
Abstract
Background
Papillary thyroid carcinoma (PTC) with clinically node-positive lateral neck is more likely to recur after surgery than node-negative PTC. The present study investigated the risk factors for recurrence in PTC patients with clinically node-positive lateral neck.
Materials and Methods
This study involved 136 patients with pathologically confirmed PTC and a clinically lymph node (LN)-positive lateral neck but no initial distant metastasis who underwent total thyroidectomy with therapeutic central and lateral neck dissection. Clinicopathologic characteristics, intraoperative findings, postoperative thyroglobulin (Tg) levels, and post-treatment recurrences were examined. Univariate and multivariate analyses were performed to identify factors associated with recurrence-free survival (RFS).
Results
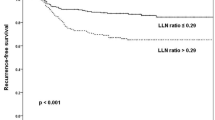
During a median follow-up of 62 months (range 33–90 months), 27 (19.9 %) patients had locoregional or distant recurrences. Univariate analyses showed that primary tumor size (p = 0.049), recurrent laryngeal nerve invasion (p = 0.035), the maximal size of metastatic LN foci (≥1.5 cm; p = 0.012), extranodal extension (p = 0.025), total LN ratio (≥0.26; p = 0.008), American Thyroid Association (ATA) risk categories (p < 0.001), and stimulated serum Tg level (≥4.4; p < 0.001) at the time of radioactive iodine ablation therapy just after thyroidectomy were significant predictors of RFS. Multivariate analyses showed that the maximal size of metastatic foci (p = 0.037), ATA risk categories (p < 0.001), and stimulated Tg level (p < 0.001) were independent predictors of RFS.
Conclusions
Maximal size of metastatic foci, ATA risk categories, and stimulated serum Tg levels are predictive of recurrence after surgery. Careful follow-up of patients with these risk factors is therefore recommended.

Similar content being viewed by others


References
Sivanandan R, Soo KC. Pattern of cervical lymph node metastases from papillary carcinoma of the thyroid. Br J Surg. 2001;88:1241–4.
Shaha AR, Shah JP, Loree TR. Patterns of nodal and distant metastasis based on histologic varieties in differentiated carcinoma of the thyroid. Am J Surg. 1996;172:692–4.
Wada N, Duh QY, Sugino K, Iwasaki H, Kameyama K, Mimura T, et al. Lymph node metastasis from 259 papillary thyroid microcarcinomas: frequency, pattern of occurrence and recurrence, and optimal strategy for neck dissection. Ann Surg. 2003;237:399–407.
Roh JL, Park JY, Park CI. Total thyroidectomy plus neck dissection in differentiated papillary thyroid carcinoma patients: pattern of nodal metastasis, morbidity, recurrence, and postoperative levels of serum parathyroid hormone. Ann Surg. 2007;245:604–10.
Ito Y, Kudo T, Takamura Y, Kobayashi K, Miya A, Miyauchi A. Lymph node recurrence in patients with N1b papillary thyroid carcinoma who underwent unilateral therapeutic modified radical neck dissection. World J Surg. 2012;36:593–7.
Edge SB, Byrd DR, Compton CC. AJCC cancer staging manual. 7th ed. New York: Springer; 2010. p. 87–96.
Lundgren CI, Hall P, Dickman PW, Zedenius J. Clinically significant prognostic factors for differentiated thyroid carcinoma: a population-based, nested case-control study. Cancer. 2006;106:524–31.
Baek SK, Jung KY, Kang SM, Kwon SY, Woo JS, Cho SH, et al. Clinical risk factors associated with cervical lymph node recurrence in papillary thyroid carcinoma. Thyroid. 2010;20:147–52.
Wada N, Masudo K, Nakayama H, Suganuma N, Matsuzu K, Hirakawa S, et al. Recommendation for subclass evaluation of TNM stage iva papillary thyroid carcinomas: T4aN1b patients are at risk for recurrence and survival. Ann Surg Oncol. 2008;15:1511–7.
American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer, Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167–214.
Porterfield JR, Factor DA, Grant CS. Operative technique for modified radical neck dissection in papillary thyroid carcinoma. Arch Surg. 2009;144:567–74.
Koo BS, Choi EC, Yoon YH, Kim DH, Kim EH, Lim YC. Predictive factors for ipsilateral or contralateral central lymph node metastasis in unilateral papillary thyroid carcinoma. Ann Surg. 2009;249:840–4.
