
Abstract
Background
Gastric cancer treatment initiation is a complex process. Inefficiencies in care coordination can lead to significant delays, which are often more prominent at safety net hospitals. Multidisciplinary teams (MDTs) have been proposed as an effective solution.
Methods
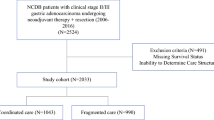
A retrospective review of sequential gastric cancer patients receiving treatment at Parkland Hospital (Dallas, TX) between 2013 and 2015 was performed before (n = 50) and after (n = 50) creation of a MDT and standardized care pathways. Patients undergoing urgent resection were excluded. Time to treatment (TTT) from initial endoscopy to initiation of chemotherapy was evaluated. The number of diagnostic tests performed and treatment variability also were compared.
Results
Groups were similar in terms of age, sex, stage distribution, tumor location, and type of presentation (outpatient vs. emergency room). Post-intervention, TTT decreased from 84.1 ± 12.3 to 32.5 ± 15.2 days (p < 0.02). This decrease was primarily related to parallel performance of subspecialty evaluations, staging studies, and procedures. MDT review reduced the number of unnecessary staging tests performed, leading to a decrease in the average number of studies from 3.8 per patient to 2.2 (p < 0.05). Use of diagnostic laparoscopy in patients with clinically locally advanced disease increased from 18 to 94% (p < 0.05).
Conclusions
Creation of a gastric cancer MDT and uniform care pathways at a large safety net hospital expedited initiation of treatment, reduced unnecessary tests, and promoted consistent patient management.

Similar content being viewed by others

References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69:7–34. https://doi.org/10.3322/caac.21551.
Mokdad A, Ali A, Nassour I, et al. Treatment trends in gastroesophageal and gastric cancers in the United States. J Clin Oncol. 2017;35:136. https://doi.org/10.1200/jco.2017.35.4_suppl.136.
Morgan R, Cassidy M, DeGeus SW, Tseng J, McAneny D, Sachs T. Presentation and survival of gastric cancer patients at an urban academic safety-net hospital. J Gastrointest Surg. 2019;23:239–46. https://doi.org/10.1007/s11605-018-3898-3.
Millas SG, Alawadi ZM, Wray CJ, et al. Treatment delays of colon cancer in a safety-net hospital system. J Surg Res. 2015;198:311–6. https://doi.org/10.1016/j.jss.2015.03.078.
Millas SG, Wray C, Alawadi Z, et al. Treatment of colon cancer in a safety-net hospital system: where are the delays? J Surg Res. 2014;186:505. https://doi.org/10.1016/j.jss.2013.11.216.
Di L, Wu H, Zhu R, et al. Multi-disciplinary team for early gastric cancer diagnosis improves the detection rate of early gastric cancer. BMC Gastroenterol. 2017;17:147. https://doi.org/10.1186/s12876-017-0711-9.
Groene O, Chadwick G, Riley S, et al. Re-organisation of oesophago-gastric cancer services in England and Wales: a follow-up assessment of progress and remaining challenges. BMC Res Notes. 2014;7:24. https://doi.org/10.1186/1756-0500-7-24.
MacDermid E, Hooton G, MacDonald M, McKay G, Grose D, Mohammed N, Porteous C. Improving patient survival with the colorectal cancer multi-disciplinary team. Colorectal Dis. 2009;11:291–5. https://doi.org/10.1111/j.1463-1318.2008.01580.x.
Ajani JA, D’Amico TA, Almhanna K, et al. Gastric cancer, version 3.2016, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Netw. 2016;14:1286–312. https://doi.org/10.6004/jnccn.2016.0137.
Ajani JA, In H, Sano T, et al. AJCC cancer staging manual. New York: Springer; 2016. p. 203–20. https://doi.org/10.1007/978-3-319-40618-3_17.
Bilimoria KY, Ko CY, Tomlinson JS, et al. Wait times for cancer surgery in the United States. Ann Surg. 2011;253:779–85. https://doi.org/10.1097/sla.0b013e318211cc0f.
Murphy CT, Galloway TJ, Handorf EA, et al. Survival impact of increasing time to treatment initiation for patients with head and neck cancer in the United States. J Clin Oncol. 2015;34:169–78. https://doi.org/10.1200/jco.2015.61.5906.
Khorana AA, Tullio K, Elson P, et al. Time to initial cancer treatment in the United States and association with survival over time: an observational study. PLoS ONE. 2019;14:e0213209. https://doi.org/10.1371/journal.pone.0213209.
Sanjeevaiah A, Cheedella N, Hester C, Porembka MR. Gastric cancer: recent molecular classification advances, racial disparity, and management implications. J Oncol Pract. 2018;14:217–24. https://doi.org/10.1200/jop.17.00025.
Zaidi MY, Rappaport JM, Ethun CG, et al. Identifying the barriers to gastric cancer care at safety-net hospitals: a novel comparison of a safety-net hospital to a neighboring quaternary referral academic center in the same healthcare system. J Surg Oncol. 2019;119:64–70. https://doi.org/10.1002/jso.25299.
Lehmann K, Eshmuminov D, Bauerfeind P, et al. 18FDG-PET-CT improves specificity of preoperative lymph-node staging in patients with intestinal but not diffuse-type esophagogastric adenocarcinoma. Eur J Surg Oncol EJSO. 2017;43:196–202. https://doi.org/10.1016/j.ejso.2016.08.020.
Nassour I, Fullington H, Hynan LS, et al. The yield of staging laparoscopy in gastric cancer is affected by racial and ethnic differences in disease presentation. Ann Surg Oncol. 2017;24:1787–94. https://doi.org/10.1245/s10434-017-5805-7.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
None of the authors have conflicts of interest to disclose. SCW is a Disease Oriented Clinical Scholar at UTSW. MRP is a Dedman Family Scholar in Clinical Care at UTSW.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ju, M., Wang, S.C., Syed, S. et al. Multidisciplinary Teams Improve Gastric Cancer Treatment Efficiency at a Large Safety Net Hospital. Ann Surg Oncol 27, 645–650 (2020). https://doi.org/10.1245/s10434-019-08037-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-019-08037-9