
Abstract
HMG-CoA reductase inhibitors (statins), cholesterol-lowering drugs that have not been approved for use in children and adolescents, may cause myopathy as a side effect. We compared the effects of three statins (simva-, prava- and lovastatin) in young rats to determine whether skeletal muscle of young animals is more susceptible than that of adults. We also evaluated whether the type of statin (lipophilic versus hydrophilic) determines the degree of muscle damage. Administration via chow of simvastatin (15 mg/kg of body weight/d) and lovastatin (43-55 mg/kg of body weight/d), both lipophilic, caused stunted growth, high creatine kinase (CK) activity in plasma, and severe myopathy. Statin doses that caused damage were much lower for young rats than for adults. Pravastatin (8-55 mg/kg of body weight/d), a hydrophilic drug, caused none of these symptoms. Histologic analysis of hind paw muscles of simvastatin- and lovastatin-treated rats showed abundant signs of damage(hypercontraction, fiber necrosis) in the extensor digitorum longus, correlating with the symptoms noted above. No cellular infiltrates were seen at the onset, pointing to a noninflammatory myopathy. Pravastatin-treated rats never showed signs of myopathy. Impaired DNA synthesis may explain why muscle toxicity is seen at lower doses in young, rapidly developing rats than in adult animals. The difference in muscle damage between the statins may be attributed to differences in lipophilicity and thus in tissue selectivity. Our results can be important when considering drug therapy in young patients with inherited lipoprotein disorders.
Similar content being viewed by others


Main
A high level of cholesterol in plasma is a major risk factor in the development of cardiovascular disease. Atherosclerosis may start in young people, especially in patients with hereditary disorders such as familial hypercholesterolemia or familial combined hyperlipidemia(1, 2). The role of drug treatment in children with lipoprotein disorders remains controversial. To date, the only lipid-lowering drugs recommended by the National Cholesterol Education Program (NCEP) for use in children are bile acid sequestrants(3–6). The so-called statins, simva-, prava-, and lovastatin, are highly effective cholesterol-lowering drugs which act by inhibiting the enzyme HMG-CoA reductase, the rate-limiting enzyme in cholesterol biosynthesis(7–11). Although they have not been approved for use in the pediatric population, some cases of administration to subjects younger than 19 y of age without adverse clinical effects have been described [lovastatin and simvastatin(3); lovastatin(12, 13); and simvastatin(14, 15)].
Some adult patients treated with statins show side effects related with myopathy, such as rhabdomyolysis, muscle pain, and elevation in CK activity in serum. Several authors mentioned these side effects to occur during simvastatin treatment(16–18). Lovastatin and pravastatin mainly showed adverse effects when coadministered with certain other drugs(11, 19–21), although two cases of pravastatin-associated myopathy in single drug regimens have been reported(22, 23). When medication was stopped, the side effects subsided in time.
The cholesterol synthetic pathway plays an important role in cell growth. Not only the end product, cholesterol, is required for the formation of membranes in replicating cells, also intermediates are essential. For example, mevalonate, produced by HMG-CoA-reductase, is necessary for DNA replication(24, 25). Statins have been shown to affect cell proliferation in vitro [lovastatin(26, 27); simvastatin(24); and pravastatin(28)]. The lipophilic HMG-CoA-reductase inhibitor simvastatin has an inhibitory effect on the proliferation of rat and human myocytes (smooth muscle), in contrast with the more hydrophilic pravastatin. The difference between the statins was attributed to their different tissue selectivity(24).
In view of these growth inhibitory effects of statins, it is plausible that skeletal muscle of young, rapidly developing animals is more susceptible to statin treatment, depending on the tissue selectivity of the type of statin, than that of adults. To test this hypothesis we compared the effect of simvastatin, pravastatin, and lovastatin on the development of myopathy in young rats with histologic and biochemical methods. In view of the growth retardation observed in some statin-treated animals [rabbit(29) and rat(30)], we also tested whether starvation alone caused the side effects seen with statin intake.
The experiments were performed with male rats which are more sensitive to muscle damage than females(31). Serum levels of CK activity were measured because CK is considered a biochemical indicator for muscle damage(32–35). To characterize and quantify the severity of muscle damage and to gain more insight into the pathogenesis of this myopathy we analyzed the soleus (mainly slow twitch type I fibers) and EDL (mainly fast twitch type II fibers) muscles histologically.
METHODS
General . Statins. Simvastatin, lovastatin (gift from Merck Sharp & Dohme Research Laboratories, Rahway, NJ), and pravastatin(gift from Bristol-Myers Squibb Institute for Pharmaceutical Research, Princeton, NJ) were used in this study. They were mixed with powdered ingredients of a standard Hope Farms chow (RMH-TM) in concentrations ranging from 10 to 400 mg/kg of chow and pelleted in a bench-top laboratory press(CPM, model CL3) according to standard procedures (Hope Farms, Woerden, The Netherlands). The groups are named according to drug and the doses they received (simva-100 = 100 simvastatin mg/kg of chow). For reference, the doses are also expressed in mg/kg of bw/d.
