Article Text

Abstract
Improving personality disorder (PD) care across a healthcare system is an important but complex task and one that has been endeavoured by many organisations. Oxford Health National Health Service (NHS) Foundation Trust recently received funding from the NHS Long Term Plan’s Community Mental Health Framework to improve PD care across Buckinghamshire mental health services. Therefore, Oxford Healthcare Improvement performed a system-wide diagnostic assessment of gaps in the provision of care for patients with PD and produced a list of recommendations to aid future improvement work. We used a robust and systematic approach that included, a range of quality improvement methods, the mapping of patient pathways, collection of quantitative data on the utilisation of these pathways and focus groups with staff, patients and carers. This paper summarises our mixed-method approach to show how the first stage of improving a complex mental health system could be approached. It also outlines potential areas for improvement associated with the care and treatment of patients with PD and change ideas to address these areas. These include, ensuring a specialised approach to triage and assessment for patients with PD, upskilling the workforce across the system and utilising a variety of evidence-based practices to best support the range of patient needs. As well as introducing a leadership structure to ensure and support improvement work associated with PD care and treatment. We believe our methodological approach could be used beyond improving PD care and we hope that sharing our methods will aid organisations when approaching system-wide improvement work.
- Quality improvement methodologies
- Focus Groups
- Implementation science
- Mental health
- Complexity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Personality disorders (PD) are common and challenging to treat. Studies have revealed that 1 in 20 people in the UK have a diagnosis,1 and prevalence is much higher in healthcare settings. Approximately a quarter of patients that attend primary care2 and 40% of those in community mental health services meet the criteria for PD.3 Estimates of prevalence in psychiatric inpatient settings range from 36% to 67%.4 People with PD experience poor quality of life5 and have a significantly shorter (19 years for women and 18 years for men) life expectancy than the general population.6 They are at high risk of self-harm7 and suicide.8 9
People with PD have more extensive involvement with psychiatric services than those with major depressive disorder,10 tend to have both a higher number of readmissions and shorter time between readmissions11 and more frequently attend emergency departments.12 However, there is substantial and long-standing evidence that services fail to meet the needs of this patient group. In 2003, the National Institute for Mental Health in England published ‘PD: No longer a diagnosis of exclusion’, a formative paper that drew attention to the inadequacies of PD care in healthcare services and called for improvements.4 Specifically, it called for dedicated PD services, clear care pathways and a substantial improvement in the skills, expertise, and training of mental health professionals in this area. The report also stated that people with PD were often stigmatised, both within mental health services and wider society, and that many mental health professionals were reluctant to work with them.
Dedicated services for PD are now more widely available,13 but problems remain. Patients are still not receiving care consistent with the National Institute for Health and Care Excellence guidelines14 and do not have equal access to dedicated services.13 Patients, carers and staff still believe that being given a PD diagnosis can be stigmatising, which may, in turn, lead to exclusion from services; staff may even be reluctant to make a diagnosis of PD for fear that this will disadvantage the patient.15 16 Care pathways are often unclear and fragmented, with patients falling into a gap between primary and secondary services, leading to inappropriate reliance on the emergency department at times of crisis. Staff’s negative attitudes and lack of understanding of PD continue to be stressed by patients and carers, and indeed by staff themselves. In many organisations, psychological therapies are not readily available to all patients and there is a lack of collaborative whole system working.14–18
PD care is a major focus of the recent National Health Service (NHS) ‘Five-Year Forward View for Mental Health’19 and ‘Long Term Plan’.20 However, improving PD care can be difficult due to a wide range of issues across the system and the absence of a distinct clinical pathway to guide system redesigns.14 Locally, many Trusts have carried out PD pathway/service reviews, strategies and redesigns.21 These are broadly described in various documents, but few give sufficient detail to enable others to follow their methods. An exception is a redesign reported by the Yorkshire and Humber Region, which used various methods including staff and patient focus groups, a literature review, analysis of referral and admission data for specific services and involvement events.22 Yet, the majority of work reported has not detailed their methodology, which severely limits wider learning and replication of the approach.
