
Abstract
Background
The burden of readmissions after major cancer surgery is high. Prior work suggests that one-third of readmitted patients are readmitted to a different hospital than where the surgery was performed. The impact of this location of readmission needs to be more thoroughly understood.
Methods
This retrospective cohort study was performed on Surveillance, Epidemiology, and End Results (SEER)-Medicare patients with bladder, esophagus, lung, or pancreas cancer diagnosed from 2001 to 2007 who underwent extirpative surgery and were readmitted within 90 days. Readmission location was classified as ‘index’ if readmission was at the hospital where surgery was performed, or ‘different’ if readmission was elsewhere. Outcomes including complications, reoperations, in-hospital mortality, 90-day mortality, and 90-day total costs were compared based on the location of readmission using a propensity score inverse probability treatment weight analysis.
Results
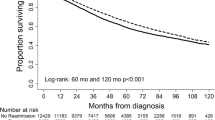
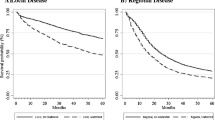
Overall, 7903 (28 %) patients were readmitted within 90 days of index hospitalization. Thirty-three percent were readmitted to a different hospital (bladder 30 %, esophagus 34 %, lung 34 %, pancreas 34 %). Ninety-day mortality and total costs of care were not significantly different between the readmission location groups (all p > 0.05); however, substantial differences in the types of patients, and timing of and reasons for readmission were observed between the two groups.
Conclusions
Patients readmitted to different hospitals after major cancer surgery are a different group of patients than those readmitted to the index hospital. Accounting for this, we did not find significant differences in short-term clinical outcomes or costs of care based on readmission location; however, differences in long-term outcomes were observed that should be further explored in future studies.


Similar content being viewed by others

References
Stitzenberg KB, Chang Y, Smith AB, Nielsen ME. Exploring the burden of inpatient readmissions after major cancer surgery. J Clin Oncol. 2015;33(5):455–464.
Goodney PP, Stukel TA, Lucas FL, Finlayson EV, Birkmeyer JD. Hospital volume, length of stay, and readmission rates in high-risk surgery. Ann Surg. 2003;238(2):161–167.
Gonzalez AA, Shih T, Dimick JB, Ghaferi AA. Using same-hospital readmission rates to estimate all-hospital readmission rates. J Am Coll Surg. 2014;219(4):656–663.
Ryoo JJ, Kunitake H, Frencher SK, et al. Continuity of care: readmission to the same hospital following gastric cancer resection. J Am Coll Surg. 2009;209(3 Suppl):S16–S17.
Brooke BS, Goodney PP, Kraiss LW, Gottlieb DJ, Samore MH, Finlayson SR. Readmission destination and risk of mortality after major surgery: an observational cohort study. Lancet. 2015;386(9996):884–95.
Tsai TC, Orav EJ, Jha AK. Care fragmentation in the postdischarge period: surgical readmissions, distance of travel, and postoperative mortality. JAMA Surg. 2015;150(1):59–64.
Zheng C, Habermann EB, Shara NM, et al. Fragmentation of care after surgical discharge: non-index readmission after major cancer surgery. J Am Coll Surg. 2016;222(5):780–789.e2.
Pak JS, Lascano D, Kabat DH, et al. Patterns of care for readmission after radical cystectomy in New York State and the effect of care fragmentation. Urol Oncol. 2015;33(10):426.e13–29.
Klabunde CN, Potosky AL, Legler JM, Warren JL. Development of a comorbidity index using physician claims data. J Clin Epidemiol. 2000;53(12):1258–1267.
Lawson EH, Louie R, Zingmond DS, et al. A comparison of clinical registry versus administrative claims data for reporting of 30-day surgical complications. Ann Surg. 2012;256(6):973–981.
List of Diagnosis Related Groups (DRGs), FY2008. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/MedicareFeeforSvcPartsAB/downloads/DRGdesc08.pdf.
Lunceford JK, Davidian M. Stratification and weighting via the propensity score in estimation of causal treatment effects: a comparative study. Stat Med. 2004;23(19):2937–2960.
Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399–424.
Xie J, Liu C. Adjusted Kaplan-Meier estimator and log-rank test with inverse probability of treatment weighting for survival data. Stat Med. 2005;24(20):3089–3110.
Sturmer T, Rothman KJ, Avorn J, Glynn RJ. Treatment effects in the presence of unmeasured confounding: dealing with observations in the tails of the propensity score distribution—a simulation study. Am J Epidemiol. 2010;172(7):843–854.
Saunders RS, Fernandes-Taylor S, Kind AJ, et al. Rehospitalization to primary versus different facilities following abdominal aortic aneurysm repair. J Vasc Surg. 2014;59(6):1502–1510, 1510.e1–2.
Luu NP, Hussain T, Chang HY, Pfoh E, Pollack CE. Readmissions after colon cancer surgery: does it matter where patients are readmitted? J Oncol Pract. 2016;12(5):e502–512.
Greenblatt DY, Weber SM, O’Connor ES, LoConte NK, Liou JI, Smith MA. Readmission after colectomy for cancer predicts one-year mortality. Ann Surg. 2010;251(4):659–669.
Donat SM, Shabsigh A, Savage C, et al. Potential impact of postoperative early complications on the timing of adjuvant chemotherapy in patients undergoing radical cystectomy: a high-volume tertiary cancer center experience. Eur Urol. 2009;55(1):177–185.
Funding
Work on this study was supported by the Integrated Cancer Information and Surveillance System (ICISS), University of North Carolina Lineberger Comprehensive Cancer Center, with funding provided by the University Cancer Research Fund (UCRF) via the state of North Carolina. Dr. Nielsen is supported in part by the National Institutes of Health (grant number 1R21CA191610-01), the American Cancer Society (grant MRSG-13-154-01-CPPB), and the Urology Care Foundation/Astellas (Rising Stars in Urology Research Award). The funders did not have any role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Conflicts of interest
Karyn B. Stitzenberg, YunKyung Chang, Angela B. Smith, Michael O. Meyers, and Matthew E. Nielsen have no relevant conflicts of interest to report.
Author information
Authors and Affiliations
Corresponding author
Additional information
I, Karyn Stitzenberg, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Rights and permissions
About this article

Cite this article
Stitzenberg, K.B., Chang, Y., Smith, A.B. et al. Impact of Location of Readmission on Outcomes After Major Cancer Surgery. Ann Surg Oncol 24, 319–329 (2017). https://doi.org/10.1245/s10434-016-5528-1
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5528-1