Experimental setup. The experiments lasted 3 wk, or less when animals became ill. In all experiments weanling (3-wk-old) male Wistar rats were used (UW:U, GDL Utrecht, The Netherlands). Rats were weighed individually three times a week. Physical signs such as general weakening, cachexia, a dull fur, local alopecia, and reflexes were recorded. Trailing with one or both hind limbs, as a sign of a myopathy, was noted separately. Statin intake was calculated by measuring food intake. CK was determined in serum obtained from a tail artery under light anesthesia (Hypnorm, 0.1 mL/100 g of bw) at d 10 or earlier, if severe myopathy became apparent, and repeated at the end of the experiment. Blood was centrifuged immediately (6 min, 3000 rpm), and plasma was kept at 4°C until further processing. CK activity was measured with a dry-chemistry method (Ektachem 700XQ, Kodak, 37°C). Plasma cholesterol levels were measured enzymatically (Boehringer Mannheim, Germany) at the end of the experiment. After 3 wk, or earlier if a severe myopathy was observed, the rats were anesthetized (Valium/Hypnorm) and killed. The left soleus and EDL muscle were dissected within 10 min, fixed in paraformaldehydelysine-phosphate buffer (0.5% paraformaldehyde, 0.05 M phosphate buffer, and 7.5% sucrose), and embedded in glycolmethacrylate. The study was approved by the Medical Faculty Committee for Studies in Experimental Animals.
Histologic analysis. Longitudinal sections (3 μm thick) of the left soleus and EDL were taken in three different regions: superficial (region 1), 100 μm deeper (region 2), and again 100 μm deeper (region 3, about the mid-part of the muscle). They were mounted on glass slides and stained with toluidine blue to study disturbances of the normal architecture of the muscle fibers with light microscopy: disarray of the normal banding pattern of the A- and I-bands (hypercontraction, widening) or necrosis of whole muscle fiber. Muscle damage was quantified by counting affected muscle fibers or by an interactive image analysis package (TIM, DIFA, Breda, The Netherlands). In each longitudinal section five samples were taken at regular distances from the proximal to the distal side of the muscle. In this way a total of 15 samples per muscle were studied (10-25 muscle fibers per sample), representing a total surface of 0.45 mm2. The fibers were scored“damaged” or “not damaged.”
Statistical analysis. Body weight data were analyzed with an analysis of variance followed by the Bonferroni t test for comparison of more than two samples. A two-sampled t test was used for comparison of two samples. CK data showed a highly skewed distribution and were analyzed with the nonparametric Kruskal-Wallis test followed by the Mann-Whitney test. Cholesterol data were analyzed with an analysis of variance followed by the Bonferroni t test. The Pearson product-moment correlation coefficient (r) was used to define a correlation between samples(36). The criterion for statistical significance was a value of p < 0.05. Data are expressed as mean ± SD or median and range.
Dose finding study. As no data were present on doses for young animals, we started with an experiment to find at which dose adverse side effects, if at all, would arise. Based on the potency of the three statins in humans and rats, lovastatin and pravastatin were tested in higher doses than simvastatin(2, 4). Food pellets were prepared with concentrations of 10, 50, and 100 mg of simvastatin; 50, 100, 200, and 400 mg of pravastatin; and 50, 100, and 200 mg of lovastatin per kg of chow. The rats had free access to chow and water. Ninety weanling rats (bw 35-58 g) were assigned at random to 11 groups (n = 6-15, 1 control, 3 simvastatin, 4 pravastatin, and 3 lovastatin groups). Physical signs were recorded, and CK activity, as well as cholesterol-levels in randomly chosen rats in four groups, were measured at the end of the treatment.
Development of simvastatin myopathy in time. To study the development of physical signs, CK activity and muscle fiber damage in time, 28 rats (40-58 g) were matched for bw, divided into two groups (n = 12 and 16, respectively), and fed control chow or chow containing 100 mg of simvastatin per kg of chow. After 2, 5, 7, and 9 d, three rats of the control group and four rats of the statin-treated group were killed, CK activity was measured, longitudinal sections of the soleus and EDL were prepared, and histologic analysis was done by counting damaged muscle fibers.
To test whether a decreased food intake per se caused the symptoms seen in the simvastatin-treated rats, control chow was administered for 9 days to six other rats in the same amount (in weight) as the simvastatin-treated group had eaten (pair-feeding).
Comparison of 2 doses of each statin. Forty-two rats were used(weight, 40-45 g). The rats were divided into seven groups of six rats and had chow and water ad libitum. The groups were administered control chow or pravastatin, lovastatin, or simvastatin, 100 and 400 mg/kg of chow. Damaged muscle surface was measured with interactive image analysis software.
