Article Text

Abstract
Objective The risk of atrial fibrillation (AF) and stroke in patients with peripheral artery disease (PAD) is an important issue that has not been investigated adequately. Our aim with the present study was to explore trends in the incidence of AF and stroke in patients with PAD.
Methods We employed Danish nationwide registers to identify all patients with first-time diagnosis of PAD (aged ≥18 years) between 1997 and 2015. Age-standardised incidence rates per 1 000 person-years were calculated to estimate trends of AF and stroke. Risk of AF and stroke was estimated by 1 year cumulative incidence.
Results A total of 121.241 patients with first-time diagnosis of PAD were identified. The 1-year cumulative incidence of AF in patients with PAD were 1.97% for year 1997–2000, 2.63% for year 2001–2005, 2.66% for year 2006–2010 and 2.78% for year 2011–2015, respectively. The 1-year cumulative incidence of stroke in patients with PAD were 2.71%, 2.71%, 1.95% and 1.81%, for the 1997–2000, 2001–2005, 2006–2010 and 2011–2015 year groups, respectively. Likewise, the age-standardised incidence rates showed increasing trends of AF during the study period, whereas trends of stroke demonstrated a decline. During study, the initiation of cholesterol-lowering agents and clopidogrel increased markedly from 7.0% to 51.3% and 0.1% to 5.9%, whereas use of warfarin slightly dropped from 4.29% to 3.21%.
Conclusions The incidence of AF in patients with PAD has significantly increased over time, whereas a marked decline has occurred in the incidence of stroke. This may suggest that the secondary prevention strategies aimed at reducing risk of stroke are broadly effective.
- peripheral vascular disease
- atrial fibrillation
- epidemiology
- stroke
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Peripheral artery disease (PAD) is associated with increased risk of cardiovascular disease and is considered as a clinical manifestation of systemic atherosclerosis.
What does this study add?
In this retrospective register-based cohort study, the age-standardised incidence of atrial fibrillation (AF) in patients with PAD has significantly increased over time, whereas a marked decline has occurred in the incidence of stroke. Global ageing, increased focus on diagnosis and improved cardiovascular pharmacotherapy may explain the increasing incidence of AF and declining risk of stroke.
How might this impact on clinical practice?
The results from the present study highlight the enormous impact this may have on future healthcare costs and expenses. Further consideration on impact of our findings on the clinical management, as well as additional studies on the mechanistic links between PAD, AF and stroke, are required, which may aid in reducing the cardiac morbidity burden and the mortality rate in PAD population.
Introduction
Peripheral artery disease (PAD) is associated with increased risk of other cardiovascular disease and is considered as a clinical manifestation of systemic atherosclerosis.1 More than 200 million individuals worldwide are estimated to have PAD, and the prevalence continues to rise with increasing age.2 Atrial fibrillation (AF) is the most prevalent cardiac arrhythmia that is associated with increased risk of stroke.3 Recent observational studies have reported a high prevalence of PAD (12.2%–16.8%) in patients with AF.4 Indeed, PAD and AF share many common cardiovascular risk factors, including hypertension, hypercholesterolaemia and diabetes mellitus (DM).4–6 It is also well known that coexistence of AF and stable vascular disease (including PAD) substantially increases the risk of future cardiovascular events; hence, PAD is included as a prognostic factor in congestive heart failure, hypertension, age ≥75 years, DM, prior stroke, vascular disease, age 65–75 years and sex category (CHA2DS2-VASc) risk score.7 An early detection and timely treatment of clinical risk factors in patients with PAD and AF may therefore contribute in reducing the risk of cardiovascular adverse outcomes. Furthermore, it is of paramount importance to gain insight into the PAD and AF population profile and plan future interventional studies to improve the public health burden related to increased risk of stroke, morbidity and death in these patients. To the best of our knowledge, data on temporal trends of AF and stroke incidence in patients with PAD are sparse; therefore, we intended to estimate the age-standardised annual incidence of AF and ischaemic stroke in all Danish citizens diagnosed with PAD over a 20-year period.
