Article Text

Abstract
In patients with severe theophylline toxicity charcoal haemoperfusion is the recommended method for rapid reduction of serum theophylline levels. However, access to this technique is limited in most hospitals. This case report shows that continuous venovenous haemofiltration, a technique available in most hospitals, is an effective alternative to charcoal haemoperfusion.
- venovenous haemofiltration
- theophylline toxicity
Statistics from Altmetric.com
Case report
A 53 year old woman was admitted to hospital with severe theophylline toxicity after taking 22.4 g (56 × 400 mg) of slow release theophylline tablets. Following admission she had a persistent sinus tachycardia (250 beats/min) resulting in left ventricular failure, intractable vomiting with haematemesis, hypokalaemia (K+ 2.6 mmol/l), and tremor. Serum theophylline levels continued to increase during the first 24 hours after admission so she was transferred to the intensive care unit (ICU) where she had a tonic-clonic seizure, aspirated, and required intubation and ventilation.
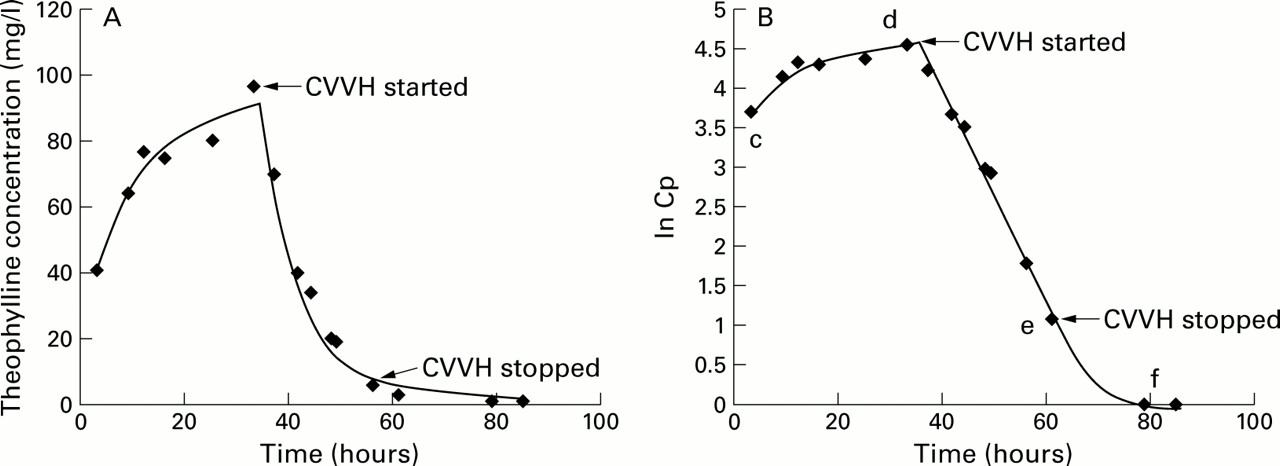
Our previous experience suggested that haemofiltration had been beneficial in two other patients with theophylline toxicity. Treatment with continuous venovenous haemofiltration (CVVH) was started in this patient 32 hours after the initial theophylline ingestion. A Gambro HFM-10 haemofilter with a polyamide filter (1.4 m2) was used, with an average ultrafiltration rate of 25 ml/min. Haemofilter circuits were primed with a bolus of 5000 units heparin and clotting was subsequently prevented with 1000 units heparin per hour. Sequential assays of serum theophylline levels were taken and measured using a high performance liquid chromatography (HPLC) assay. Theophylline levels were plotted against time before, during, and after haemofiltration (fig 1A). The natural logarithm of these values was also plotted against time to predict the patient's theophylline pharmacokinetics (fig 1B).

{kind=link}
(A) Theophylline concentration (mg/l) before, during, and after CVVH. (B) Natural logarithm of theophylline concentration plotted against time. Before (c–d) and after (e–f) CVVH the pharmacokinetics of theophylline were non-linear. During (d–e) CVVH the pharmacokinetics were linear with an elimination constant (K) of 0.118/h (slope of d–e) and an estimated half life of 5.87 hours.
Twelve hours after the onset of haemofiltration the patient's vomiting had settled and she was started on oral activated charcoal (50 g four hourly). She had no further complications and haemofiltration was stopped after 24 hours. Theophylline levels fell rapidly from 96.4 mg/l at commencement to 6 mg/l on cessation of CVVH (fig 1A). After a further 24 hours she was discharged from the ICU and made a full recovery.