RESULTS
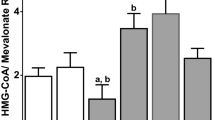
Dose finding study . Physical signs. All statins dose-dependently caused growth retardation, with the order of potency being simvastatin > lovastatin ≅ pravastatin ( Fig. 1, bar graphs). After 9 d, four of the nine rats of the simva-100 group (13 mg of simvastatin/kg of bw) developed adverse physical signs and myopathy. They had a significant lower bw than control rats and looked generally ill (dull fur, less motion, and less grooming). Furthermore, they showed serious muscle weakness in the extremities, a waddling gait, and trailing with one or both hind limbs. There seemed to be no involvement of the nervous system, because squeezing of a hind limb showed a normal onset of the withdrawal reflex, and when the rats were placed on their back they showed a normal righting reflex. Of the other five simva-100 rats, three had an appearance and weight comparable to that of the control rats, and two showed a dull fur but no abnormal walking pattern. The entire simva-100 group was killed at d 9. The other groups showed no myopathy during the 3-wk statin treatment(Table 1). Lovastatin-treated rats showed no symptoms at doses of 200 mg/kg of chow (30 mg/kg of bw/d), but their bw curve deviated significantly from that of the control group. Pravastatin-treated rats, even at doses of 400 mg/kg of chow (55 mg/kg of bw/d), showed no signs and no increase in CK activity, and their bw curve did not deviate significantly from that of controls.

The bw of 3-wk-old rats fed with simvastatin, lovastatin, and pravastatin, as well as control animals (experiment I) are shown in the bar graphs. The animals were weighed daily, but only the weights at d 7, 14, and 21 are given. The × indicates “no data” as the simvastatin-treated animals had been killed (at d 9) because of serious side effects. The doses of statins differ per statin and are given below each bar graph: simvastatin 10, 50, and 100 mg/kg of chow; lovastatin 50, 100, and 200 mg/kg of chow; pravastatin 100, 200, and 400 mg/kg of chow. The line graph(bottom right) shows the growth curve during 9 d of treatment with 100 mg of simvastatin/kg of bw (•) or no statin (○) (experiment II). Bars indicate the SD.
CK activity. Table 1 shows the median CK activity after 9 d or 3 wk of statin treatment. Differences between groups were highly significant (p < 0.001, Kruskal-Wallis). The mean CK activity in the simva-100 group after 9 d was significantly higher than that of the control group. None of the other statin-treated groups showed a significantly higher CK activity. The variation in CK activity within the simva-100 group was large (123-12994 U/L), probably because the group consisted of both sick and almost normal animals. The CK activity was correlated with the occurrence of physical signs or myopathy and with a decrease in bw (r = 0.79), as can be seen from the data for individual animals (Table 1).
Cholesterol level. The mean plasma cholesterol levels (mmol/L)(mean ± SEM) of four rats in the prava-100 (3.4 ± 0.2) and simva-50 (2.6 ± 1.0) groups and nine rats in the simva-100 group (1.0± 0.9) showed no significant differences compared with the control group (2.8 ± 0.4) (Bonferroni), although the rats treated with the highest dose of simvastatin showed a trend toward a decreased level of plasma cholesterol.
Development of simvastatin myopathy in time . Physical signs. Throughout the experimental period rats fed simvastatin showed a lower increase in bw than controls ( Fig. 1, line graph). From d 5 onward the difference was significant. Until d 8 no adverse physical signs were noticeable but at d 9 all four rats of the simvastatin group suffered from severe myopathy as described for experiment I.
CK activity. Until d 7 the CK activity was not different from controls, but at d 9 the CK activity of the simvastatin group reached significantly higher levels (Mann-Whitney test, p < 0.05;Table 2). As in experiment I, there was a strong correlation between bw, CK activity, and physical signs.
Histology. Longitudinal sections of the soleus and EDL of the simvastatin group and control animals showed no morphologic abnormalities at d 7. However, at d 9 all four rats of the simvastatin group showed a markedly disturbed morphology of the EDL (Mann-Whitney test, p < 0.05;Table 2). The soleus muscle was affected in three of the four rats.
Pair-feeding. The bw curve of the rats pair-fed with control chow was similar to that of the simvastatin-treated rats (results not shown). Apart from a lower bw, starving did not produce any of the simvastatin-associated physical signs, nor did it elevate CK levels (CK median 116, range 82-163 U/L).
Comparison of two doses of statins . Statin intake. At the start of the experiment the daily food intake was 6-9 g of chow per rat, resulting in a daily statin dose of 15 and 43-55 mg/kg of bw for the groups treated with 100 and 400 mg of statin/kg of chow, respectively. During the experiment statin intake remained more or less constant, except for the group treated with the highest dose of simvastatin (400 mg/kg of chow). Due to decreased food intake the dose of simvastatin 43 mg/kg of bw dropped to 11 mg/kg of bw followed by death at d 8 or 9.