Oxford Health NHS Foundation Trust (OHFT) recently received funding from the NHS Long Term Plan’s Community Mental Health Framework to improve PD care across Buckinghamshire. Oxford Healthcare Improvement (OHI) carried out a comprehensive system-wide diagnostic assessment of gaps in the provision of care for working age adults (18–65) with PD. It produced a list of recommendations to aid future improvement work. Our primary aim was to use a robust and systematic approach, including a range of quality improvement (QI) methods, qualitative approaches and an in-depth quantitative analysis of services.23 This paper summarises this mixed-method approach to show how a complex mental health system can be assessed, as well as presenting potential areas of improvement for the care and treatment of patients with PD.
Methods
Our methodological approach was made up of several stages and steps, see figure 1 for an overview of these and associated timeline.

This displays each stage and step of our method and the associated order and timeline of these activties.
Preparatory tasks
Oversight team and stakeholder team identified
OHI led this project and facilitated forming an oversight and stakeholder team. The oversight team met monthly to monitor progress. The stakeholder team represented staff across OHFT and acted as the core working group for the project. See online supplemental material for a full list of those involved.
Supplemental material
Process mapping
The stakeholder group created the process map with maximal engagement from front-line staff. This displayed all possible patient pathways for patients with PD, from referral to discharge. Once completed, the process map provided a visual tool, acted as an agreed understanding of the system and aided the stakeholders in focusing on the areas of improvement.
Data collection and review
Focus groups
OHI conducted focus groups to gather a range of perspectives on PD care currently delivered throughout OHFT (see box 1 for the list of focus groups). All focus groups were conducted virtually, and notes were taken throughout. OHI used a pragmatic approach to theming the feedback. The process maps were presented in these focus groups so stakeholders could review their accuracy.
Focus groups that took place and the number of people involved
Patients with PD who have been in contact with adult services (6).
Carers of patients with PD in adult services (6).
Carers of patients in the Complex Needs Service (10).
Adult acute services staff (10).
Adult Psychological Therapies Service staff (10).
Data on the number of patients with PD in each service and receiving evidence-based therapy, length of care episodes and waiting times
To further identify the gaps in PD care across OHFT, an in-depth collection and analysis of quantitative data across various services was performed. See table 1 for details and reasons for the data collection. OHI collected data using existing datasets (for 2019–2020 to account for the impact of COVID-19), provided by services and the Clinical Record Interactive Search (CRIS), which allows access and analysis of deidentifiable data from electronic records. Details on the inclusion and exclusion criteria used for CRIS is provided in online supplemental material. This data was added to the process map, and length of care episodes/waiting times were added to a timeline.
Supplemental material
Quantitative data collected and reasons for collecting this data
Reviewing the data described in 2.c and 2.d
The stakeholder group acted as an expert panel, reviewing the findings (process map with added data, focus group themes and the timeline demonstrating the length of care and waiting times) throughout several meetings. Commonalities in the gaps in care identified across the sources were identified.
Diagnosing the gaps in care and identifying change ideas
Building on previous discussions, the stakeholders identified/prioritised the gaps in care
Following the above discussions, the stakeholder group prioritised the gaps in care, informed by the process map, focus group findings and data. Initially, the group was split into four smaller groups to discuss and convened to agree on the final list. This took place across several meetings.
Created a driver diagram based on findings from 3.f
OHI used the agreed list of gaps in care to create a driver diagram—a visual tool to identify drivers for improvement and initial change ideas.24
Change Ideas to address the gaps in care identified
The stakeholder group identified potential change ideas outside of the meetings, then met to discuss these to maximise their engagement and experiential knowledge to guide change ideas. Once agreed, they added these to the driver diagram to ensure they were fit for purpose.
Planning future improvement work based on project's findings
Workstreams identified to take forward and test the suggested change ideas
OHI presented the driver diagram to the oversight team. Workstreams and associated working groups were identified to carry out tests of change.
Results
Our results describe issues identified through the process mapping, focus group findings and the patient’s journey through the system informed by quantitative data. Finally, gaps in care are identified along with improvement ideas to address these.
