Article Text

Abstract
Objectives The COVID-19 pandemic highlighted concerns regarding the equity of medical care. We evaluated associations between race/ethnicity, timing of hospital presentation and outcomes of acute appendicitis (AP) and acute cholecystitis (AC) during the initial pandemic peak.
Methods Analysis was performed on a prospective, observational, multicenter study of adults with AP or AC. Patients were categorized as pre-pandemic (pre-CoV: October 2019–January 2020) or during the first pandemic peak (CoV: April 2020 through 4 months following the end of local pandemic restrictions). Patient demographics, American Association for the Surgery of Trauma (AAST) imaging/pathology grade, duration of symptoms before triage, time from triage to intervention and hospital length of stay were collected.
Results A total of 2165 patients (1496 pre-CoV, 669 CoV) were included from 19 centers. Asian and Hispanic patients with AC had a longer duration of symptoms prior to presentation during CoV than pre-CoV (100.6 hours vs 37.5 hours, p<0.01 and 85.7 hours vs 52.5 hours, p<0.05, respectively) and presented later during CoV than Black or White patients (34.3 and 37.9 hours, p<0.01). During CoV, Asian patients presented with higher AAST pathology grade for AP compared with pre-CoV (1.90 vs 1.26, p<0.01). Asian and Hispanic patients presented with higher AAST pathology grade for AC during CoV versus pre-CoV (2.57 vs 1.45, p<0.01, and 1.57 vs 1.20, p<0.05, respectively). Patients with AC and an AAST pathology grade of ≥3 were at higher odds of postoperative complications (OR 4.4, 95% CI 1.0 to 18.4) and AP (OR 2.8, 95% CI 1.3 to 6.0). Asian and Hispanic patients with AC had a higher risk of postoperative complications compared to White patients (Asian: OR 3.9, 95% CI 1.2 to 12.7; Hispanic: OR 3.3, 95% CI 1.2 to 8.9).
Conclusion Asian and Hispanic patients had a longer duration of symptoms before hospital presentation during the initial COVID-19 peak, had higher odds of postoperative complications and more advanced pathologic disease.
Level of evidence III, Prognostic/epidemiological.
- appendicitis
- cholecystitis
- healthcare disparities
- healthcare quality, access, and evaluation
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The COVID-19 pandemic highlighted previous disparities in the equity of medical care.
WHAT THIS STUDY ADDS
Asian and Hispanic patients who delayed presentation to the hospital displayed higher pathologic grade and were more likely to experience postoperative complications.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Clinicians and surgeons should be aware of any patient’s personal reasons for delaying presentation or societal discrimination that could potentially impact well-being and timely access to surgical care.
Introduction
In the United States, inequalities in healthcare are complex and multifactorial. The vulnerability of socioeconomically disadvantaged groups was exacerbated by the onset of the COVID-19 pandemic which imposed additional challenges on under-represented minorities already at higher risk of poor health outcomes. Socioeconomic disparities have imposed challenges on under-represented groups to adhere with the Centers for Disease Control social distancing recommendations. Crowded living conditions due to financial difficulties, reliance on public transportation and the disproportionate incarceration of black Americans are among the factors that made underserved minorities more vulnerable to COVID-19 infection.1 Black patients were also found to have a higher incidence of in-hospital mortality due to COVID-19 compared with White patients, even when controlling for sociodemographic and clinical presentation on admission.2
During the COVID-19 pandemic, patients from under-represented racial groups also suffered worse outcomes for non-COVID-19-related conditions highlighting pre-existing disparities in healthcare access and differences in ability to socially distance at work and home.3 4 Medically necessary non-emergent surgeries were more likely to be performed on White patients with private insurance compared with any other group during the pandemic.3
The COVID-19 pandemic exacerbated existing disparities in healthcare utilization and access beginning in March 2020, when COVID-19 cases were increasing, and hospital restrictions began. Emergency departments saw 42% fewer patients between March and April 2020, in comparison to the same time frame in 2019 due to the state of emergency declared by the US government.4 This decline is thought to have led to an increase in morbidity and mortality for non-COVID-19 conditions such myocardial infarction and transient ischemic attacks.5–7
In this study, we report the first investigation of the impact of race and ethnicity on emergent surgery for acute appendicitis (AP) and acute cholecystitis (AC) during the COVID-19 pandemic.