Physical signs. At d 8, two rats of the simva-400 group had died. Three others were extremely weak, cyanotic, and cold. The last one showed the same signs at d 9. They also had areas with alopecia. However, no muscle weakness was recorded. After collecting a blood sample the rats were killed and muscles were taken out. At d 9 one, and at d 10 four of the lova-400 treated animals showed signs of a severe myopathy (paralysis of the hind limbs). They all showed a dull fur but no other adverse physical signs. Myopathy was also seen in the simva-100 group. Four of the six animals developed myopathy at d 10 without other adverse physical signs. As soon as a severe myopathy was apparent, the rats were anesthetized and killed after collecting blood for CK determination. The other groups showed no adverse physical signs nor myopathy during the 3 wk of statin treatment. In no animal with signs of myopathy involvement of the nervous system could be detected. Squeezing the hind limb showed a normal onset, but less powerful performance, of the withdrawal reflex, and when placed on their back, rats showed a normal righting reflex.
CK activity. All rats with adverse physical signs or myopathy showed raised CK levels, as high as 44 800 U/L. For unaffected animals, the CK activity at d 10 was noted (Table 3). The CK activities of the lova-400, simva-100, and simva-400 groups were significantly higher than those of the other groups. The variation in CK activity within these groups was large as the group consisted of both sick and normal animals. Both pravastatin groups, and the lova-100 group did not show elevated CK levels. In both simvastatin groups and the lova-400 group the CK activity correlated with the occurrence of adverse physical signs or myopathy and with a decrease in bw.
Body weight. Table 3 shows the differences in bw of the seven different groups at d 8-10. All rats showed dose-dependent changes, simvastatin being the most potent. At d 9, the bw of all high statin groups and the simva-100 differed significantly from the control group(t test, p < 0.001 and p < 0.05, respectively).
Histology. In the lova-400 and simva-100 groups large regions of muscle fiber damage were observed consisting of focal areas with hypercontraction and a total loss of internal structure (Fig. 2, A and B). Also, necrosis of muscle fibers became apparent (Fig. 2, C and D). This was particularly outspoken in the EDL, whereas the soleus muscle was spared. A striking feature was the relatively mildly affected EDL in the simva-400 group. The control, prava-100/400, and the lova-100 groups showed only mild damage, or no damage at all. In the soleus muscle we sometimes found “smudges”: tiny areas of focal myofibrillar disruption without hypercontraction (not shown). Electron microscopic study showed that these “smudges” seen at light microscopy were small areas with Z-band streaming. They were observed only in the soleus of animals with muscle damage, and they were the only abnormality we occasionally found in muscles of animals treated with pravastatin (prava-400 only).

Resumé of the most commonly seen muscle damage in toluidine blue-stained longitudinal sections of the EDL muscle of a rat treated with simvastatin 100 mg/kg of chow. (A) Focal damage with hypercontraction (h) and (B) extensive damage with hypercontraction (h). The lesions consist of coagulated myofiber cytoplasm and loss of internal structure. (C and D) Degenerating myofibers (d) largely occupied by macrophages and clotted fibers (c); v is a blood vessel. Thickness: 3μm. Scale bar represents 25 μm.
The results of quantification of damaged muscle surface are summarized inTable 3. For the soleus muscle, damage seen in the lova-400 and simva-400 groups differed significantly from the control group(Mann-Whitney test, p < 0.05) but also from both pravastatin-treated groups (p < 0.05). For the EDL muscle both simvastatin groups and the lova-400 group showed significantly more muscle damage than the control group (p < 0.05). Compared with the highest pravastatin group (400 mg/kg of chow) the difference was highly significant (p < 0.001 for all three groups). Body weight, myopathy, CK activity, and morphometrical data were highly correlated.
DISCUSSION
Treatment of young rats with simvastatin (15 mg/kg of bw/d) in the 1st wk postweaning resulted in general malaise, high CK activity in serum, and a severe myopathy. The latter two findings appeared very abruptly between d 8 and 9. The same dose does not affect adult rats. At d 5, before any signs were noticeable, a significantly lower bw and reduced food intake could be observed. However, reduced food intake per se did not produce symptoms. Histologic studies showed severe disturbance of the normal muscle cytoarchitecture, especially in the EDL. CK activity and bw were correlated with muscle fiber damage in the EDL and physical signs. Lovastatin in the same dose did not produce CK elevations or myopathy, but a higher dose of lovastatin (43 mg/kg of bw/d) did. Pravastatin produced none of these symptoms at any dose tested (15-55 mg/kg of bw/d). Even very high doses, more than 100 mg/kg of bw/d, tested in a pilot experiment, produced very small, but extremely lively, animals, that neither looked ill nor showed signs of myopathy.
It appears from our study that young rats are less susceptible to statin-induced muscle damage from pravastatin than from simvastatin or lovastatin, as also has been described for adult rats. Treatment with statins in very high doses, several times higher than we used (150-1200 mg/kg of bw/d), administered via gavage in methylcellulose resulted in decreased physical activity, localized alopecia, decreased food consumption, and mortality. Simvastatin caused muscle damage at lower doses than pravastatin and lovastatin(30). However, even the lowest dose of simvastatin used for adult rats by these authors was still more than four times higher than the highest dose we used for young animals (180 and 43-55 mg/kg of bw/d, respectively), although the method of statin administration(chow versus gavage) could slightly affect drug availability and serum levels. A pilot experiment indicated that statins are taken up better via gavage (i.e. was toxic at lower doses), which makes the difference between the doses even more pronounced. Another pilot experiment consisting of 3 wk of simvastatin (15 mg/kg of bw/d) treatment of adult rats(age 6 wk, bw 159 g) showed no symptoms and no significant decrease in bw(data not shown).