Methods
Data sources
All Danish residents are allocated a permanent and unique civil registration number at birth or immigration that enables unambiguous cross-linkage of data across several national administrative and healthcare registers.8–10 These registers are nationwide and offer a unique possibility of conducting large-scale epidemiological studies of several endpoints with a minimum loss to follow-up. In the present study, the Danish National Patient Registry was used to retrieve information on comorbidities, prior to the PAD diagnosis date.9 This register holds information on all inpatient and outpatient treatments (recorded as International Classification of Diseases (ICD) codes) since 1978. Data on related pharmacotherapy were gained from the Danish Register of Medicinal Product Statistics (National Prescription Register) that holds information on all medicine prescribed and dispensed since 1995 according to The International Anatomical Therapeutic Chemical (ATC) classification system.9 10 These Danish registers have previously been shown to be complete and accurate with a number of well-validated diagnoses codes.9–11
Study population
The study cohort included all Danes aged ≥18 years, with a first-time diagnosis of PAD (inpatient and outpatient) over a period of 19 years spanning from 1 January 1997 to 31 December 2015. Patients with a previous diagnosis of PAD, AF and stroke were excluded at baseline. Moreover, the study subjects were censored on death, migration and at the end of study period (31 December 2015). Definition of PAD is based on European Society of Cardiology (ESC) Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases (2017) and comprises all arterial diseases (ICD-10 diagnoses codes: I70, I702, I708, I709, I738, I739, I742, I743, I744, I748 and I749) except the atherosclerotic disease of the coronary arteries, aorta and intracranial arteries.
Pharmacotherapy and comorbidity
Baseline pharmacotherapy was defined by dispensed prescriptions 180 days prior to the PAD diagnosis date. Comorbidities were established based on diagnostic codes recorded in the National Patient Registry, within 10 years of diagnosis of PAD. Hypertension was identified by hospital diagnoses for hypertension (ICD-10 codes I110-I115) or if patient was treated with at least two of the following antihypertensive agents inside a 90-day period after receiving the diagnosis: alpha-adrenergic blockers, non-loop diuretics, vasodilators, beta-blockers, calcium channel blockers and renin-angiotensin system inhibitors.12 The respective ICD and ATC codes for all examined comorbidities and pharmacotherapy are presented in online supplementary table.
Supplemental material
Outcomes
AF and ischaemic stroke were outcomes of interest and defined by the ICD-10 diagnoses codes, that is, I48, I63 and I64. Haemorrhagic stroke (I61) was not considered for this study. Patients with embolic stroke of undetermined source are predominantly coded as I64 in the Danish registers.
Statistical analysis
All statistical analyses were performed with SAS statistical software V.9.4, R statistics (R Core Team, 2016), and Join-point regression program (4.2.0.1 May 2015, National Cancer Institute, https://surveillance.cancer.gov/joinpoint/).
Baseline characteristics for cohort participants were presented as medians, frequencies and percentages. χ2 test was used to test the difference between categorical variables and t-test or the Kruskal-Wallis test for differences between continuous variables. The level of statistical significance was set as p<0.05. Risk of AF and stroke in 1 year of follow-up were presented as cumulative incidence curves with 95% CI using the Aalen-Johansen method. Risk-time (used to calculate cumulative incidence) was constituted of time since PAD diagnosis date (index) until an outcome of either AF or stroke occurred. Furthermore, age-adjusted time trends of PAD were estimated as incidence rates per 1.000 person-years (IR). Age was categorised in following age groups (years): 18–49, 50–59, 60–69 and >70.
Ethics
Data were made available in a way that individuals could not be identified. Approval from an ethics committee is not required for retrospective register-based studies in Denmark.
The study was conducted and reported in accordance with the recommendation of Strengthening the Reporting of Observational Studies in Epidemiology.13
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination of our research.
Results
After exclusion of patients with prevalent AF, PAD or stroke at baseline, a total of 121.241 patients had a first-time diagnosis of PAD between 1 January 1997 and 31 December 2015. Mean age was 68.89 (IQR 61–77 years), and 53.05% of the identified patients were male. A flow chart of the study population is illustrated in figure 1 and baseline characteristics stratified by four year-groups with 5-year intervals among patients with PAD are presented in table 1.

Flow chart of selection of the study population. PAD, peripheral artery disease.
Baseline characteristics of the study population
During study period, the initiation of cholesterol-lowering agents, acetylsalicylic acid, clopidogrel and new oral anticoagulants increased markedly from 7.0% to 51.3%, 30.1% to 47.7%, 0.1% to 5.9% and 0.0% to 0.7%, respectively, whereas use of vitamin K antagonist declined from 4.3% to 3.2% (table 1).