Methods
Data/study population
We performed a post hoc analysis of a prospective, observational, multicenter study of adults with confirmed or suspected AP or AC. Patients were categorized as admitted pre-pandemic (pre-CoV: October 1, 2019–January 31, 2020) or during the first pandemic peak (CoV: April 2020 through 4 months following the end of local pandemic restrictions). Data were collected from 19 participating urban and rural hospitals located throughout the USA. Patients <18 years of age were excluded. No interventions were performed for the purpose of the study and the patients underwent evaluation and treatment as deemed necessary by the surgical team at each institution.
Data collection and outcomes
We collected data on patient age, sex, race/ethnicity (self-reported in the medical records as White, Black, Asian or Hispanic), pre-existing medical comorbidities, initial laboratory results on admission, duration of symptoms prior to hospital triage in hours, time between hospital triage and initial intervention in hours, and American Association for the Surgery of Trauma (AAST) imaging and pathology grade.8
Primary outcomes included hospital length of stay (LOS) and incidence of one or more postoperative complications. Postoperative complications included surgical site infection, intra-abdominal abscess, wound complications, bleeding, bile leak, retained stones, multiorgan failure, sepsis, bacteremia, catheter-associated urinary tract infection, anastomotic leak, postoperative ileus, Clostridium difficile infection, hospital-acquired pneumonia, acute respiratory distress syndrome, acute kidney injury, deep vein thrombosis, pulmonary embolism, myocardial infarction, congestive heart failure, supraventricular AV nodal arrhythmia, ventricular arrhythmia, duct injury, and small bowel obstruction. All complications were defined according to the Common Terminology Criteria for Adverse Events.9
Data management and statistical analysis
Patient data were collected and stored on a Health Insurance Portability and Accountability Act (HIPPA) compliant RedCap server managed by the University of Alabama Birmingham. Patients with missing variables were excluded. All statistical analyses were performed using GraphPad Prism V.9.2.0 (GraphPad Software, San Diego, California, USA). Data are presented as mean±SEM with range for continuous variables, unless otherwise indicated. Comparison between two groups for continuous variables was performed using unpaired t-tests and an analysis of variance (ANOVA) test was conducted when comparing more than two groups.
A multivariate logistic regression was performed to assess the relation between the incidence of one or more postoperative complications and the explanatory variables for patients with AC: study group (pre-Cov and CoV), age, sex, race/ethnicity, imaging AAST severity grade, pathologic AAST severity grade, body mass index (BMI), hypertension, diabetes mellitus, peripheral vascular disease, coronary artery disease, congestive heart failure, current smoker, alcohol abuse, substance abuse, cerebrovascular accident (CVA), chronic obstructive pulmonary disease (COPD), history of myocardial infarction, other chronic pulmonary disease, and peptic ulcer disease. Similarly for patients with AP, the previous multivariate logistic regression model was modified to include the total Alvarado score as an explanatory variable. Data were checked for multicollinearity with the Belsley-Kuh-Welsch technique. Heteroskedasticity and normality of residuals were assessed respectively by the White test and the Shapiro-Wilk test. P values <0.05 were considered significant.
Results
Demographic data
A total of 2165 patients (1134 female, 1031 male; mean age 45.03 years) were included with 1231 AP (835 pre-CoV, 396 during CoV) patients and 934 AC (661 pre-CoV, 273 during CoV) patients. Patient characteristics are shown in tables 1 and 2.
