
Abstract
Early diagnosis is very important to improve the survival rate of patients with gastric cancer and to understand the biology of cancer. In order to meet the clinical demands for early diagnosis of gastric cancer, we developed a disposable easy-to-use electrochemical microfluidic chip combined with multiple antibodies against six kinds of biomarkers (carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9), Helicobacter pylori CagA protein (H.P.), P53oncoprotein (P53), pepsinogen I (PG I), and PG-II). The six kinds of biomarkers related to gastric cancer can be detected sensitively and synchronously in a short time. The specially designed three electrodes system enables cross-contamination to be avoided effectively. The linear ranges of detection of the electrochemical microfluidic chip were as follows: 0.37–90 ng mL−1 for CEA, 10.75–172 U mL−1 for CA19-9, 10–160 U L−1 for H.P., 35–560 ng mL−1 for P53, 37.5–600 ng mL−1 for PG I, and 2.5–80 ng mL−1for PG II. This method owns better sensitivity compared with enzyme-linked immunosorbent assay (ELISA) results of 394 specimens of gastric cancer sera. Furthermore, we established a multi-index prediction model based on the six kinds of biomarkers for predicting risk of gastric cancer. In conclusion, the electrochemical microfluidic chip for detecting multiple biomarkers has great potential in applications such as early screening of gastric cancer patients, and therapeutic evaluation, and real-time dynamic monitoring the progress of gastric cancer in near future.
Similar content being viewed by others


Background
Gastric cancer (GC) is the second most common cancer and the third leading cause of cancer-related death in China [1–3]. It remains very difficult to cure effectively, primarily because most patients present with advanced diseases. Up to date, gastric cancer prognosis is very poor with 5-year survivals below 24 %. Multidisciplinary treatment is used to improve treatment efficacy of advanced stage of GC. However, it has been proven that gastric cancer is not particularly sensitive to current chemotherapy agents, which is closely associated with intrinsic or acquired properties of gastric cancer cells. Therefore, discovery of early gastric cancer has become main pathway to improve the therapeutic efficacy.
We have tried to establish an early gastric cancer pre-warning and diagnosis system since 2005 [4]. We hoped to find early gastric cancer cells in vivo by multi-mode targeting imaging and serum biomarker detection techniques. Our previous studies showed that subcutaneous and in situ gastric cancer tissues with 5 mm in diameter could be recognized and treated by using multifunctional nanoprobes such as breast cancer-associated antigen 1(BRCAA1)-conjugated fluorescent magnetic nanoparticles [5], human epidermal growth factor receptor-2 (HER-2) antibody-conjugated Rnase A (ribonuclease A)-associated CdTe quantum dots [6], folic acid-conjugated upper conversion nanoparticles [7], Arg-Gly-Asp (RGD) peptide-conjugated gold nanorods [8], ce6-conjugated carbon dots [9], ce6-conjugated Au nanoclusters (AuNCs) [10], HAI-178 antibody-conjugated fluorescent magnetic nanoparticles [11], CD44 monoclonal antibody-conjugated gold nanostars [12], and RNA nanoparticles carrying both ligand and siRNA [13]. However, clinical translation of these prepared nanoprobes still exist great challenge because their biosafety still needs a long term evaluation. We also screened out some breath biomarkers associated with gastric cancer [14], and established some methods and devices to detect these biomarkers [15–17]. We also developed a giant magneto resistive (GMR) microfluidic system to detect the circulation gastric cancer cells [18]. However, up to date, serum biomarker detection to screen or find early gastric cancer is still most effective method.