A total of 15.476 (12.77%) patients with PAD developed AF, and 14.671 (12.10%) patients with PAD were diagnosed with stroke the following years. The age-standardised incidence rates showed increasing trends of AF from IR 24.44 (1997) to IR 33.20 (2015) per 1.000 person-years during the study period, while trends of stroke demonstrated a decline from IR 34.51 (1997) to IR 18.58 (2015) per 1.000 person-years (figure 2). The estimated annual per cent change for the entire time period (1997–2015) increased by 1.7% (95% CI 0.8 to 2.7, p<0.0001) for AF and decreased by 3.4% (95% CI 2.4 to 4.3, p<0.0001) for stroke. All age-standardised trends were statistically significant (p<0.05).
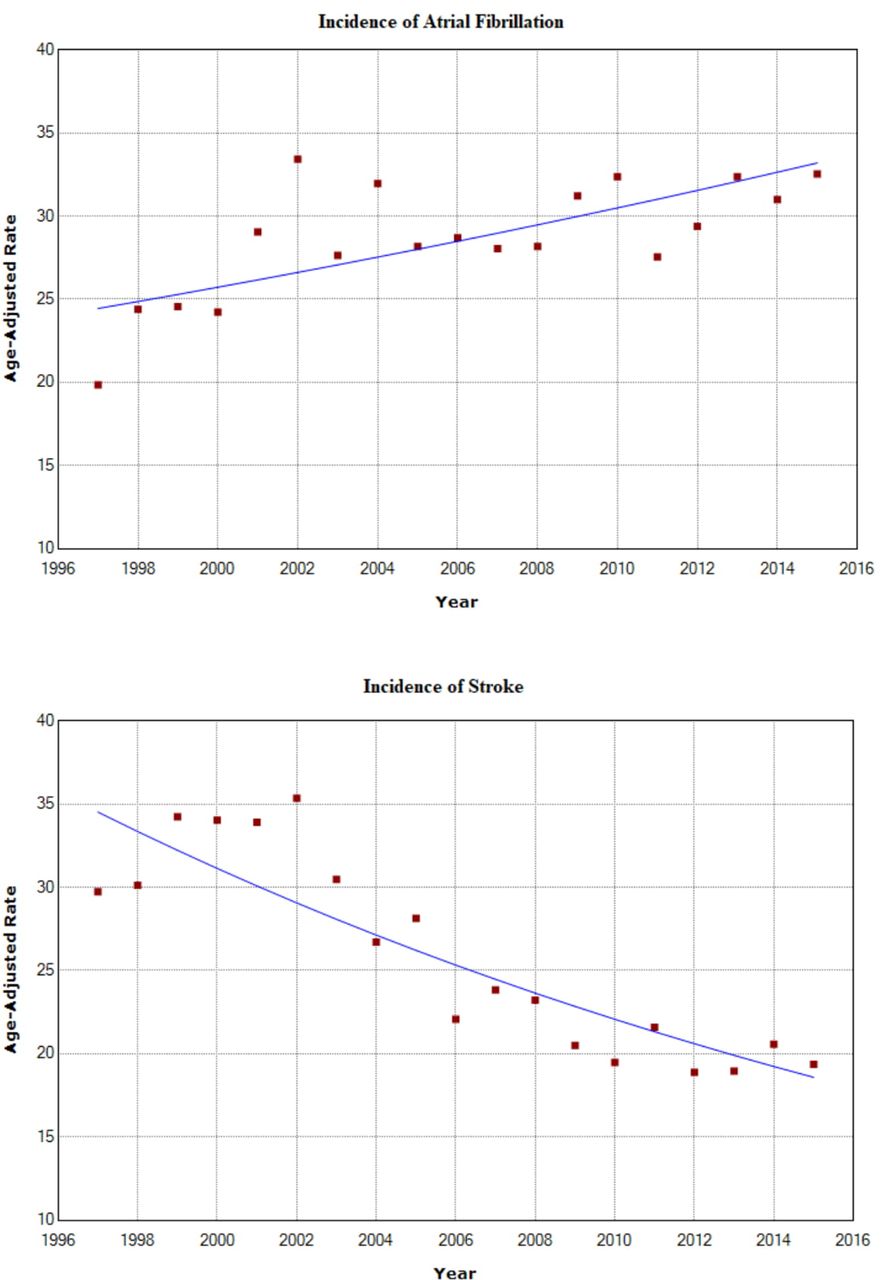
Age-standardised incidence rates per 1.000 person-years of AF and stroke in patients with PAD (y-axis) from 1997 to 2015 (x-axis). AF, atrial fibrillation; PAD, peripheral artery disease.