Patient characteristics of suspected or confirmed acute appendicitis
Patient characteristics for suspected or confirmed acute cholecystitis
Duration of symptoms before hospital triage
Acute appendicitis
Overall, patients with AP waited significantly less time before hospital triage during CoV compared with pre-CoV (39.86 (2.71) vs 52.76 (3.05) hours, p<0.01), and there were no significant differences between races/ethnicity in the duration of symptoms prior to hospital triage (figure 1A). Mean time to triage during pre-CoV versus CoV was not statistically significantly different for Asian (58.58 (10.74) vs 31.07 (6.19), p=0.13), Black (68.91 (13.36) vs 59.47 (19.86), p=0.97), or Hispanic patients (58.20 (9.32) vs 48.58 (7.68), p=0.56). However, White patients had a significantly longer mean duration of symptoms before hospital triage pre-CoV compared with the CoV period (48.73 (3.26) vs 37.71 (3.59), p<0.05) (figure 1A).

Duration of symptoms in hours: patients with acute appendicitis (A) and acute cholecystitis (B) experienced before presenting to the emergency room, stratified by patient race, ethnicity and pre-CoV or CoV group.
Acute cholecystitis
For the entire AC cohort, there was no significant difference in the mean time to presentation during CoV versus pre-CoV (49.61 (2.99) vs 42.73 (3.62), p=0.19). For the pre-CoV period, duration of symptoms before hospital triage was similar between races/ethnicities (figure 1B). However, during CoV, Asian and Hispanic patients had a significantly longer mean duration of symptoms before hospital triage compared with pre-CoV (Asian: 37.52 (6.69) vs 100.6 (40.88), p<0.01; Hispanic: 69.13 (9.57) vs 85.76 (26.95), p<0.01) (figure 1B).
AAST imaging grade
Acute appendicitis
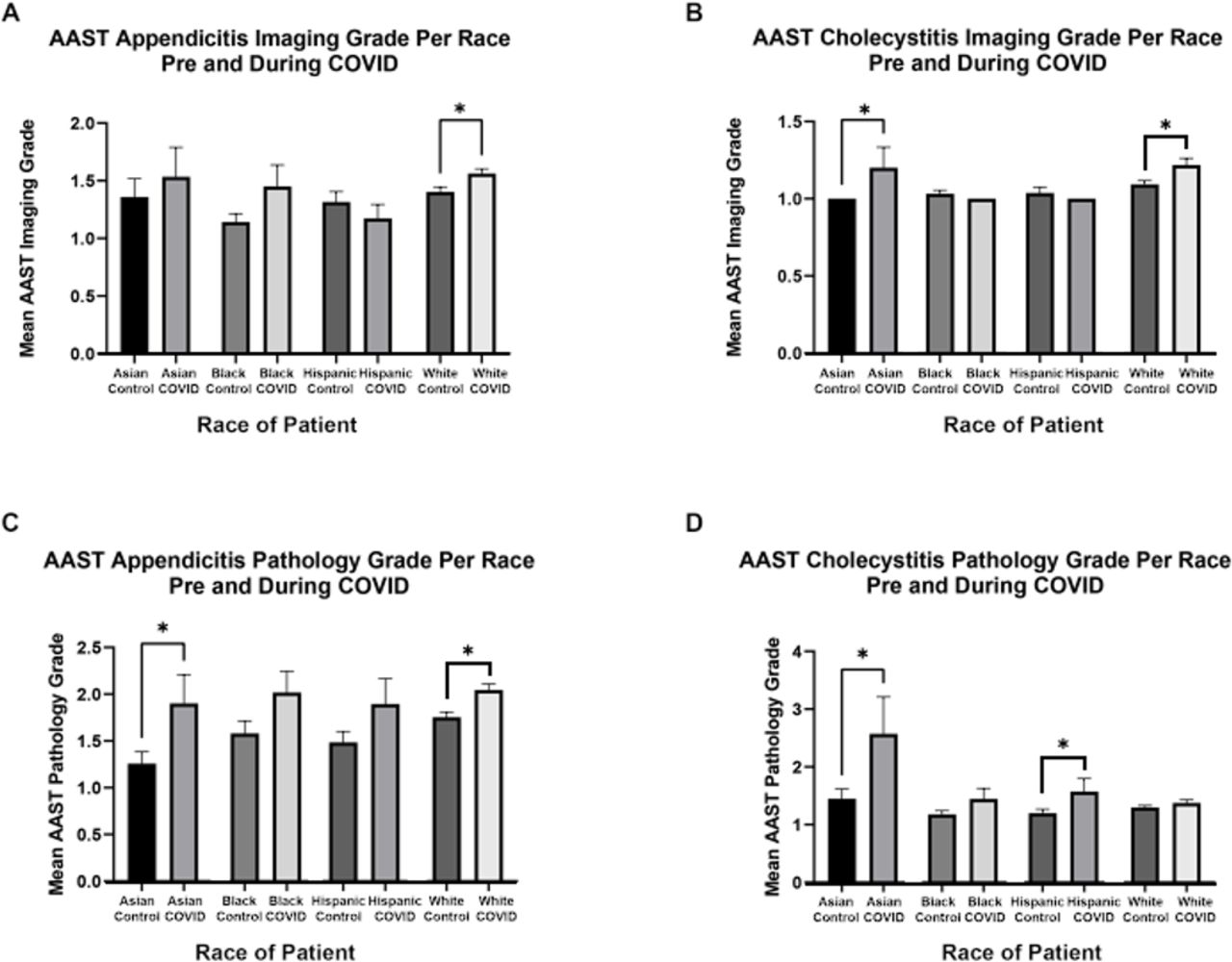
The AAST imaging grade for all patients significantly increased for AP during CoV compared with pre-CoV (1.36 (0.03) vs 1.78 (0.05), p<0.0001). There was no significant difference in the AAST imaging grade between races/ethnicities during both pre-CoV and CoV (figure 2A). When considering individual races, there was a significant increase in the mean AAST imaging grade among White patients during CoV compared with pre-CoV (1.40 (0.04) vs 1.56 (0.04), p<0.01).