Kassouf W, Agarwal PK, Herr HW, Munsell MF, Spiess PE, Brown GA, et al. Lymph node density is superior to TNM nodal status in predicting disease-specific survival after radical cystectomy for bladder cancer: analysis of pooled data from MDACC and MSKCC. J Clin Oncol. 2008;26:121–6.
Ryu IS, Song CI, Choi SH, Roh JL, Nam SY, Kim SY. Lymph node ratio of the central compartment is a significant predictor for locoregional recurrence after prophylactic central neck dissection in patients with thyroid papillary carcinoma. Ann Surg Oncol. 2014;21:277–83.
Schneider DF, Mazeh H, Chen H, Sippel RS. Lymph node ratio predicts recurrence in papillary thyroid cancer. Oncologist. 2013;18:157–62.
Vas Nunes JH, Clark JR, Gao K, Chua E, Campbell P, Niles N, et al. Prognostic implications of lymph node yield and lymph node ratio in papillary thyroid carcinoma. Thyroid. 2013;23:811–6.
Kim TY, Kim WB, Kim ES, Ryu JS, Yeo JS, Kim SC, et al. Serum thyroglobulin levels at the time of 131I remnant ablation just after thyroidectomy are useful for early prediction of clinical recurrence in low-risk patients with differentiated thyroid carcinoma. J Clin Endocrinol Metab. 2005;90:1440–5.
Kim SJ, Park SY, Lee YJ, Lee EK, Kim SK, Kim TH, et al. Risk factors for recurrence after therapeutic lateral neck dissection for primary papillary thyroid cancer. Ann Surg Oncol. 2014;21:1884–90.
Hughes DT, Miller BS, Cohen MS, Doherty GM, Gauger PG. Outcomes of total thyroidectomy with therapeutic central and lateral neck dissection with a single dose of radioiodine in the treatment of regionally advanced papillary thyroid cancer and effects on serum thyroglobulin. Ann Surg Oncol. 2014;21:1647–52.
Ito Y, Miyauchi A. Lateral and mediastinal lymph node dissection in differentiated thyroid carcinoma: indications, benefits, and risks. World J Surg. 2007;31:905–15.
Sugitani I, Kasai N, Fujimoto Y, Yanagisawa A. A novel classification system for patients with PTC: addition of the new variables of large (3 cm or greater) nodal metastases and reclassification during the follow-up period. Surgery. 2004;135:139–48.
Ito Y, Tomoda C, Uruno T, Takamura Y, Miya A, Kobayashi K, et al. Prognostic significance of extrathyroid extension of papillary thyroid carcinoma: massive but not minimal extension affects the relapse-free survival. World J Surg. 2006;30:780–6.
Lipton RJ, McCaffrey TV, van Heerden JA. Surgical treatment of invasion of the upper aerodigestive tract by well-differentiated thyroidcarcinoma. Am J Surg. 1987;154:363–7.
Nishida T, Nakao K, Hamaji M, Kamiike W, Kurozumi K, Matsuda H. Preservation of recurrent laryngeal nerve invaded by differentiated thyroid cancer. Ann Surg.1997;226:85–91.
Randolph GW, Kamani D. The importance of preoperative laryngoscopy in patients undergoing thyroidectomy: voice, vocal cord function, and the preoperative detection of invasive thyroid malignancy. Surgery. 2006;139:357–62.
Van Herle AJ, Uller RP, Matthews NI, Brown J. Radioimmunoassay for measurement of thyroglobulin in human serum. J Clin Invest. 1973;52:1320–7.
Eustatia-Rutten CF, Smit JW, Romijn JA, van der Kleij-Corssmit EP, Pereira AM, Stokkel MP, et al. Diagnostic value of serum thyroglobulin measurements in the follow-up of differentiated thyroid carcinoma, a structured meta-analysis. Clin Endocrinol. 2004;61:61–74.
Conflict of interest
There are no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Lee, C.W., Roh, JL., Gong, G. et al. Risk Factors for Recurrence of Papillary Thyroid Carcinoma with Clinically Node-Positive Lateral Neck. Ann Surg Oncol 22, 117–124 (2015). https://doi.org/10.1245/s10434-014-3900-6
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-014-3900-6