The cholesterol-reducing properties of statins in rats remain controversial. The observed changes in plasma cholesterol levels vary considerably. Plasma cholesterol levels in rats treated with lovastatin have been shown to increase(37) or decrease(38). In contrast, simvastatin and pravastatin treatment of adult rats did not result in any significant change of cholesterol levels(10, 39). Very little is known about possible differences in pharmacokinetics and pharmacodynamics between young and adult rats. In our study no significant effects of the different statins on cholesterol levels in young rats could be detected.
The potency of simvastatin as a cholesterol-lowering drug in humans is about one to three times higher than that of pravastatin and lovastatin(2, 4). However, young rats receiving a dose of pravastatin four times as high as a dose of simvastatin that led to myopathy, showed no symptoms at all. This difference may be explained by their different selectivity toward nonhepatic cells(10, 40–42). Lovastatin and simvastatin enter the cell easily, whereas the more hydrophilic pravastatin remains in the extracellular space(43, 44). Experiments in which simvastatin and lovastatin inhibited the cholesterol synthesis in the lenses of various animals, but pravastatin did not, support this theory(40, 42, 45). As simvastatin is even more lipophilic than lovastatin, this may explain why simvastatin produced symptoms at lower doses than did lovastatin(43).
Animals treated with simvastatin or lovastatin showed an early deviation of the growth curve and developed high CK activity and myopathy later on. In pravastatin-treated animals such relation did not exist: the bw in rats treated with high doses of pravastatin was lower than in controls, but never associated with clinical signs. Fasting alone without the administration of statin did not cause any symptoms in weanling rats other than stunted growth, indicating that this per se does not lead to a myopathy. Also, whereas growth is affected in an early stage, the myopathy had a very abrupt, relatively late onset, making it less likely that the loss of bw alone causes myopathy. Force-feeding of rabbits treated with simvastatin ameliorated the symptoms, suggesting that a decrease in food consumption potentiates statin toxicity(29). These observations and our results collectively suggest that bw plays an important role in, but does not cause, the appearance of symptoms during statin treatment.
The damage caused by high doses of lipophilic statins does not involve all muscle fibers, and the fibers are not (except when necrosis occurs) affected over their entire length. The most obvious damage occurred in the EDL muscle of animals treated with simva-100 (15 mg/kg of bw/d) or lova-400 (43-55 mg/kg of bw/d). In these groups the EDL was either severely damaged or not affected at all, pointing to some threshold effect. Severe muscle damage was always accompanied by an increase in CK activity and myopathy. In the prava-400 rats(43-55 mg/kg of bw/d) the only muscle damage we observed were small, focal areas of myofibrillar disturbances observed in the soleus muscle, not in the EDL muscle. Similar spots were also seen in the soleus of the other groups. In the pravastatintreated animals these small spots of damage were never associated with an increased CK activity or myopathy. Similar small areas of fiber damage have been described in muscle biopsies from the soleus of man 1 wk postexercise(46). In our study muscle fiber damage was most obviously present in the EDL muscle which contains mainly type II(fast-twitch, glycolytic) fibers, corresponding with the observation of others in adult rats(30). Furthermore, patients receiving lovastatin plus gemfibrozil show a predominant type II atrophy(47). The soleus muscle, with only few type II fibers and mainly type I fibers, showed less damage. The highest dose of simvastatin we used (43-55 mg/kg of bw/d) caused small and seriously ill animals without signs of myopathy. Muscle damage, especially in the EDL, was relatively mild compared with the damage in the simvastatin (15 mg/kg of bw/d) and lovastatin(43-55 mg/kg of bw/d) groups, but the CK activity was the highest observed in this study. It is likely that these animals would have developed serious morphologic muscle damage had they survived the simvastatin treatment. This observation gives further insight into the order of symptoms: first, growth is affected, then CK leaks into the circulation as muscle starts to be affected, then a full-blown myopathy develops, evidenced by clinical and histologic criteria.