Understanding patient pathways through the system
Process mapping highlighted the numerous different patient pathways and staff understanding of the current system. It also highlighted some of the apparent problems and unhelpful aspects of the current system. Please see box 2 for issues identified during the process mapping excerise and online supplemental material for the process map.
Supplemental material
Issues identified through the process mapping exercise
Limited access to support while patients wait for an evidence-based treatment.
The system contains multiple entry points, without a distinct and consistent assessment process and triaging early in the system.
Structured Clinical Management is only being delivered in some Community Mental Health Teams (CMHTs) due to COVID-19 constraints and is offered to a small number of patients due to staffing.
Access to evidence-based treatments in inpatient units is lacking.
Staff do not describe treatment options to patients, other than those offered in the Complex Needs Service (CNS; PD specialist service).
Patient and carer views on the current system
Findings from the focus groups identified a balanced view of the positives of current care and what could be improved (see box 3 for full list). Patients and carers value the support provided in primary care and non-medicalised options such as peer support, Safe Haven (OHFT’s out of hours support), and carer groups, as well as external organisations such as Samaritans. They identified that OHFT would benefit from further enhancing these services. Patients and carers raised that it is rare to receive a diagnosis early on, also identified with staff during process mapping, which has a knock-on effect throughout the patient pathway, resulting in a lack of support and ownership of care. Likewise, they stated that there is a lack of knowledge and expertise in PD outside of the CNS and variable approaches to care across services and staff.
Patient and carer views of the current system
Positives
The care received by general practitioners (GPs) is highly valued, they are viewed as very supportive and engaged. They are showing more awareness of PDs and starting to make appropriate referrals.
The CNS and talking therapies, generally, are viewed as beneficial once patients have access to them.
Carer groups are viewed as a fantastic resource, as they are very informative and supportive.
Safe Haven is useful for patients who are not in the position to use the CNS. It is beneficial for both the individual with a PD and those around them.
Peer-support workers are highly valued by patients.
Gaps in care
A formal diagnosis is lacking early in the care pathway. Patients are often misdiagnosed and/or do not receive a diagnosis until seen by the CNS.
When a formal diagnosis has not been given, patients often feel that they are being passed between services due to a lack of knowledge on who should provide care for this patient group.
If patients do have a formal or suspected diagnosis (and are not referred to the CNS) they are often excluded from services.
Patients feel in limbo when on the waiting list for CNS, due to the lack of support they receive during this time.
Staff in crisis care are underequipped to deal with a patient with PD in acute stress.
Conversations about PD and forms of self-help are avoided in CMHTs.
Need a consistent approach to PD care across services, informed by education and training.
All services need better structure and care planning to provide effective support for patients with PD.
Non-medicalised options (eg, peer support, Safe Haven and Samaritans) need to be upscaled.
Better joined up working and communication between services, families and patients is needed.
Transition from children and adolescent mental health services to adult services needs improvement.
Greater carer support and involvement is needed.
Experience of care is currently variable and depends on what staff you are allocated.
Access and waiting times for appropriate treatment needs improvement.
Staff views on the current system
There was a shared understanding of the issues with the OHFT system across staff, patients and carers. Staff also identified that the system lacked a formal assessment and triage process early on and a lack of competence on where to refer patients for the most appropriate care and how to support them throughout the patient pathway. They also highlighted that CMHTs, particularly, lacked the resources to follow best practice guidelines for PD care, for example, managing endings with services and supporting transitions through informed discussions (see box 4 for full list).
Staff views of gaps in care in the current system
The system lacks an assessment for PD at the beginning of the patients’ journey.
The system lacks a triage point for choosing the appropriate treatment option for a patient that can be revisited over time.
Staff feel undertrained on the current treatment offerings and where to refer patients depending on their level of need rather than level of risk.
Stretched CMHTs are unable to prioritise aspects of PD care for example, staff supervision, managing endings, complex case panels, multidisciplinary team care reviews.
More training for staff in understanding and caring for patients with PD is needed.
Long waiting lists for therapy mean that CMHTs are managing crises, holding risk and feeling unsupported.
CMHTs need separate specialist roles to care for patients with PD, as many staff feel undertrained and undersupported to provide effective care.