{kind=link}
{kind=link}
American Association for the Surgery of Trauma (AAST) radiographic imaging severity grading for patients with acute appendicitis (A) and acute cholecystitis (B). AAST pathologic severity grading for patients with acute appendicitis (C) and acute cholecystitis (D). Data were stratified by patient race, ethnicity, and pre-CoV or CoV group.
Acute cholecystitis
The AAST imaging grade for all patients with AC significantly increased during CoV compared with pre-CoV (1.07 (0.02) vs 1.16 (0.03), p<0.0001). There was no significant difference in the mean AAST imaging grade between races/ethnicities during pre-CoV and CoV. However, there was a significant increase in the AAST imaging grade for Asian and White patients during CoV compared with pre-CoV (Asian: 1.00 (0.01) vs 1.20 (0.13), p<0.01; white: 1.09 (0.02) vs 1.22 (0.04), p<0.01) (figure 2B).
AAST pathology grade
Acute appendicitis
The AAST pathology grade for all patients significantly increased for AP during CoV compared with pre-CoV (1.67 (0.05) vs 2.04 (0.06), p<0.01). There were no significant differences in AAST pathology grade between races/ethnicities for AP during pre-CoV or CoV (figure 2C). Comparing pre-CoV versus CoV by race/ethnicity revealed a significant increase in AAST pathology grade for Asian and White patients during the CoV period (Asian: 1.26 (0.13) vs 1.90 (0.29), p<0.01; white: 1.75 (0.05) vs 2.04 (0.06), p<0.001) (figure 2C).
Acute cholecystitis
The AAST pathology grade for all patients significantly increased for AC during CoV compared with pre-CoV (1.28 (0.03) vs 1.4 (0.05), p<0.05). There were no significant differences in AAST pathology grade between races/ethnicities during pre-CoV (figure 2D). However, Asian and Hispanic patients experienced significantly increased AAST pathology scores during CoV compared with pre-CoV (figure 2D). Additionally, during CoV, Asian patients had significantly higher AAST pathology grades compared with all other races/ethnicities (p<0.001) (figure 2D).