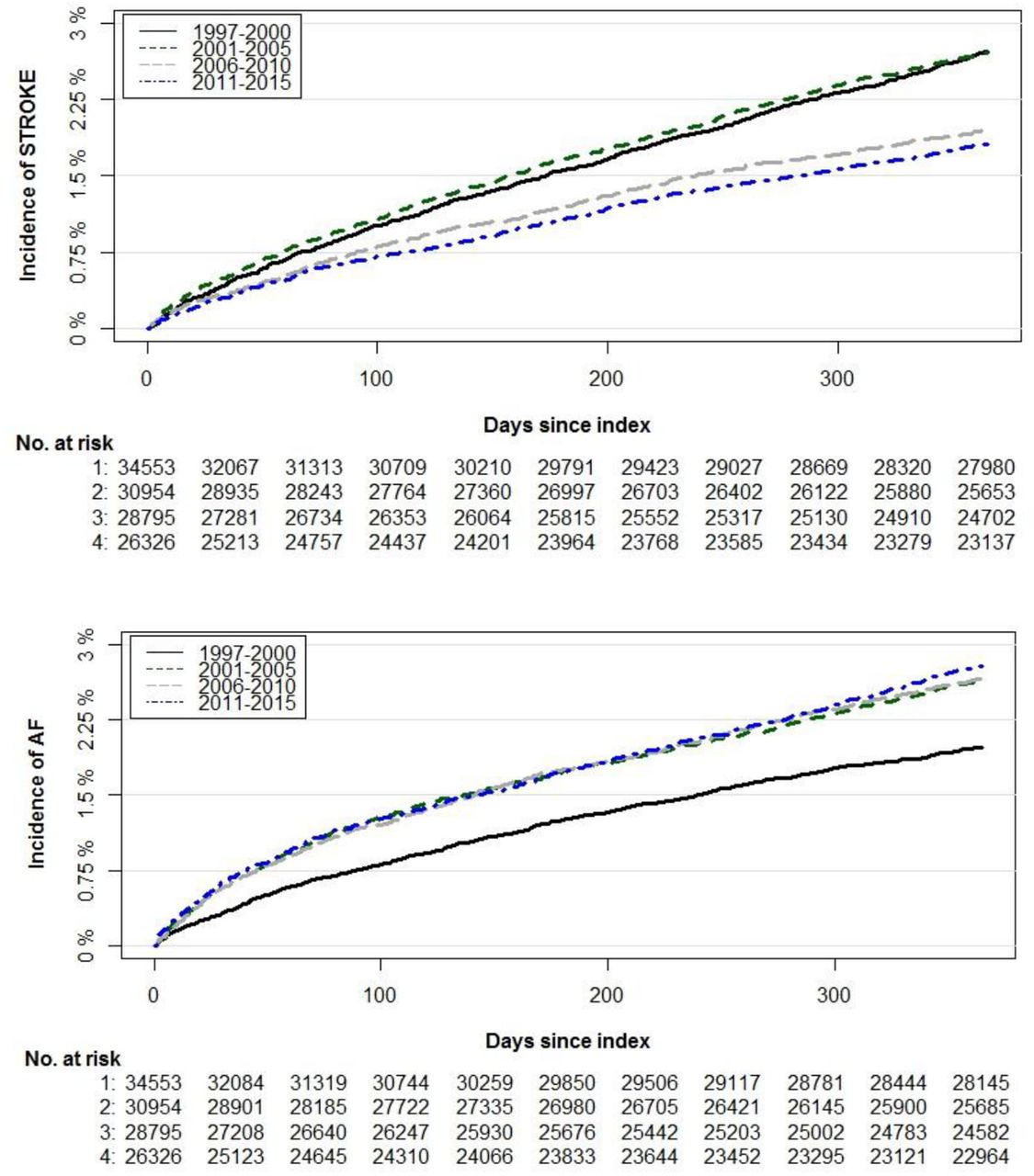
In addition, the 1-year cumulative incidence of AF in patients with PAD were estimated to be 1.97% for year 1997–2000, 2.63% for year 2001–2005, 2.66% for year 2006–2010 and 2.78% for year 2011–2015, respectively. The corresponding 1-year cumulative incidence of stroke in patients with PAD were 2.71%, 2.71%, 1.95% and 1.81%, for the 1997–2000, 2001–2005, 2006–2010 and 2011–2015 year-groups, respectively (figure 3). Furthermore, an additional subcategory analyses to examine the specific trends for PAD diagnoses codes (I70, I73, and I74) is included as supplementary data (online supplementary file 2).