Resource for Structured Clinical Management in CMHTs is lacking.
Supportive conversations and the transfer of patients between services if needed is lacking.
Need to move away from managing patients according to risk.
Understanding the patients’ journey through the system
The quantitative data demonstrated that there are a significant number of patients with PD and how widespread they are throughout OHFT. Approximately 40% of patients within CMHTs and Crisis Response and Home Treatment Teams (CRHTTs) either had a confirmed or suspected PD diagnosis and 58%–70% in inpatient units. These figures illustrated the importance of carrying out a system-wide diagnosis of PD care and the need to recognise PD as a significant patient group in OHFT.
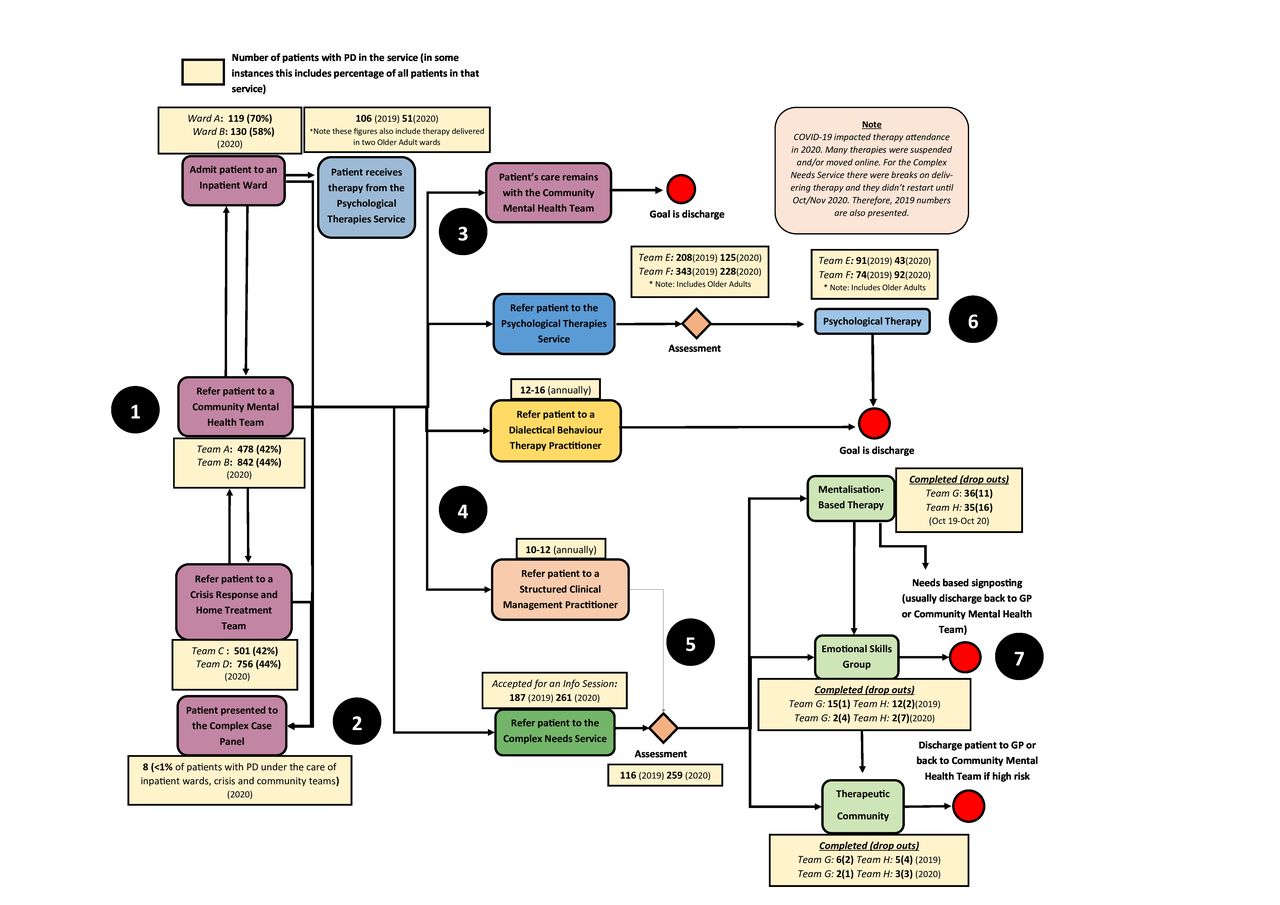
The data also substantiated the focus group findings and identified further gaps in care. It displayed that only a small proportion of patients under the care of CMHTs receive an evidence-based therapy. Additionally, less than 1% of patients under the care of CMHTs, CRHTTs and inpatient mental health units combined received a complex case panel review (an expert panel that provides guidance and advise surrounding the care of complex patients), suggesting the needed for greater utilisation of expertise to support this patient group. See figure 2 for the simplified process map with the number of patients with PD presenting at each service.