In the past decades, detection of serum tumor biomarkers has always been an important mean of diagnosis of various cancers. However, accepted unique serological biomarker for gastric cancer, like as Alpha-fetoprotein (AFP) for hepatocellular carcinoma (HCC) [19], remains absent. For this reason, combined detection of multiple serological biomarkers is an alternative effective method for predicting risk of gastric cancer. Several serological biomarkers based on a lot of literature can be used for early diagnosis of gastric cancer so far. Mutations in the tumor suppressor gene p53 are the most commonly observed in human cancers. In the serum of healthy subjects, the presence of P53 protein is extremely rare. Mutations in this gene cause an accumulation of nonfunctional proteins. The accumulated proteins are detectable in tissues, sloughed cells, blood, and other body fluids [20]. The p53 gene mutations are significantly correlated with P53 protein over-expression and contribute to genetic predisposition in gastric cancer patients [21–23]. Carcinoembryonic antigen (CEA) is an acknowledged member of immunoglobulin superfamily, with a role as an intracellular adhesion molecule [24]. A high-serum CEA is associated with a number of malignancies, including colorectal, breast, gastric, and pancreatic cancers [25]. CA19-9 has a positive correlation with depth of invasion, nodal involvement, and peritoneal metastasis in gastric adenocarcinoma [26, 27]. In addition, many studies have shown that serum pepsinogen I (PG I) [28, 29], pepsinogen II (PG II) [30], PG I/PG II ratio [31, 32], and Helicobacter pylori (H. P.) [33–35] are also associated with an increased risk of gastric cancer. So, combined detection of above serum biomarkers is helpful to enhance accuracy of predicting gastric cancer risk.
Enzyme-linked immunosorbent assay (ELISA) is widely used for clinical cancer diagnosis; nevertheless, these ordinary ELISA kits for single biomarker are not suitable for individual diagnosis, especially for patients with risk of gastric cancer. Moreover, the ELISA kits for batch samples from the different patients not only easily expose to cross-contamination, but also the operation is complicated. Self-assembled monolayers (SAMs) are widely used to immobilize biomolecules on gold surfaces [36]. The self-assembly process is the spontaneous organization of substances into gold surfaces. SAMs of different substances have frequently utilized for development of biosensors, microarrays, biochips, and molecular switches [37]. Microfluidic technology seeks to improve analysis time, decreasing the consumption of sample and reagents, diminishing the risk of contamination, consuming less power, and sensitivity through automation, integrating multiplexing analysis, and especially portability to provide the possibility of point-of-care applications [38–40]. In comparison with the methods based on chemiluminescence, fluorescence, electrochemiluminescence, or quartz crystal microbalance, electrochemical immunoassay has attracted tremendous interest due to its high sensitivity, low cost, simple instrumentation, and good portability [41]. All the same, this electrochemical immunoassay still have complicated preparation processes, high cost bring about difficult to clinical application and poor universality.
In this study, in order to meet the clinical demands and to overcome the above disadvantages, we develop a disposable easy-to-use electrochemical microfluidic chip combined with multiple antibodies for early diagnosis of gastric cancer. Optimized design of three electrodes system can effectively avoid cross disturbance. And combined detection based on multiple antibodies can improve the early diagnostic rate of gastric cancer. Accordingly, the unique electrochemical microfluidic chip owns great potential in application for gastric cancer early screening in near future.
Methods
Fabrication of Electrochemical Microfluidic Chip
Microelectrodes were fabricated on a glass wafer using standard micro-fabrication techniques. Chromium (Cr 100 nm)/gold (Au 200 nm) film stack was deposited on the glass wafers using electron-beam evaporator (L-H Inc.). Cr layer acts as the adhesion promoter for the gold film. The Au microelectrodes were formed on a glass wafer using a lift-off process as follows: a photoresist (AZ4903) was spin coated onto a glass wafer and then patterned by photolithography. Next, Au/Cr (200 nm/100 nm) was deposited onto the patterned glass wafer by electron-beam evaporator. After that, the electrodes on the glass substrate were completed by removing the photoresist from underneath the deposited metal using a solvent. Lift off was performed via sonication in acetone followed by rinsing in deionized water. Individual chips were cut using cutting machine (K&S Inc.). Each of the chips included six groups of electrodes. One group of detection electrode was comprised of working electrode, pseudo reference, and counter electrode. The surfaces of the Au electrodes were immobilized with antibodies by chemical process according to the following section of methods. PDMS (polydimethylsiloxane) molds were fabricated by photolithography of SU-8 photoresist on Si wafers and the thickness of SU-8 is 30 μm. PDMS pre-polymer and curing agents were mixed, degassed and poured onto the molds, and cured at 60 °C for 3 h. Individual PDMS chips were cut and inlet/outlet holes were punched. Briefly, PDMS surfaces were exposed to oxygen plasma (DQJ-150, Shanghai, China). PDMS channels were assembled together with glass chips Fig. 1.