Time from hospital triage to initial intervention
Acute appendicitis
There was no significant difference in mean time from hospital triage to initial intervention pre-CoV versus CoV for AP (28.10 (7.08) vs 27.98 (8.02), p=0.99) (online supplemental figure 1A). Comparing the time from hospital triage to initial intervention between races/ethnicities showed no significant differences during pre-CoV and CoV (p=0.74 and p=0.90, respectively) (online supplemental figure 1B). There was also no significant difference within each race/ethnicity during CoV compared with pre-CoV (online supplemental figure 1B).
Supplemental material
Acute cholecystitis
There was a significant increase in mean time from hospital triage to initial intervention for AC during CoV versus pre-CoV (43.88 (5.67) vs 34.48 (1.59), p<0.05) (online supplemental figure 1C). There were no significant differences between races/ethnicities for the time from hospital triage to initial intervention during pre-CoV or CoV (online supplemental figure 1D). There was also no significant difference within each race/ethnicity for pre-CoV versus CoV (p=0.88 and p=0.73, respectively) (online supplemental figure 1D).
Length of hospital stay
Acute appendicitis
The hospital LOS for patients with AP significantly decreased during CoV compared with pre-CoV (3.17 (0.11) vs 2.77 (0.13), p<0.05) (online supplemental figure 2A). There were no significant differences in LOS between race/ethnicity for AP or AC during pre-CoV or CoV (p=0.10 and p=0.23, respectively) (online supplemental figure 2B).
Supplemental material
Acute cholecystitis
There was no significant change in hospital LOS during CoV compared with pre-CoV for patients with AC (4.88 (0.19) vs 5.38 (0.40), p=0.21) (online supplemental figure 2C). There were no significant differences in LOS between races for AC during pre-CoV or CoV (p=0.53 and p=0.30, respectively) (online supplemental figure 2D).
Postoperative complications
Acute appendicitis
In multivariate analysis for patients with AP, age (OR 1.03, 95% CI 1.01 to 1.05), imaging AAST severity grade ≥3 (OR 2.57, 95% CI 1.21 to 5.46), pathologic AAST severity grade ≥3 (OR 2.8, 95% CI 1.3 to 6.0) and coronary artery disease (OR 4.91, 95% CI 1.45 to 16.7) were associated with an increased incidence of one or more postoperative complications (table 3). There was not a significant risk of postoperative complications based on the study period (pre-CoV vs CoV) (p=0.23).
Postoperative complications for patients with acute appendicitis
Acute cholecystitis
In multivariate analysis for patients with AC, Hispanic race/ethnicity (OR 3.29, 95% CI 1.22 to 8.88), Asian race (OR=3.88, 95% CI 1.18 to 12.74), and pathologic AAST severity grade ≥3 (OR 4.36, 95% CI 1.03 to 18.39) were associated with an increased incidence of one or more postoperative complications (table 4). There was not a significant risk of postoperative complications based on the study period (pre-CoV vs CoV) (p=0.61).
Postoperative complications for patients with acute cholecystitis
Discussion
Our analysis of patients presenting with AP and AC to hospitals across the USA revealed significant variations in time to hospital triage based on race/ethnicity during the pandemic. We found that Asian and Hispanic patients both had increased duration of symptoms for AC prior to hospital triage and increased AAST pathology grading. Additionally, Asian and Hispanic patients had a higher AAST pathology grade for AC compared with all other races/ethnicities during CoV. For AC, Hispanic and Asian patients and AAST pathologic grading were associated with increased rates of postoperative complications. There was no difference in time from hospital triage to initial intervention between race/ethnicity. These consistent differences across race/ethnicity for AC were not seen for AP. Both Asian and White patients had an increase in the AAST pathology grading for AP during CoV compared with pre-CoV. AAST imaging and pathologic grading were associated with increased rates of postoperative complications for AP but race/ethnicity and pre-CoV/CoV were not associated with postoperative complications.