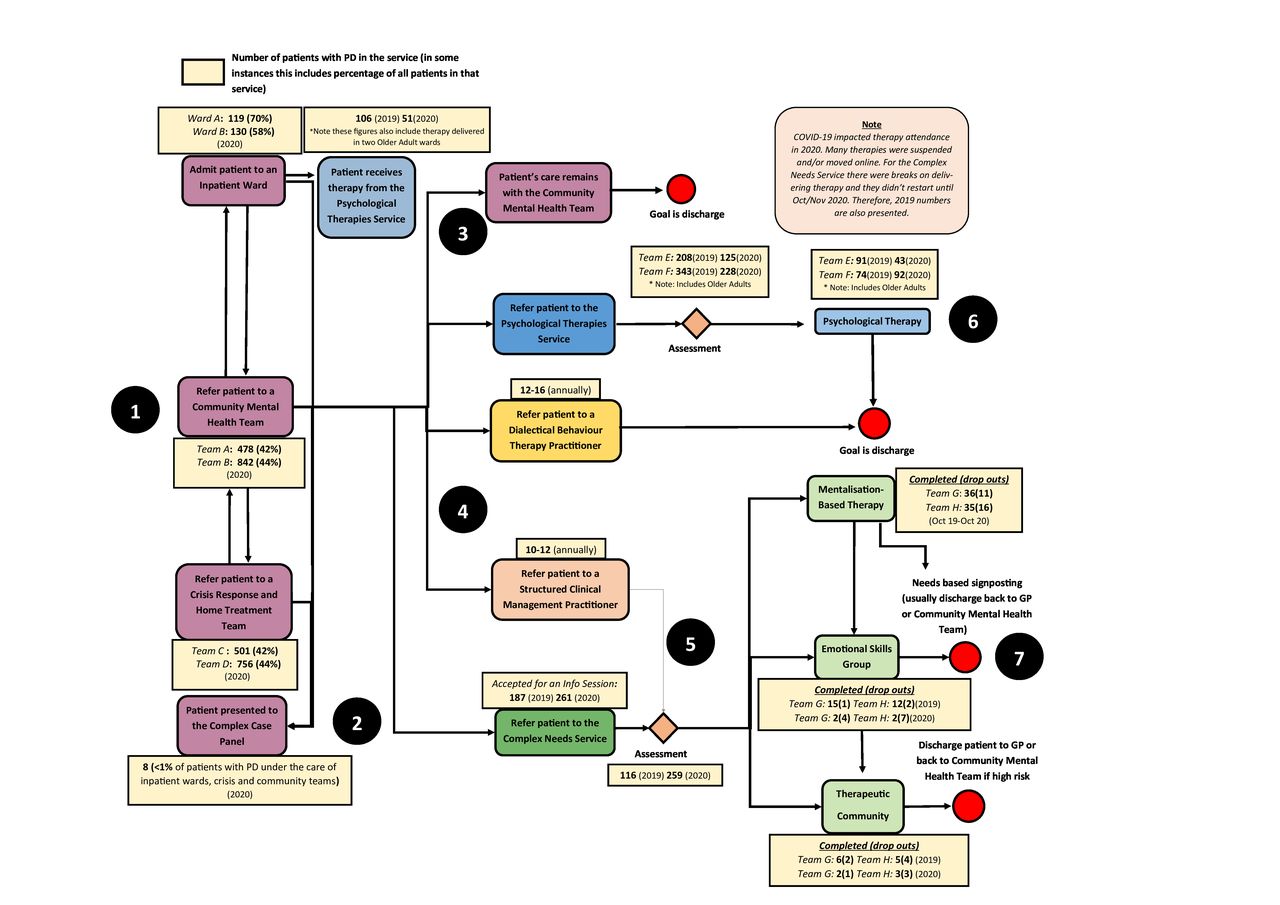
Number of patients with PD presenting across the system. GP, general practitioner; PD, personality disorder. 1. Once patients have entered the system, they can be under the care of either the Community Mental Health Teams, Crisis Response and Home Treatment Team (there are two teams for each in Buckinghamshire, covering different locations) or two of the adult acute inpatient wards. Patients can move between services depending on their need. 2. All services can refer patients to the complex case panel for help and guidance on how to most effectively provide care for particularly complex patients. 3. If patients do not need a specific evidence-based therapy, their care will remain under Community Mental Health Teams where staff will work with the patient until an agreed point, with the goal of discharge. 4. If the patient does need an evidence-based therapy, they will either be referred to the Complex Needs Service, Psychological Therapies Service or will be offered either Dialectical Behaviour Therapy or Structured Clinical Management, which are both delivered by pracitioners within the Community Mental Health Teams. 