The etiology of statin-induced myopathy remains poorly understood. The abrupt occurrence of myopathy in the rats treated with simvastatin or lovastatin is suggestive of a threshold or cumulative effect on the muscle membrane. The membrane defect may allow influx of calcium into muscle fibers causing hypercontraction and initiating fiber necrosis(48–52). This, however, does not shed further light on the basic cause of the plasma membrane defect. One hypothesis is that the cholesterol content of the muscle membrane might be affected(47), another is that statins cause a dramatic increase in membrane fluidity, causing sarcolemmal changes which might underlie the development of myopathy(47, 53). To explain the differences between young and adult animals we hypothesize that statins, apart from their toxicity toward muscle tissue, inhibit the continuous proliferation of myogenic precursor cells, such as satellite cells and myocytes(24), which takes place in growing muscle. HMG-CoA reductase inhibitors interfere with mevalonate metabolism, a precursor of cholesterol(25). Some intracellular proteins which play an essential role in the cell cycle require covalent binding to farnesol, an intermediate in mevalonate metabolism. By binding to the inner plasma membrane, and therefore possibly serving as signaling mechanisms for growth factors, these farnesylated proteins (p21ras, lamin B) allow the cell to enter from the G1 phase into the DNA synthetic phase (S phase)(26, 27, 54). This hypothesis is currently under investigation. Thus, in combination with possible membrane defects, chiefly structures which are highly dependent of DNA synthesis, will be affected by statin treatment, particularly in the juvenile stage. In the young, fast growing organism, muscle is such tissue, whereas in adult animals higher doses of statin may be necessary to affect muscle. These results may be of importance when considering treatment of children with hereditary disorders of lipid metabolism with particular members of this group of cholesterol-lowering drugs. Although sporadically authors have reported well tolerated treatment of children with a HMG-CoA-reductase inhibitor(3, 12, 13, 15), our results suggest that more detailed, specifically designed, long-term studies in a pediatric population will be necessary before this group of HMG-CoA-reductase inhibitors may be safely applied to children and adolescents.
Note: After acceptance of this manuscript we became aware of an independently performed safety study with pravastatin in young children(55). Three doses (5-10-20 mg/kg) were given for 12 wks to children (age 8-16 y) in a double-blind study. These doses were all well tolerated; adverse effects were mild and equally distributed among the three treatment groups. The plasma total-and LDL-cholesterol levels were significantly reduced. Although the authors conclude that a long-term study is necessary before new treatment strategies can be considered, their results in children and our results in young rats strongly suggest that in such studies pravastatin is the most likely candidate for safe and effective treatment of familial hypercholesterolemia.
Abbreviations
- EDL:
-
extensor digitorum longus
- CK:
-
creatine kinase (EC 2.7.3.2)
- HMG:
-
3-hydroxy-3-methylglutaryl
- bw:
-
body weight
References
Brown MS, Goldstein JL 1984 How LDL receptors influence cholesterol and atherosclerosis. Sci Am 251: 52–60.
Illingworth DR, Bacon S 1987 Hypolipidemic effects of HMG-CoA reductase inhibitors in patients with hypercholesterolemia. Am J Cardiol 60: 33G–42G.
Stein EA 1989 Treatment of familial hypercholesterolemia with drugs in children. Arteriosclerosis 9( suppl): I145–I151.
Malini PL, Ambrosioni E, De Divitiis O, Di Somma S, Rosiello G, Trimarco B 1991 Simvastatin versus pravastatin: efficacy and tolerability in patients with primary hypercholesterolemia. Clin Ther 13: 500–510.
Kwiterovich PO Jr 1993 Identification and treatment of heterozygous familial hypercholesterolemia in children and adolescents. Am J Cardiol 72: 30D–37D.
National Cholesterol Education Program 1992 Report of the expert panel on blood cholesterol levels in children and adolescents. Pediatrics 89: 525–584.
Alberts AW 1988 HMG-CoA reductase inhibitors-the development. Atheroscler Rev 18: 123–131.
Hoffman WF, Alberts AW, Anderson PS, Chen JS, Smith RL, Willard AK 1986 3-Hydroxy-3-methylglutaryl-coenzyme A reductase inhibitors. 4. Side chain ester derivatives of mevinolin. J Med Chem 28: 849–852.
Haruyama H, Kuwano H, Kinoshita T, Terahara A, Nishigaki T, Tamura C 1986 Structure elucidation of the bioactive metabolites of ML-236B(mevastatin) isolated from dog urine. Chem Pharm Bull 34: 1459–1467.
Tsujita Y, Kuroda M, Shimada Y, Tansawa K, Arai M, Kaneko I, Tanaka M, Masuda H, Tarumi C, Watanabe Y, Fujii S 1986 CS-514, a competitive inhibitor of 3-hydroxy-3-methylglutaryl coenzyme A reductase: tissue-selective inhibition of sterol synthesis and hypolipidemic effect on various animal species. Biochim Biophys Acta 877: 50–60.
McTavish D, Sorkin EM 1991 Pravastatin. A review of its pharmacological properties and therapeutic potential in hypercholesterolaemia. Drugs 42: 65–89.
Tarantino MD, McNamara DJ, Granstrom P, Ellefson RD, Unger EC, Udall JN 1991 Lovastatin therapy for cholesterol ester storage disease in two sisters. J Pediatr 118: 131–135.
Cortner JA, Coates PM, Liacouras CA, Jarvik GP 1993 Familial combined hyperlipidemia in children: clinical expression, metabolic defects, and management. J Pediatr 123: 177–184.