Antibodies Immobilization
Firstly, the electrodes were washed ultrasonically in ethanol for 5 min and then were immersed in piranha solution (H2O2(v)/H2SO4(v) = 1/3) for 5 min to clean the surfaces. Subsequently, the electrodes were rinsed with sterile ultrapure water for 10 times and were dried with nitrogen. After dripping 2 μL mercaptoacetic acid (Sigma, USA) on the surface of each working electrode, the chip was placed in an airtight container for 1 h to form a carboxylic self-assembled monolayer. Then, the chip was rinsed with ethanol and was dried with nitrogen gently. The carboxyl groups on the surface of electrodes were activated with 0.4 M 1-ethyl-3-[3-dimethylaminopropyl] carbodiimide hydrochloride (EDC) and 0.2 M N-hydroxysuccinimide (NHS) solution prepared in a 0.1 M phosphate buffer solution (PBS, pH = 7.4) for 20 min for immobilizing antibodies. After rinsing with PBS buffer and drying with nitrogen, six kinds of antibodies (anti-CEA, anti-CA19-9, anti-H.P., anti-P53, anti-PG I, and anti-PG II) solutions were respectively dripped on the surfaces of six working electrodes and incubated at 37 °C for 3 h. Lastly, the immunological chip was obtained after incubating 0.5 % BSA (bovine serum albumin) at 37 °C for 1 h to block non-specific binding sites and rinsing with 0.01 M PBS buffer. The prepared chips were stored at 4 °C for next immunoreaction and electrochemical detection.
Immunological Reaction and Electrochemical Signal Detection
The immunological reaction was carried out as follows: Firstly, the six kinds of biomarkers related to gastric cancer (CEA, CA19-9, H.P., P53, PG I, and PG II) solutions were respectively prepared in a series of concentration with phosphate buffer solution (PBS, pH = 7.4) (Table. 1). Secondly, the biomarker solutions with series of concentrations were injected into the microfluidic chips and incubated at 37 °C for 30 min to form the antigen–antibody immune complexes [42–44]. In order to remove unbound biomarkers, PBS was subsequently injected into microfluidic chip for rinsing microchannel and microchamber at 100 μL min−1 for 5 min.
After immunological reaction, antigen–antibody complexes formed on the surface of working electrodes were simultaneously detected by differential pulse voltammetry (DPV) with an electrochemical analyzer (CHI-1030, Chenhua, China). All electrochemical measurements were performed in 5 mM K3[Fe(CN)6]/K4[Fe(CN)6]-PBS (pH = 7.4) solution from −0.3 to 0.6 V at scan rate 50 mV s−1.
Comparing with ELISA and Establishing Multi-index Prediction Model
Three hundred ninety-four specimens of gastric cancer sera were collected from Tangdu Hospital, East-southern Hospital affiliated to East-southern University, Xi’an Central Hospital. Gastric cancer patients were identified by pathological doctor. ELISA kits (Boster, Wuhan, China) for CEA, CA19-9, H.P., PG I, PG II, and P53 were purchased from Shanghai Reagent Company, all ELISA kits obtained the permission certification by China Food and Drug Administration (CFDA). All specimens were examined by using ELISA method and electrochemical method in Department of Clinical Biochemistry, No. 1 People Hospital affiliated to Shanghai Jiao Tong University.
Statistical Analysis
All results are reported as means ± SD. And all data were analyzed by statistical methods including correlation and F test with SPSS 22.0 (IBM Corp., USA). The level of P < 0.05 was regarded as significant.
Results and Discussion
Electrochemical Microfluidic Chip
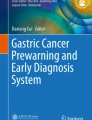
As shown in Fig. 2b, electrochemical microfluidic chips (ECMC) were fabricated successfully. It consists of six detection areas for six different kinds of biomarkers. Every detection area was an independent gold three-electrode unit including working electrode, pseudo reference, and counter microelectrodes. As shown in Fig. 2c, the surface of electrode formed a nano-film consist of Au nanoparticles. The size of a nanoparticle is 50 ± 2 nm. The volume of single chamber is about 0.2–0.25 μL. Six kinds of antibodies against CEA, CA19-9, H.P., PG I, PG II, and P53 were respectively immobilized on surfaces of working electrodes by chemical coupling (Fig. 2a).