5. Patients that need further help following Structured Clinical Management, could go on to be referred for an assessment from the Complex Needs Service. 6. The Psychological Therapies Service offer a range of individual and group available to patients with PD, including cognitive behavioural, psychodynamic and mindfulness therapy. There are two teams which cover different localities. 7. The Complex Needs Service has three different offerings depending on the patients' level of need and patients can be provided with more than one if required.
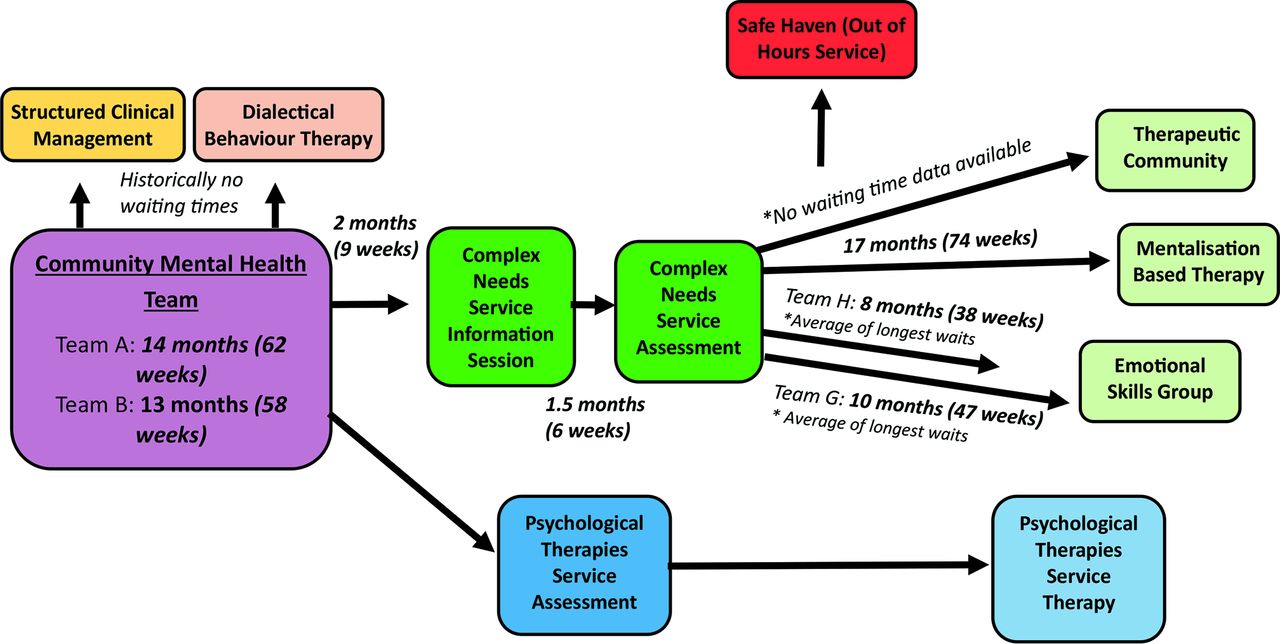
The data also demonstrated significant delays while under the care of CMHTs, including long waiting times for assessment and treatment. Safe Haven confirmed that many of the patients with PD accessing their support were on the waiting list for the CNS, emphasising the need for enhanced support for patients with PD while they wait for assessment and treatment. See figure 3 for a visual of patient pathways and waiting times.