Supplemental material
{kind=link}
{kind=link}
{kind=link}
Cumulative incidence curves and number of patients at risk within 1 year from first-time diagnosis of PAD to development of AF or stroke. At-risk table represents number of patients at risk of an event at given time (ie, each month for all four time periods). AF, atrial fibrillation; PAD, peripheral artery disease.
Discussion
In this Danish nationwide register-based cohort study including patients with first-time diagnosis of PAD, we examined temporal trends on risk of AF and stroke spanning over 20 years. The main finding is a significantly increased age-adjusted incidence of AF and a significant decline in the incidence of stroke along the study period. Moreover, the corresponding 1-year cumulative incidence of AF in patients with PAD showed an increasing trend, whereas the 1-year cumulative incidence of stroke in patients with PAD demonstrated a decline.
PAD is considered as a serious atherosclerosis-related disease that can lead to frequent hospitalisations, higher health economic cost, a poor quality of life and an increased mortality rate.14–16 Although PAD definition is that of atherosclerosis of the arteries outside the heart, the term is most commonly used to describe occlusive arterial disease of the lower extremities.17
Similar to other atherosclerotic diseases, PAD is associated with the presence of traditional cardiovascular risk factors, including DM, hypertension, dyslipidaemia, obesity and tobacco consumption.5 17 Moreover, along with endothelial dysfunction and hypercoagulable state, studies have linked PAD with a heightened low-grade inflammation that may contribute to increased risk of cardiovascular events.18–20 Indeed, patients with PAD are at remarkably high risk of cardiovascular and cerebrovascular diseases, which are concomitantly present in more than half of the patients with PAD.21
It is commonly known that AF is strongly correlated to atherosclerotic vascular disease.22 As PAD is one of the cardinal signs representing the presence of systemic atherosclerosis, AF and PAD often coexist.3 23 Furthermore, restricted physical activity due to intermittent claudication may aid the development of adverse conditions, such as insulin resistance, metabolic syndrome, obesity and severe depression, which confer an increased cardiovascular risk. Recent observational studies have reported a high prevalence of PAD (12.2%–16.8%) in patients with AF and an increased risk of incident AF (29%) in patients with PAD.4 Although the complex mechanism linking AF and PAD is not fully elucidated, mounting evidence has suggested an overlap of multiple common risk factors, increased levels of inflammation and prothrombic state, which leads to the susceptibility for a bidirectional relationship between the two conditions. This association between AF and PAD elicits an increase in all major adverse cardiovascular outcomes, including stroke and thromboembolic events, which makes the concurrent presence a much dangerous combination for patients with AF and PAD.3 23 In addition, PAD is also considered as an independent predictor of ischaemic stroke, which is the main reason that it is currently included in the clinical score (CHA2DS2-VASc score) of baseline assessment for newly diagnosed patients with AF.7 24 The overlap of the common risk factors among PAD, AF and stroke reflect shared pathophysiological mechanisms and a multiple-stage disease process, where presence of risk factors promotes development of atherosclerosis, diagnosis of PAD, incident AF and ultimately thromboembolic events including stroke.
Despite the well-known association and evidence on the prognostic implication of AF in PAD, there are only a few studies, if any, that have evaluated the trends of AF and stroke in patients with PAD during the past two decades. We therefore used the Danish national health and administrative registers to examine this important topic. The results from our study demonstrate an increasing incidence of AF in patients with PAD across years. This trend is supported by other studies suggesting a growing prevalence and incidence of AF linked to an early and frequent diagnosis and the shifting demographics of the general populations.25–30 For example, recent estimates from the Framingham cohort reported a 3–4 fold increase in age-adjusted incidence of AF between 1958 and 1967 and 1998 and 2007, along with temporal changes in AF-associated risk factors.31 Indeed, as people age, they are more likely to develop chronic medical conditions, including PAD and AF. In addition to ageing population and improved survival from other cardiovascular conditions, the increased awareness and initiatives to improve the detection of AF is also considered as a major contributing factor in greater incidence of diagnosed AF.26 Moreover, PAD and AF share several risk factors, for example, increased levels of inflammation, thrombosis and coagulation, which may, in part, explain the increased incidence of AF in PAD patients.18–20 Nevertheless, further research is needed to clarify the underlying mechanisms.