To further investigate factors that could have led to patients developing more advanced pathologic AAST grades during the pandemic, we evaluated the time from hospital triage to initial intervention. There was a significant increase in the time from triage to initial intervention for patients with AC during CoV. However, we did find it encouraging that there were not any significant differences in time from hospital triage to initial intervention between racial/ethnic groups for either time point for both AC and AP, thus once patients reached the hospital, they received equitable levels of medical care. The reasons for this delay are not able to be answered by our study but possibilities include an increased usage of medical therapy, increased waiting time for available operating rooms, time to receive a negative COVID-19 test or staffing concerns during the COVID-19 pandemic.
The changes within our healthcare system and surgical options available to patients during the COVID-19 pandemic are well described in the literature. Up to 15% of adults delayed or were unable to receive elective procedures or surgeries during the COVID-19 pandemic.10 Among those who delayed care, almost 60% experienced negative health consequences as a result.10 The major contributing factors for delaying medical or surgical care were as follows: (1) fear of contraction of COVID-19, (2) inability to get an appointment or find a physician who would see them, and (3) financial concerns.10 11 Other studies have shown that patients aged 18–24 years, Hispanic adults, persons with disabilities, and patients with two or more comorbidities and students are also at risk for delaying care.12
Delaying medical care, especially emergent surgery, increases the risk for poor outcomes. Specifically in patients with AP, delays to surgical care have been associated with increased rates of perforation13 with subsequent advanced pathology and postoperative complications.14 Our results showed an increase in the AAST imaging and pathology grades for AP during CoV compared with pre-CoV, and these were associated with an increased risk of complications. The association of AAST grading and pathologic severity have been established, with more advanced scoring correlating to more advanced disease in patients with AP, confirming our study results.15 However, there is ongoing work to validate the AAST grading schemas.16 17 Both Asian and White patients also had an increase in the AAST pathology grading for AP during CoV compared with pre-CoV. Our results coincide with recent studies reporting that in the early COVID-19 pandemic period, there was an overall increase in the rates of complicated and perforated appendicitis.16 17
The reason for more advanced appendicitis is unclear as patients presented earlier during CoV compared with pre-CoV with no apparent delays in treatment. Other studies have found that there was up to a 30% decrease in emergency department admissions, but an increase in acuity during the pandemic for non-COVID-19 conditions, including medical emergencies such as AP.18 19 Interestingly, one recent study reported a decreased mean time to presentation for patients with AP symptoms during CoV, as we have, but a higher proportion of patients that waited longer than 24 hours.17 The threshold for seeking care during the pandemic may have thus increased, with patients with mild appendicitis and spontaneous resolution not presenting at all while patients with more advanced disease and clinical symptoms urgently seeking medical care.20 The overlap in clinical symptoms for AP and COVID-19 such as fever, chills, diarrhea, nausea and vomiting may have also influenced patient decisions to present for care. Patients with appendicitis typically experience an abrupt onset of severe symptoms, prompting urgent evaluation, while in cases of cholecystitis, colicky pain may be more familiar and thus ignored until reaching unavoidable severity. However, it is unclear whether these factors played a role in delays to care and increased pathology at presentation.