Leone L, Ippoliti PF 1991 Use of simvastatin plus cholestyramine in the treatment of lysosomal acid lipase deficiency. [Letter] J Pediatr 119: 1008–1009.
Ducobu J, Brasseur D, Chaudron JM, Deslypere JP, Harvengt C, Muls E, Thomson M 1992 Simvastatin use in children. [Letter] Lancet 339: 1488
Deslypere JP, Vermeulen A 1991 Rhabdomyolysis and simvastatin. [Letter] Ann Intern Med 114: 342
Berland Y, Vacher Coponat H, Durand C, Baz M, Laugier R, Musso JL 1991 Rhabdomyolysis with simvastatin use. [Letter] Nephron 57: 365–366.
Bizarro N, Bagolin E, Milani L, Cereser C, Finco B 1992 Massive rhabdomyolysis and simvastatin. Clin Chem 38: 1504
Kogan A, Orenstein S 1990 Lovastatin-induced acute rhabdomyolysis. Postgrad Med J 66: 294–296.
Goldman JA, Fishman AB, Lee JE, Johnson RJ 1989 The role of cholesterol-lowering agents in drug-induced rhabdomyolysis and polymyositis. Arthritis Rheum 32: 358–359.
Wiklund O, Angelin B, Bergman M, Berglund L, Bondjers G, Carlson A, Lindén T, Miettinen T, Odman B, Olofsson SO, Saarinen I, Sipinen R, Sjöström P, Kron B, Vanhanen H, Wright I 1993 Pravastatin and gemfibrozil alone and in combination for the treatment of hypercholesterolemia. Am J Med 94: 13–20.
Wiklund O, Angelin B, Fager G, Eriksson M, Olofsson SO, Berglund L, Lindén T, Sjöberg A, Bondjers G 1990 Treatment of familial hypercholesterolaemia: a controlled trial of the effects of pravastatin or cholestyramine therapy on lipoprotein and apolipoprotein levels. J Int Med 228: 241–247.
Schalke BB, Schmidt B, Toyka K, Hartung HP 1992 Pravastatin-associated inflammatory myopathy. [Letter] N Engl J Med 327: 649–650.
Corsini A, Raiteri M, Soma MR, Gabbiani G, Paoletti R 1992 Simvastatin but not pravastatin has a direct inhibitory effect on rat and human myocyte proliferation. Clin Biochem 25: 399–400.
Goldstein JL, Brown MS 1990 Regulation of the mevalonate pathway. Nature 343: 425–430.
Jakóbisiak M, Bruno S, Skierski JS, Darewicz Z 1991 Cell cycle-specific effects of lovastatin. Proc Natl Acad Sci USA 88: 3628–3632.
O'Donnell MP, Kasiske BL, Kim Y, Atluru D, Keane WF 1993 Lovastatin inhibits proliferation of rat mesangial cells. J Clin Invest 91: 83–87.
Kawata S, Nagase T, Yamasaki E, Ishiguro H, Matsuzawa Y 1994 Modulation of the mevalonate pathway and cell growth by pravastatin andd-limonene in a human hepatoma cell line (Hep G2). Br J Cancer 69: 1015–1020.
Kornbrust DJ, Macdonald JS, Peter CP, Duchai DM, Stubbs RJ, Germershausen JI, Alberts AW 1989 Toxicity of the HMG-coenzyme A reductase inhibitor, lovastatin, to rabbits. J Pharmacol Exp Ther 248: 498–505.
Smith PF, Eydelloth RS, Grossman SJ, Stubbs RJ, Schwartz MS, Germershausen JI, Vyas KP, Kari PH, McDonald JS 1991 HMG-CoA reductase inhibitor-induced myopathy in the rat: cyclosporine A interaction and mechanism studies. J Pharmacol Exp Ther 257: 1225–1235.
Amelink GJ, Bär PR 1986 Exercise-induced muscle damage in the rat: effects of hormonal manipulation. J Neurol Sci 76: 61–68.
Rogers MA, Stull GA, Apple FS 1985 Creatine kinase isoenzyme activities in men and women following a marathon race. Med Sci Sports Exerc 17: 679–682.
Armstrong RB 1986 Muscle damage and endurance events. Sports Med 3: 370–381.
Kagen LJ, Aram S 1987 Creatine kinase activity inhibitor in sera from patients with muscle disease. Arthritis Rheum 30: 213–217.
Bär PR, Rodenburg JW, Koot RW, A`melink GJ 1994 Exercise-induced muscle damage: recent developments. Basic Appl Myol 4: 5–16.
Glantz SA 1987 Primer of Biostatistics. McGraw-Hill, New York
Yamauchi S, Linscheer WG, Beach DH 1991 Increase in serum and bile cholesterol and HMG-CoA reductase by lovastatin in rats. Am J Physiol 23:G625–G630.