THEOPHYLLINE ABSORPTION AND CLEARANCE
Theophylline is rapidly absorbed and, because of its short half life (1.4–12.8 hours), sustained release preparations are often used. In an overdose sustained release may result in toxicity for up to 24 hours after ingestion.1 Theophylline is metabolised by the cytochrome p450 enzyme system in the liver.2 Its metabolism can be described as biphasic pharmacokinetics or capacity limited metabolism. At normal and low therapeutic doses metabolism is linear and obeys first order kinetics.3 At higher doses, with concentrations at the top of the therapeutic range and in overdose, the enzyme system becomes capacity limited and results in non-linear or zero order kinetics.4 The interpretation of overdose pharmacokinetics with slow release formulations such as theophylline is further complicated by continued drug absorption which will prolong the apparent half life.5
The maximum metabolic capacity of the enzyme system in 24 hours (Vmax) of theophylline is 1630–4397 mg/day.6 Our patient took 22 400 mg of theophylline, a dose well in excess of Vmax, and the enzyme system would be saturated resulting in non-linear pharmacokinetics. The increasing theophylline concentration before haemofiltration, which peaked at 96.4 mg/l (therapeutic range 10–20 mg/l) at 33 hours, reflects the zero order kinetics and the continued absorption of the slow release preparation (fig 1). These two factors prevent prediction of total body clearance. However, even if we assume that the Vmax was 4397 mg/day, the apparent theophylline half life before haemofiltration could have been as long as five days. During haemofiltration there was a rapid change from non-linear to linear kinetics (fig 1B). The elimination rate constant (K) on the haemofilter was 0.118/h (slope of the linear decay in fig 1B). The apparent half life for theophylline on the haemofilter is estimated at 5.87 hours. Increasing the ultrafiltration rate, which was not possible due to technical problems, would have reduced the apparent half life further.
Discussion
Theophylline is an important component of treatment for the management of reversible airways disease. Overdoses usually occur in patients with respiratory disease and management will often involve the respiratory physician. Toxicity can occur at levels as low as 15 mg/l.4 Severe toxicity (>80 mg/l) causes cardiac arrhythmias, hypotension, nausea, vomiting, and tremor.1Convulsions, rhabdomyolysis, and acute renal failure can occur.1 Laboratory tests typically reveal hypokalaemia, hypercalcaemia, respiratory alkalosis, and metabolic acidosis.1
Currently recommended techniques to increase theophylline clearance are oral activated charcoal and charcoal haemoperfusion. Oral charcoal can double the rate of clearance7 and is recommended in any overdose greater than 1 g.1 Charcoal haemoperfusion is recommended if there are persistent convulsions, intractable vomiting, haemodynamic instability, rapidly deteriorating condition, or theophylline levels greater than 80 mg/l.1Haemoperfusion requires that blood is passed over semipermeable microcapsules containing absorbants such as activated charcoal in a suitable extracorporeal circuit. It removes protein bound and middle sized toxins.7
Haemofiltration involves the passage of blood down one side of a semipermeable membrane which allows water and solutes with a molecular weight up to 40 000 to pass across the membrane by convective flow, as in glomerular filtration.8 The rate of removal of such a solute is proportional to its concentration in the blood and independent of its size.8 The advantage of haemofiltration over haemoperfusion and haemodialysis is that it can be performed for long periods in haemodynamically unstable patients, can remove solutes with a relatively large molecular mass (up to approximately 15 000 Da), is more readily accessible in most hospitals, and costs less.
In theory, haemofiltration should benefit patients with toxic theophylline levels because the theophylline molecule has a low molecular mass (180 Da), a low volume of distribution (<1 l/kg), single compartment kinetics and a low endogenous clearance (<4 ml/min/kg), and is not heavily protein bound (∼40%).2 The use of haemofiltration in the treatment of theophylline toxicity has not been reported previously (Medline and Embase literature search). One report has described increased aminophylline clearance in an asthmatic patient with acute renal failure who required higher doses of aminophylline to achieve therapeutic levels when on continuous arteriovenous haemofiltration.9
Charcoal haemoperfusion is claimed to achieve the highest rate of theophylline removal with an expected fourfold increase in clearance.3 In this case, the rate of theophylline clearance from the body was significantly increased during haemofiltration by the associated change from linear to non-linear kinetics. This effect explains the patient's rapid recovery from a near fatal condition to discharge from the ICU within 24 hours. It is impossible in this case to predict the exact clearance before haemofiltration due to the combination of zero order kinetics and the continued absorption of the slow release preparation. Nevertheless, clearance was increased by at least fourfold.
Most physicians have little immediate access to the technique of charcoal haemoperfusion. In contrast, haemofiltration is readily available in most hospitals in the ICU. In combination with oral activated charcoal, it appears to be a realistic and practical alternative to charcoal haemoperfusion, particularly in the haemodynamically unstable patient with severe theophylline toxicity.
Linked Articles
- PostScript