Overview of the electrochemical microfluidic chip fabrication process

a Schematic illustration of the electrochemical microfluidic chip. b Picture of electrochemical microfluidic chip. c SEM image of surface of work electrode
Experimental Results of Six Kinds of Biomarkers
The electrodes of chips were characterized by differential pulse voltammetry (DPV). As shown in Fig. 3, the electrons transfer ability of working electrodes weakened obviously compared with bare electrodes (black line) after antibodies immobilization (blue line). After BSA blocking at 37 °C for 1 h (red line), the electrons transfer ability further weakened, but a little. In this study, the DPA signals of electrodes modified with antibodies after BSA blocking were defined as control signals. The control signals of working electrodes for detecting six kinds of biomarkers were −347 nA for CEA, −103 nA for CA19-9, −447 nA for H.P., −298 nA for P53, −373 nA for PG I, and −548 nA for PG II, respectively. All detectable signals stronger than the corresponding control signals were defined as positive signals.

Typical differential pulse voltammograms of the electrode modified by antibodies: a CEA, b CA19-9, c H.P., d P53, e PG I, and f PG II
The six kinds of biomarkers solutions were respectively injected into the microchannels and incubated at 37 °C for 30 min. DPV responses of K3[Fe(CN)6]/K4[Fe(CN)6] PBS were measured by multiplex electrochemical work station. As shown in Fig. 4, the oxidation currents of Fe2+ decreased with the biomarkers concentrations increased, and there was a positive correlation between the oxidation peak currents and the concentration of analytes. As shown in Table 2, the linear detection ranges were 0.37–90 ng mL−1 for CEA, 10.75–172 U mL−1 for CA19-9, 10–160 U L−1 for H.P., 35–560 ng mL−1 for P53, 37.5–600 ng mL−1 for PG I, and 2.5–80 ng mL−1 for PG II, respectively. And the corresponding correlation coefficients were 0.961, 0.983, 0.942, 0.971, 0.934, and 0.972, respectively. The detection limits, the minimum detectable signal higher than control signals, are 0.37 ng mL−1 for CEA, 10.75 U mL−1 for CA19-9, 5 U L−1 for H.P., 35 pg mL−1 for P53, 37.5 ng mL−1 for PG I, and 2.5 ng mL−1 for PG II, respectively. Although the detection point (5 U L−1 for H.P.) was not in the linear range, it still can generate a detectable response signal (Fig. 4c).

Linear detection ranges of six kinds of biomarkers by differential pulse voltammetry. a CEA, b CA19-9, c H.P., d P53, e PG I, and f PG II
As shown in the Fig. 4, electrochemical signals of electrodes weakened owing to formation of antibody–antigen immune complexes. The immune complexed impeded of electrons transporting between the surface of electrodes and K3[Fe(CN)6]/K4[Fe(CN)6]-PBS solution. In addition, external disturbance can efficiently be avoided by independent three microelectrodes system and closed micro-chambers that are conducive to the stable electrochemical signal acquisition.
The currently electrochemical immunoassay is focused on biomarkers immobilized on nanomaterials for enhancing intensity and specificity of signal [45]. The traditional electrochemical immunoassay relied on electroactive materials and enzyme, such as HRP (horseradish peroxidase), thionine, prussian blue, and so on [46, 47]. These reported methods have inevitable limitations such as specific materials and are difficult to acquire stable signals in clinical application. At present, most of multiplex detection always detect two or three biomarkers [46, 48, 49], which cannot meet the clinical needs. This work has adopted a novel solution to avoid the above trouble. We immobilized six kinds of antibodies on the surface of microelectrodes separated by micro-chambers, respectively. An electrochemical microfluidic chip has six detection areas, each of detection area included a working electrode, a pseudo reference, a counter electrode, and a micro-chamber. Independent three electrodes system in micro-chambers avoided the crosstalk between the working electrodes. And this chip can directly detect biomarkers captured by antibodies on the surface of microelectrodes and generate response signals for early diagnosis of gastric cancer.
