in the thyroid isthmus. World J Surg. 2010;34:36–9.
Nixon IJ, Palmer FL, Whitcher MM, et al. Thyroid isthmusectomy for well-differentiated thyroid cancer. Ann Surg Oncol. 2011;18:767–70.
Goldfarb M, Rodgers SS, Lew JI. Appropriate surgical procedure for dominant thyroid nodules of the isthmus 1 cm or larger. Arch Surg. 2012;147:881–4.
Mai KT, Gulavita P, Lai C, et al. Topographic distribution of papillary thyroid carcinoma by mapping in coronal sections of 125 consecutive thyroidectomy specimens. Int J Surg Pathol. 2014;22:303–15.
Karatzas T, Charitoudis G, Vasileiadis D, Kapetanakis S, Vasileiadis I. Surgical treatment for dominant malignant nodules of the isthmus of the thyroid gland: a case control study. Int J Surg. 2015;18:64–8.
Huang H, Liu S-Y, Ni S, Zhang Z-M, Wang X-L, Xu Z-G. Treatment outcome of papillary carcinoma confined to the thyroid isthmus. J Cancer Ther. 2016;07:963–9.
Song CM, Lee DW, Ji YB, Jeong JH, Park JH, Tae K. Frequency and pattern of central lymph node metastasis in papillary carcinoma of the thyroid isthmus. Head Neck. 2016;38(Suppl 1):E412–6.
Chang YW, Lee HY, Kim HS, Kim HY, Lee JB, Son GS. Extent of central lymph node dissection for papillary thyroid carcinoma in the isthmus. Ann Surg Treat Res. 2018;94:229–34.
Lei J, Zhu J, Li Z, Gong R, Wei T. Surgical procedures for papillary thyroid carcinoma located in the thyroid isthmus: an intention-to-treat analysis. OncoTargets Targets Ther. 2016;9:5209–16.
Park H, Harries V, McGill MR, Ganly I, Shah JP. Isthmusectomy in selected patients with well-differentiated thyroid carcinoma. Head Neck. 2020;42:43–9.
Haugen BR, Alexander EK, Bible KC, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26:1–133.
Perros P, Boelaert K, Colley S, et al. Guidelines for the management of thyroid cancer. Clin Endocrinol Oxf. 2014;81(Suppl 1):1–122.
Tuttle RM, Haddad RI, Ball DW, et al. Thyroid carcinoma, version 2.2014. J Natl Compr Cancer Netw. 2014;12:1671–80 (quiz 80).
Sugenoya A, Shingu K, Kobayashi S, et al. Surgical strategies for differentiated carcinoma of the thyroid isthmus. Head Neck. 1993;15:158–60.
American Thyroid Association Guidelines Taskforce on Thyroid N, Differentiated Thyroid C, Cooper DS, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167–214.
Lamartina L, Grani G, Arvat E, et al. 8th Edition of the AJCC/TNM staging system of thyroid cancer: what to expect (ITCO#2). Endocr Relat Cancer. 2018;25:L7–11.
Dural AC, Sahbaz NA, Akarsu C, et al. Feasibility of thyroid imaging reporting and data system classification in predicting thyroid malignancy. Am Surg. 2019;85:1345–9.
Ito Y, Miyauchi A, Oda H. Low-risk papillary microcarcinoma of the thyroid: a review of active surveillance trials. Eur J Surg Oncol. 2018;44:307–15.
Lodewijk L, Kluijfhout WP, Kist JW, et al. Characteristics of contralateral carcinomas in patients with differentiated thyroid cancer larger than 1 cm. Langenbecks Arch Surg. 2016;401:365–73.
Brito JP, Ito Y, Miyauchi A, Tuttle RM. A Clinical framework to facilitate risk stratification when considering an active surveillance alternative to immediate biopsy and surgery in papillary microcarcinoma. Thyroid. 2016;26:144–9.
Huang H, Xu ZG, Liu SY, Wang XL. Clinical analysis of 27 cases of well-differentiated carcinoma of the thyroid isthmus. Zhonghua Zhong Liu Za Zhi. 2013;35:871–4.
Lim ST, Jeon YW, Suh YJ. Correlation between surgical extent and prognosis in node-negative, early-stage papillary thyroid carcinoma originating in the isthmus. World J Surg. 2016;40:344–9.
Fama F, Cicciu M, Giudice GL, et al. Pattern of nodal involvement in papillary thyroid cancer: a challenge of quantitative analysis. Int J Clin Exp Pathol. 2015;8:11629–34.
Pontieri G, Urselli F, Peschi L, et al. Is the isthmus location an additional risk factor for indeterminate thyroid nodules? Case report and review of the literature. Front Endocrinol (Lausanne). 2018;9:750.
Wang J, Sun H, Gao L, Xie L, Cai X. Evaluation of thyroid isthmusectomy as a potential treatment for papillary thyroid carcinoma limited to the isthmus: a clinical study of 73 patients. Head Neck. 2016;38(Suppl 1):E1510–4.
Xiang D, Xie L, Xu Y, Li Z, Hong Y, Wang P. Papillary thyroid microcarcinomas located at the middle part of the middle third of the thyroid gland correlates with the presence of neck metastasis. Surgery. 2015;157:526–33.
Hahn SY, Han BK, Ko EY, Shin JH, Ko ES. Ultrasound findings of papillary thyroid carcinoma originating in the isthmus: comparison with lobe-originating papillary thyroid carcinoma. AJR Am J Roentgenol. 2014;203:637–42.
Randolph GW, Duh QY, Heller KS, et al. The prognostic significance of nodal metastases from papillary thyroid carcinoma can be stratified based on the size and number of metastatic lymph nodes, as well as the presence of extranodal extension. Thyroid. 2012;22:1144–52.
Funding
The authors received no specific funding for this work.
Author information
Authors and Affiliations
Contributions
Conceptualization and methodology, SL and OJK; formal analysis, OJK; resources, SL, JSB and CKJ; investigation and data curation, SL and OJK; writing original draft preparation, OJK; writing review and editing, SL and JSB; supervision, SL.
Corresponding author
Ethics declarations
Conflict of interest
There are no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kwon, O., Lee, S., Bae, J.S. et al. Thyroid Isthmusectomy with Prophylactic Central Compartment Neck Dissection is a Feasible Approach for Papillary Thyroid Cancer on the Isthmus. Ann Surg Oncol 28, 6603–6612 (2021). https://doi.org/10.1245/s10434-021-09833-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-021-09833-y