Chao Y, Chen JS, Hunt VM, Kuron GW, Karkas JD, Liou R, Alberts AW 1991 Lowering of plasma cholesterol levels in animals by lovastatin and simvastatin. Eur J Clin Pharmacol 40:S11–S14.
Sérougne C, Mathé D, Férézou J, Bertin C, Riottot M, Lutton C, Jacotot B 1995 Effects of simvastatin on plasma lipoprotein concentrations and very-low-density lipoprotein secretion in the rat. J Clin Biochem Nutr 18: 55–64.
Mosley ST, Kalinowski SS, Schafer BL, Tanaka RD 1989 Tissue-selective acute effects of inhibitors of 3-hydroxy-3-methylglutaryl coenzyme A reductase on cholesterol biosynthesis in lens. J Lipid Res 30: 1411–1420.
Koga T, Shimada Y, Kuroda M, Tsujita Y, Hasegawa K, Yamazaki M 1990 Tissue-selective inhibition of cholesterol synthesis in vivo by pravastatin sodium, a 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor. Biochim Biophys Acta 1045: 115–120.
Kalinowski SS, Tanaka RD, Mosley ST 1991 Effects of long-term administration of HMG-CoA reductase inhibitors on cholesterol synthesis in lens. Exp Eye Res 53: 179–186.
Serajuddin ATM, Ranadive SA, Mahoney EM 1991 Relative lipophilicities, solubilities and structure-pharmacological considerations of HMG-CoA reductase inhibitors pravastatin, lovastatin, mevastatin and simvastatin. J Pharm Sci 80: 830–834.
Koga T, Fukuda K, Shimada Y, Fukami M, Tsujita Y 1992 Tissue selectivity of pravastatin sodium, lovastatin and simvastatin. The relationship between inhibition of de novo sterol synthesis and active drug concentrations in the liver, spleen and testis in rat. Eur J Biochem 209: 315–319.
De Vries ACJ, Vermeer MA, Bredman JJ, Bär PR, Cohen LH 1992 Cholesterol content of the rat lens is lowered by administration of simvastatin, but not by pravastatin. Exp Eye Res 56: 393–399.
Fridén J, Sjöström M, Ekblom B 1981 A morphological study of delayed muscle soreness. Experientia 37: 506–507.
London SF, Gross KF, Ringel SP 1991 Cholesterol-lowering agent myopathy (CLAM). Neurology 41: 1159–1160.
Mokri B, Engel AG 1975 Duchenne dystrophy: electron microscopic findings pointing to a basic or early abnormality in the plasma membrane of the muscle fiber. Neurology 25: 1111–1120.
Schmalbruch H 1975 Segmental fibre breakdown and defects of the plasmalemma in diseased human muscles. Acta Neuropathol 33: 129–141.
Soza M, Karpati G, Carpenter S, Prescott S 1986 Calcium-induced damage of skeletal muscle fibers is markedly reduced by calcium channel blockers. Acta Neuropathol 71: 70–75.
Baracos V, Greenberg RE, Goldberg AL 1986 Influence of calcium and other divalent cations on protein turnover in rat skeletal muscle. Am J Physiol 250:E702–E710.
Nakahara K, Yada T, Kuriyama M, Osame M 1994 Cytosolic Ca2+ increase and cell damage in L6 rat myoblasts by HMG-CoA reductase inhibitors. Biochem Biophys Res Commun 202: 1579–1585.
Bregestovski PD, Bolotina VN 1989 Membrane fluidity and kinetics of Ca2+-dependent potassium channels. Biomed Biochim Acta 48: 382S–387S.
Fairbanks KP, Witte LD, Goodman DS 1984 Relationship between mevalonate and mitogenesis in human fibroblasts stimulated with platelet-derived growth factor. J Biol Chem 259: 1546–1551.
Knipscheer HC, Boelen CCA, Kastelein JJP, van Diermen DE, Groenemeijer BE, Van den Ende A, Büller HR, Bakker HD 1996 Short-term efficacy and safety of pravastatin in 72 children with familial hypercholesterolemia. Pediatr Res 39: 867–871.
Acknowledgements
We thank Drs. G. J. Amelink, A. L. Bootsma, F. G. I. Jennekens, and J. J. Wokke for their comments. We are indebted to Dr. R. W. Ogilvie (University of Oklahoma) for his opinion on morphologic aspects of this study. We thank C. Brand, A. v. d. Sar, S. de Bont, C. P. W. M. Veraart, W. A. F. Balemans, and P. J. Bosman for technical assistance. The cooperation of Ir Gemma Smulders (Hope Farms) in preparing the pelleted chow is greatly appreciated.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Reijneveld, J., Koot, R., Bredman, J. et al. Differential Effects of 3-Hydroxy-3-methylglutaryl-Coenzyme A Reductase Inhibitors on the Development of Myopathy in Young Rats. Pediatr Res 39, 1028–1035 (1996). https://doi.org/10.1203/00006450-199606000-00016
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199606000-00016
This article is cited by
-
The non-immunosuppressive management of childhood nephrotic syndrome
Pediatric Nephrology (2016)