Comparison with ELISA and Establishment of Multi-index Prediction Model
In order to evaluate the performance of ECMC in clinical application, 394 serum specimens of gastric cancer patients collected were used to measure the serum CEA, CA19-9, H.P., P53, PG I, and PG II levels. The normal cut-off values of CEA, CA19-9, P53, H.P., PG I, PG II, and PG I/PG II are 5.0 ng mL−1, 37 U mL−1, 10 U L−1, 150 pg mL−1, 70 ng mL−1, 11.5 ng mL−1, and 3.0, respectively [30, 31, 50–52]. As shown in Table 3, for electrochemical microfluidic chip (ECMC), the positive rates of CEA, CA19-9, H.P., P53, PG I, PG II were 7.11, 38.07, 68.78, 59.65, 74.11, and 76.74 %, respectively. For ELISA, the positive rates of CEA, CA19-9, H.P., P53, PG I, PG II were 4.57, 33.76, 52.03, 51.52, 66.75, and 65.74 %, respectively. It was evident that ECMC possessed higher detection sensitivity than ELISA.
To explore the correlation between the six kinds of biomarkers and gastric cancer, we established a multi-index prediction model by multiple linear regression based on 394 serum samples of gastric cancer patients. The multi-index model based on large samples can be used to predict risk of gastric cancer more accurately and effectively in clinical screening.
A i (i = 1, 2, 3, 4, 5, 6), X j (j = 1, 2, 3, 4, 5, 6) represented regression coefficient and detection value of six kinds of biomarkers, respectively (Table 4).
Conclusions
In summary, a novel electrochemical immune detection system based on microfluidic chip was developed for simultaneous detecting multiple biomarkers (CEA, CA19-9, H.P., P53, PG I, and PG II) for early diagnosis of gastric cancer. The experimental construction and the DPV detection were based on the fact that the formed antibody–antigen immune complexes retarded the electron transfer tunnel of gold electrodes. Highlights of this work could be summarized as follows: (1) Simultaneous detection for multiple biomarkers has higher efficiency than single biomarker of ELISA. (2) The proposed microfluidic chip with independent reaction micro-chambers can contribute to stable detection signal and minimal false positive compared with conventional protein microchip systems. (3) Microfluidic chip has low detection cost because of low reagent consumption. (4) The ECMC has higher detection sensitivity and is very suitable for clinical diagnosis. (5) The multi-index prediction model can be used to predict risk of gastric cancer more accurately and effectively.
Abbreviations
- BSA:
-
bovine serum albumin
- CA19-9:
-
carbohydrate antigen 19-9
- CEA:
-
carcinoembryonic antigen
- DPV:
-
differential pulse voltammetry
- ECMC:
-
electrochemical microfluidic chips
- EDC:
-
1-ethyl-3-[3-dimethylaminopropyl] carbodiimide hydrochloride
- ELISA:
-
enzyme-linked immunosorbent assay
- GC:
-
gastric cancer
- H.P:
-
Helicobacter pylori CagA protein
- NHS:
-
N-hydroxysuccinimide
- P53:
-
P53 oncoprotein
- PBS:
-
phosphate buffer solution
- PDMS:
-
polydimethylsiloxane
- PG I:
-
pepsinogen I
- PG II:
-
pepsinogen II
- SAMs:
-
self-assembled monolayers
References
WHO Cancer. http://www.who.int/mediacentre/factsheets/fs297/en/. Accessed February 2015.