Our study shows that Hispanic and Asian patients with AC presented to the hospital for triage and evaluation in a delayed manner during CoV compared with other races/ethnicities and warrants further evaluation. Research has demonstrated that Asian Americans have experienced increased racial discrimination and racially motivated violence since the start of the COVID-19 pandemic.21 During the pandemic, over 30% of Asian American people have reported being subjected to slurs or racist jokes, 26% have feared that someone might threaten or physically attack them, and almost 60% believe that anti-Asian sentiment has increased.22 Discrimination and racially triggered attacks have occurred in a wide variety of locations, possibly causing Asian American patients to feel vulnerable in spaces they previously deemed safe, such as hospitals and clinics. While we cannot determine if this was a factor in the delay to seeking treatment in our study, healthcare providers can continue to make the medical environment a safe space. Several suggestions include displaying health brochures translated into languages commonly spoken in the surrounding community, posting signs indicating that translators are available and increasing healthcare worker cultural competency by emphasizing training in targeted techniques such as bystander intervention and crisis de-escalation.23
Some groups of patients may have delayed medical care due to concerns of contracting COVID-19, and early on in the pandemic there were decreases in emergency department visits for non-COVID-19-related conditions. Subsequently, patients showed advanced pathologies for conditions such as myocardial infarction and stroke due to postponing emergent care.24 Establishing proper expectations for hospital visits and risks regarding COVID-19 contraction could encourage all groups of patients who are considering delaying emergent care to present to the hospital for necessary intervention. Methods to motivate patients in need of acute medical attention include online or offline information sharing about the status of emergency department availability and protocols in place to protect patients from COVID-19 exposure.24
There are several limitations to this study. The centers included in the study are from across the USA, but may not all have been equally impacted by the COVID-19 pandemic. This study was not designed to specifically address differences in race or ethnicity as it captures only the recorded race or ethnicity and not the true diversity. Thus, we may not have accurately captured individuals that identify as multiple races or ethnicities. As a retrospective database study, we were unable to ask the delays in presentation or other factors contributing to their timing of presentation to the hospital. Data collection did not include the patient’s primary language, which is a factor that may influence treatment. We also did not capture those with milder forms of abdominal pain that may have been AP or AC and stayed at home or were seen in other settings and treated with non-operative management. There is also the possibility of recall bias when asking patients to report duration of symptoms. Finally, the percentage of Asian and black patients was much smaller than Hispanic and White. Depending on the region of the country or populations that each hospital serves, these percentages may not be reflective of all geographic areas; therefore, our results may not be generalizable to other study populations.
In summary, our post hoc analysis of an EAST prospective, observational, multicenter cohort study of patients with suspected or diagnosed AC or AP showed significant differences in race/ethnicity with respect to the amount of time patients waited before hospital triage, AAST pathology grade and postoperative complications during the early COVID-19 pandemic. The reasons for delays in presentation cannot be determined by this database and further research is needed to understand the reasons for delayed presentations in Asian and Hispanic patients. However, we as clinicians and surgeons should be aware of any patient’s personal reasons for delaying presentation or societal discrimination that could potentially impact well-being and timely access to surgical care.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Retrospective review of patient data that comprise this article was approved by the Loma Linda University Institutional Review Board in November 2021 (IRB5210047). The Loma Linda University Institutional Review Board has waived the requirement for individual patient consent for this analysis.
Acknowledgments
We would like to thank the contributors to the EAST Management of Appendicitis and Cholecystitis during COVID (MACC) Group: Majid Chammas MD, Russell Griffin PhD, Talar Vartanoglu Aktokmakyan MD, James M Bardes MD, Stephen Barnes MD, Bishwajit Bhattacharya MD, Rachel L Choron MD, Courtney Collins MD, Amanda Cooper MD, Deidre V Dillon BS, Tanya Egodage MD, Eric W. Etchill MD, Kelsey Fletcher MD, Perrone Gennaro, Mario Giuffrida, Britney R Harris, Alistair Kent MD, Mariuxi Manukyan MD, Matthew Martin, MD, Francesk Mulita, Michail Vailas MD, Caroline Neff MD, Rick O’Connor, Marisa A O’Neill DO, Amelia M Pasley DO, Asanthi Ratnasekera DO, Samantha L Roche MD, Alexandra Rooney MPH, Sirivan Suon Seng MD, Victoria Sharp DO, David P Stonko MD, Madhu Subramanian MD, Amanda L Teichman MD, Brett Tracy MD, Zachary Warriner MD, D. Dante Yeh MD.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at This work was presented at the 81st Annual Meeting of AAST and Clinical Congress of Acute Care Surgery.
Contributors NMW, SB, BC and RG designed this study. NMW, AD and SM searched the literature. NMW, SB, BC and RG collected the data. NMW, AD and SM analyzed the data. All authors participated in data interpretation and manuscript preparation. NMW is acting as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.