Furthermore, the present study demonstrates a consistent decline in the incidence of stroke during the study period of 20 years. This trend is in line with the studies demonstrating the similar lower incidence of stroke in general population.27 Patients with PAD are at increased risk of stroke due to more advanced atherosclerosis, increased prevalence of comorbidities, enhanced platelet aggregability and a reduced fibrinolytic potential.32 Preventing future ischaemic events is therefore the main objective of the PAD treatment. The observed decrease in age-standardised rates and cumulative incidence of stroke in the present study may suggest an increased and effective use of anticoagulants and antiplatelet drugs and a better control of modifiable cardiovascular risk factors, particularly hypertension, diabetes, dyslipidaemia and smoking.33 34 Interestingly, during the course of our study (ie, between 1997 and 2015), the use of cholesterol-lowering agents, antihypertensives and clopidogrel increased markedly, which supports the notion of improvement in risk factor modification strategies in high-risk population (table 1). Hypertension is the most prevalent risk factor for stroke, and it is estimated that the risk of stroke could be significantly reduce through an optimal management of hypertension.35 Consequently, the treatment guidelines have included recommendations focused on lowering blood pressure in patients with hypertension-related conditions including stroke.36 Comparable with the trends observed in the general population, we also observe an increase in use of antihypertensive treatment in patients with PAD in the present study (table 1). The similar increase has been observed in prevalence of hypertension, which has increased from 10.7% (1997–2000) to 33.7% (2011–2015). As we have defined hypertension by using diagnoses coded and/or use of at least two antihypertensive agents, this may, in part, explain the observed higher frequency. Also, this increase is in line with the existing studies showing an overall increased risk of hypertension in PAD, as well as an increase prevalence of hypertension in general population during the recent years.37–40
Taken together, besides constituting highly relevant future research questions, the results from the present study underline the importance of timely and early anticoagulation in management of patients with PAD in order to prevent risk of thromboembolic events including stroke. Of notice, PAD is often overlooked by the primary care providers as the early clinical findings are subtle and patients may not complain of the symptoms until the disease is in the advance stages. More attention should be paid to patients in whom coexistence of AF and PAD occurs, as they represent a vulnerable subgroup at a very high risk for adverse outcomes. Indeed, AF in patients with PAD may serve as a surrogate marker of more severe disease with subsequent poor cardiovascular (CV) outcomes in terms of survival and morbidity. Showing a substantial increase in AF incidence in patients with PAD, the results from the present study highlights the enormous impact this may have on future healthcare costs and expenses. Nevertheless, further consideration on impact of our findings on the clinical management, as well as additional studies on the mechanistic links between PAD, AF and stroke, are required, which may aid in reducing the cardiac morbidity burden and the mortality rate in PAD population.
Strengths and limitations
Notable strengths of the present study include a large number of unselected patients in a real-world setting, completeness of follow-up and use of validated measures of exposure and outcome. Furthermore, the Danish healthcare system is government financed that guarantees free of charge and equally accessible care for all its inhabitants, reducing confounding by variables associated with social class to a minimum.
Despite these strengths, there are also several limitations that must be acknowledged. For example, the observational nature of the study only enables to establish association and does not represent cause-and-effect relationships. Moreover, the subpopulation was identified by using diagnosis from the registers; although the registration of data in Danish registers is known to be accurate, there still might be some limitations regarding the PAD diagnoses, especially as PAD is under-reported due to the often-asymptomatic nature of the disease. Finally, the Danish population is predominately of Northern European descent, and generalisability of our findings to other ethnicities should be performed with caution.
Conclusion
The incidence of AF in patients with PAD has significantly increased over time, whereas a marked decline has occurred in the incidence of stroke. This may suggest that the secondary prevention strategies aimed at reducing risk of stroke are broadly effective. Moreover, an increased focus on earlier and adequate diagnosis and improved treatment of cardiovascular disease allowing survival with the disease may explain the increasing incidence of AF.
Acknowledgments
The study sponsors had no influence on data collection, interpretation of data, nor the final decision to submit the manuscript for publication.
References
Footnotes
Presented at The abstract of the present study has been presented as a poster at ESC Congress 2019 (Paris); however, the data have never been published in any scientific journal.
Contributors SK, TS, HD and GG designed the study. SK performed the statistical analyses and wrote the initial draft of the paper. All authors contributed equally to interpretation of data, revised the paper for important intellectual content and approved the final version of the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Danish Data Protection Agency approved the present study (ref. 2007-58-0015, int. ref: GEH-2014–018).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. Data may be obtained from a third party on reasonable request and are not publicly available.