Lordick F, Allum W, Carneiro F, Mitry E, Tabernero J, Tan P et al (2014) Unmet needs and challenges in gastric cancer: the way forward. Cancer Treat Rev 40(6):692–700
Ferlay J, Shin H-R, Bray F, Forman D, Mathers C, Parkin DM (2010) Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 127(12):2893–2917
Cui DX, Zhang L, Yan XJ, Zhang LX, Xu JR, Guo Y et al (2005) A microarray-based gastric carcinoma prewarning system. World J Gastroentero 11(9):1273–1282
Wang K, Ruan J, Qian QR, Song H, Bao CC, Zhang XQ et al (2011) BRCAA1 monoclonal antibody conjugated fluorescent magnetic nanoparticles for in vivo targeted magnetofluorescent imaging of gastric cancer. J Nanobiotecg 9:23
Ruan J, Song H, Qian QR, Li C, Wang K, Bao CC et al (2012) HER2 monoclonal antibody conjugated RNase-A-associated CdTe quantum dots for targeted imaging and therapy of gastric cancer. Biomaterials 33(29):7093–7102
Ma JB, Huang P, He M, Pan LY, Zhou ZJ, Peng LL et al (2012) Folic acid-conjugated LaF3:Yb, Tm@SiO2 nanoprobes for targeting dual-modality imaging of upconversion luminescence and X-ray computed tomography. J Phys Chem B 116(48):14062–14070
Xu WC, Luo T, Li P, Zhou CQ, Cui DX, Pang B et al (2012) RGD-conjugated gold nanorods induce radiosensitization in melanoma cancer cells by downregulating alpha(v)beta(3) expression. Int J Nanomed 7:915–924
Huang P, Lin J, Wang XS, Wang Z, Zhang CL, He M et al (2012) Light-triggered theranostics based on photosensitizer-conjugated carbon dots for simultaneous enhanced-fluorescence imaging and photodynamic therapy. Adv Mater 24(37):5104–5110
Huang P, Lin J, Wang SJ, Zhou ZJ, Li ZM, Wang Z et al (2013) Photosensitizer-conjugated silica-coated gold nanoclusters for fluorescence imaging-guided photodynamic therapy. Biomaterials 34(19):4643–4654
Wang C, Bao C, Liang S, Zhang L, Fu H, Wang Y et al (2014) HAI-178 antibody-conjugated fluorescent magnetic nanoparticles for targeted imaging and simultaneous therapy of gastric cancer. Nanoscale Res Lett 9(1):1–9
Liang S, Li C, Zhang C, Chen Y, Xu L, Bao C et al (2015) CD44v6 monoclonal antibody-conjugated gold nanostars for targeted photoacoustic imaging and plasmonic photothermal therapy of gastric cancer stem-like cells. Theranostics 5(9):970
Qi LF, Wu LX, Zheng S, Wang YL, Fu HL, Cui DX (2012) Cell-penetrating magnetic nanoparticles for highly efficient delivery and intracellular imaging of siRNA. Biomacromolecules 13(9):2723–2730
Zhang Y, Gao G, Liu H, Fu H, Fan J, Wang K et al (2014) Identification of volatile biomarkers of gastric cancer cells and ultrasensitive electrochemical detection based on sensing interface of Au-Ag alloy coated MWCNTs. Theranostics 4(2):154–162
Gui C, Wang K, Li C, Dai X, Cui DX (2014) A CCD-based reader combined with CdS quantum dot-labeled lateral flow strips for ultrasensitive quantitative detection of CagA. Nanoscale Res Lett 9:57
Mou X, Li T, Wang J, Ali Z, Zhang Y, Chen Z et al (2015) Genetic variation of BCL2 (rs2279115), NEIL2 (rs804270), LTA (rs909253), PSCA (rs2294008) and PLCE1 (rs3765524, rs10509670) genes and their correlation to gastric cancer risk based on universal tagged arrays and Fe3O4 magnetic nanoparticles. J Biomed Nanotechnol 11(11):2057–2066
Zhang J, Song Y, Zhang C, Zhi X, Fu H, Ma Y et al (2015) Circulating MiR-16-5p and MiR-19b-3p as two novel potential biomarkers to indicate progression of gastric cancer. Theranostics 5(7):733–745
Chen L, Bao CC, Yang H, Li D, Lei C, Wang T et al (2011) A prototype of giant magnetoimpedance-based biosensing system for targeted detection of gastric cancer cells. Biosens Bioelectron 26(7):3246–3253
Shu J, Li CG, Liu YC, Yan XC, Xu X, Huang XE et al (2012) Comparison of serum tumor associated material (TAM) with conventional biomarkers in cancer patients. Asian Pac J Cancer P 13(5):2399–2403
