
Abstract
Background
Patients with ductal carcinoma in situ (DCIS) who are treated with mastectomy seldom recur locally or with metastatic disease. When patients with DCIS recur with invasive cancer, they are upstaged and their lives are threatened. We questioned whether histopathologic data could be used to predict these infrequent events.
Methods
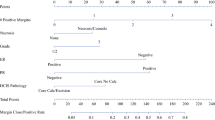
We reviewed a prospective database of 1,472 patients with pure DCIS. All patients were scored from 4 to 12 using the USC Van Nuys Prognostic Index, an algorithm based on DCIS size, nuclear grade, necrosis, margin width, and patient age. Probabilities of recurrence and death were calculated using the Kaplan–Meier method.
Results
A total of 496 patients with pure DCIS were treated with mastectomy. None received any form of postmastectomy adjuvant treatment. Average follow-up was 83 months. Eleven patients developed recurrences, all of whom scored 10–12 using the USC/VNPI. No patient who scored 4–9 recurred. All 11 patients who recurred had multifocal disease and comedo-type necrosis. The probability of disease recurrence after mastectomy for patients scoring 10–12 was 9.6% at 12 years, compared with 0% for those scoring 4–9. There was no difference in overall survival.
Conclusions
There were no recurrences among mastectomy patients who scored 4–9 using the USC/VNPI. Patients scoring 10–12 were significantly more likely to develop recurrence after mastectomy. At risk were young patients with large, high-grade, and multifocal or multicentric tumors. For every 100 patients with USC/VNPI scores of 10–12, 10 patients will recur by 12 years and 2–3 will develop metastatic disease.

Similar content being viewed by others


References
Baxter NN, Virnig BA, Durham SB, Tuttle TM. Trends in the treatment of ductal carcinoma in situ of the breast. J Natl Cancer Inst. 2004;96(6):443–8.
Lee LA, Silverstein MJ, Chung CT, et al. Breast cancer-specific mortality after invasive local recurrence in patients with ductal carcinoma-in situ of the breast. Am J Surg. 2006;192(4):416–9.
Silverstein MJ, Barth A, Poller DN, Gierson ED, Colburn WJ, Waisman JR, Gamagami P. Ten-year results comparing mastectomy to excision and radiation therapy for ductal carcinoma in situ of the breast. Eur J Cancer. 1995;31A:1425–7.
Silverstein MJ. The University of Southern California/Van Nuys prognostic index for ductal carcinoma in situ of the breast. Am J Surg. 2003;186(4):337–43.
Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin. 2009;59(4):225–49. Epub 2009 May 27.
Burstein HJ, Polyak K, Wong JS, Lester SC, Kaelin CM. Ductal carcinoma in situ of the breast. N Engl J Med. 2004;350(14):1430–41.
Katz SJ, Lantz PM, Janz NK, et al. Patient involvement in surgery treatment decisions for breast cancer. J Clin Oncol. 2005;23(24):5526–33.
Ernster VL, Barclay J, Kerlikowske K, Grady D, Henderson C. Incidence of and treatment for ductal carcinoma in situ of the breast. JAMA. 1996;275:913–8.
Kim JH, Tavassoli F, Haffty BG. Chest wall relapse after mastectomy for ductal carcinoma in situ: a report of 10 cases with a review of the literature. Cancer J. 2006;12:92–101.
Godat LN, Horton JK, Shen P, Stewart JH, Wentworth S, Levine EA. Recurrence after mastectomy for ductal carcinoma in situ. Am Surg. 2009;75(7):592–5; discussion 595–7.
Rashtian A, Iganej S, Liu IA, et al. Close or positive margins after mastectomy for DCIS: pattern of relapse and potential indications for radiotherapy. Int J Radiat Oncol Biol Phys. 2008;72:1016–20.
Chan LW, Rabban J, Fowble B, et al. Is radiation indicated in patients with DCIS and close/positive mastectomy margins. Int J Rad Biol Phys. 2008;72:S151.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kelley, L., Silverstein, M. & Guerra, L. Analyzing the Risk of Recurrence after Mastectomy for DCIS: A New Use for the USC/Van Nuys Prognostic Index. Ann Surg Oncol 18, 459–462 (2011). https://doi.org/10.1245/s10434-010-1335-2
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-010-1335-2