Zhang J, Xu ZW, Yu LX, Chen ML, Li K (2014) Assessment of the potential diagnostic value of serum p53 antibody for cancer: a meta-analysis. PLoS One 9(6), e99255
Uchino S, Noguchi M, Ochiai A, Saito T, Kobayashi M, Hirohashi S (1993) p53 mutation in gastric cancer: a genetic model for carcinogenesis is common to gastric and colorectal cancer. Int J Cancer 54(5):759–764
Karim S (2009) Correlation of p53 over-expression and alteration in p53 gene detected by polymerase chain reaction-single strand conformation polymorphism in adenocarcinoma of gastric cancer patients from India. World J Gastroentero 15(11):1381–1387
Otani K, Li XX, Arakawa T, Chan FKL, Yu J (2013) Epigenetic-mediated tumor suppressor genes as diagnostic or prognostic biomarkers in gastric cancer. Expert Rev Mol Diagn 13(5):445–455
Sisik A, Kaya M, Bas G, Basak F, Alimoglu O (2013) CEA and CA 19-9 are still valuable markers for the prognosis of colorectal and gastric cancer patients. Asian Pac J Cancer P 14(7):4289–4294
Shimada H, Noie T, Ohashi M, Oba K, Takahashi Y (2014) Clinical significance of serum tumor markers for gastric cancer: a systematic review of literature by the Task Force of the Japanese Gastric Cancer Association. Gastric Cancer 17(1):26–33
Kwon OK, Yu W, Chung H (2013) Prognostic value of postoperative CA19-9 normalization in patients with advanced gastric cancer. Hepatogastroenterology 60(122):240–243
Fan BA, Xiong B (2011) Investigation of serum tumor markers in the diagnosis of gastric cancer. Hepatogastroenterology 58(105):239–245
Yoshihara M, Sumii K, Haruma K, Kiyohira K, Hattori N, Kitadai Y et al (1998) Correlation of ratio of serum pepsinogen I and II with prevalence of gastric cancer and adenoma in Japanese subjects. Am J Gastroenterol 93(7):1090–1096
Boltin D, Gingold-Belfer R, Dickman R, Halpern M, Morgenstern S, Roth M et al (2014) Gastric mucin expression in first-degree relatives of gastric cancer patients. Eur J Gastroenterol Hepatol 26(7):710–714
Cao XY, Jia ZF, Jin MS, Cao DH, Kong F, Suo J et al (2012) Serum pepsinogen II is a better diagnostic marker in gastric cancer. World J Gastroenterol 18(48):7357–7361
Kitahara F, Kobayashi K, Sato T, Kojima Y, Araki T, Fujino MA (1999) Accuracy of screening for gastric cancer using serum pepsinogen concentrations. Gut 44(5):693–697
Zhang XM, Li JX, Zhang GY, Li XH, Gu H (2014) The value of serum pepsinogen levels for the diagnosis of gastric diseases in Chinese Han people in midsouth China. BMC Gastroenterol 14:3
Malfertheiner P, Selgrad M, Bornschein J (2012) Helicobacter pylori: clinical management. Curr Opin Gastroen 28(6):608–614
Shafaghi A, Mansour-Ghanaei F, Joukar F, Sharafkhah M, Mesbah A, Askari K et al (2013) Serum gastrin and the pepsinogen I/II ratio as markers for diagnosis of premalignant gastric lesions. Asian Pac J Cancer P 14(6):3931–3936
Companioni O, Bonet C, Munoz X, Weiderpass E, Panico S, Tumino R et al (2014) Polymorphisms of Helicobacter pylori signaling pathway genes and gastric cancer risk in the European Prospective Investigation into Cancer-Eurgast cohort. Int J Cancer 134(1):92–101
Ko S, Kim B, Jo SS, Oh SY, Park JK (2007) Electrochemical detection of cardiac troponin I using a microchip with the surface-functionalized poly(dimethylsiloxane) channel. Biosens Bioelectron 23(1):51–59
Canbaz MC, Simsek CS, Sezginturk MK (2014) Electrochemical biosensor based on self-assembled monolayers modified with gold nanoparticles for detection of HER-3. Anal Chim Acta 814:31–38
Hervás M, López MA, Escarpa A (2012) Electrochemical immunosensing on board microfluidic chip platforms. TrAC, Trends Anal Chem 31:109–128
Zhi X, Liu QS, Zhang X, Zhang YX, Feng J, Cui DX (2012) Quick genotyping detection of HBV by giant magnetoresistive biochip combined with PCR and line probe assay. Lab Chip 12(4):741–745
Zhi X, Deng M, Yang H, Gao G, Wang K, Fu H et al (2014) A novel HBV genotypes detecting system combined with microfluidic chip, loop-mediated isothermal amplification and GMR sensors. Biosens Bioelectron 54:372–377
Nahavandi S, Baratchi S, Soffe R, Tang SY, Nahavandi S, Mitchell A et al (2014) Microfluidic platforms for biomarker analysis. Lab Chip 14(9):1496–1514
Morris MC, Depollier J, Mery J, Heitz F, Divita G (2001) A peptide carrier for the delivery of biologically active proteins into mammalian cells. Nat Biotechnol 19(12):1173–1176
Xu H, Aguilar ZP, Yang L, Kuang M, Duan H, Xiong Y et al (2011) Antibody conjugated magnetic iron oxide nanoparticles for cancer cell separation in fresh whole blood. Biomaterials 32(36):9758–9765
Wu M, Mao C, Chen Q, Cu XW, Zhang WS (2010) Serum p53 protein and anti-p53 antibodies are associated with increased cancer risk: a case-control study of 569 patients and 879 healthy controls. Mol Biol Rep 37(1):339–343
Bange A, Halsall HB, Heineman WR (2005) Microfluidic immunosensor systems. Biosens Bioelectron 20(12):2488–2503
Jia X, Liu Z, Liu N, Ma Z (2014) A label-free immunosensor based on graphene nanocomposites for simultaneous multiplexed electrochemical determination of tumor markers. Biosens Bioelectron 53:160–166
Jiang W, Yuan R, Chai Y, Mao L, Su H (2011) A novel electrochemical immunoassay based on diazotization-coupled functionalized bioconjugates as trace labels for ultrasensitive detection of carcinoembryonic antigen. Biosens Bioelectron 26(5):2786–2790
Chen X, Jia X, Han J, Ma J, Ma Z (2013) Electrochemical immunosensor for simultaneous detection of multiplex cancer biomarkers based on graphene nanocomposites. Biosens Bioelectron 50:356–361
Tang D, Hou L, Niessner R, Xu M, Gao Z, Knopp D (2013) Multiplexed electrochemical immunoassay of biomarkers using metal sulfide quantum dot nanolabels and trifunctionalized magnetic beads. Biosens Bioelectron 46:37–43
Duraker N, Celik AN, Gencler N (2002) The prognostic significance of gastric juice CA 19–9 and CEA levels in gastric carcinoma patients. Eur J Surg Oncol 28(8):844–849
Suwa H, Ohshio G, Okada N, Wang Z, Fukumoto M, Imamura T et al (1997) Clinical significance of serum p53 antigen in patients with pancreatic carcinomas. Gut 40(5):647–653
Kishikawa H, Nishida J, Ichikawa H, Kaida S, Takarabe S, Matsukubo T et al (2011) Fasting gastric pH of Japanese subjects stratified by IgG concentration against Helicobacter pylori and pepsinogen status. Helicobacter 16(6):427–433
Acknowledgements
This work was supported by Chinese 973 Project (Grant No. 2010CB933902), the National Natural Science Foundation of China (Grant No. 81225010, 20803040, 81028009, and 31170961), 863 Project of China (2012AA022703), Shanghai Science and Technology Fund (No. 13NM1401500, 15441904800).
Author information
Authors and Affiliations
Corresponding authors
Additional information
Competing Interests
The authors declare that they have no competing interests.
Authors’ Contributions
Yao Xie and Xiao Zhi performed the experiments and co-wrote the manuscript. Haichuan Su and Zhen Yan carried out collection of serum specimens of gastric cancer patients. Kan Wang and Jingpu Zhang analyzed the experimental data. Nongyue He, Di Chen, and Daxiang Cui designed the experiments. All authors read and approved the final manuscript.
Yao Xie and Xiao Zhi contributed equally to this work.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Xie, Y., Zhi, X., Su, H. et al. A Novel Electrochemical Microfluidic Chip Combined with Multiple Biomarkers for Early Diagnosis of Gastric Cancer. Nanoscale Res Lett 10, 477 (2015). https://doi.org/10.1186/s11671-015-1153-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s11671-015-1153-3