{kind=link}
{kind=link}
{kind=link}
Possible treatment pathways from the Community Mental Health Teams and associated waits. Times displayed in the Community Mental Health Team box demonstrate the average length of care with the two teams for patients with PD. The remaining times display the average wait times unless specified otherwise. There are no waiting times displayed alongside the Psychological Therapies Service as we were unable to retrieve waiting times specifically for patients with PD.
Prioritisation of gaps in care by the stakeholder group
The stakeholders met to review the process map, focus group findings and quantitative data and establish commonalities in gaps in care identified across sources. Please see online supplemental table 1 for those gaps in care.
Supplemental material
Informed by the previous steps, the stakeholder group agreed on a final list of gaps in care which fell under two broad themes: gaps in care along the patient pathway and gaps in care relevant across the entire system. We have discussed a few examples in detail below but see box 5 for an overview of some of the main gaps in care identified. Online supplemental table 2 provides details on all the gaps in care identified and included in the final list put together by the stakeholder group.
Supplemental material
Gaps in care
Patient pathway
Inconsistent approaches to diagnosis and assessment and lack of knowledge around treatment options
Inconsistency in timing of an assessment.
Assessment and triage are risk based not needs based.
Staff lack awareness of all treatment options.
Lacking a system for choosing the appropriate treatment pathway.
Lack of evidence-based treatment and support across the patient pathway
Need to improve availability of a range of evidence-based treatments that can be accessed by all teams.
Need to increase the availability of evidence-based treatments in primary and secondary care (including patients on waiting lists for therapy).
Need timely access to evidence-based treatments as there are currently long waits for the CNS and Psychological Therapies Service.
Patients with PD are often over prescribed medication and there is a lack of guidance on appropriate prescribing for this patient group.
System-wide
Staff knowledge and support
Staff need a greater understanding on how to care for patients with PD as many staff feel ill equipped/undertrained.
Many staff feel under supported in regards to caring for patients with PD.
Need for greater utilisation and availability of expertise to support complex cases.
Culture around PD care
No ownership/responsibility of PD care throughout the system.
Lack of clear and identifiable leadership structure for PD care.
Lack of collaborative working between services across the system and shared conceptualisation of PD
Lack of supportive conversations/communication between services and transfer if needed.
No senior support for inter-service working.
Lack of consistent language in relation to PD used through the system.
Gaps in care across the patient pathway
The findings highlighted that it is rare to receive a diagnosis of PD before being seen by the CNS, and that this service receives a significant amount of potentially inappropriate referrals that could receive alternative lower-level therapy. This compounds the need for a wider range of evidence-based therapies and sources of support across the system, and results in long wait times and issues of access for this patient group.
System-wide gaps in care
It became apparent that staff working in CMHTs and CRHTTs across OHFT were unclear that patients with PD were part of their core business, despite this population constituting a significant proportion of the patients accessing these services. Services appear reluctant to take ownership of their care, sources of available expertise such as the complex case panel are being underutilised and there is a demonstrable lack of supportive conversations between services. Furthermore, a lack of understanding of PD, support structures, and resources culminat in patients with PD only receiving adequate support when accessing the CNS.
Suggested change ideas for future improvement work
Once the final list of gaps in care was agreed on, appropriate change ideas were collated. Broad themes and related change ideas are discussed below. The full list of change ideas suggested to address the gaps in care described in the above section are presented in box 6. Again, online supplemental table 2 provides a full list of the change ideas identified through the project.
Change ideas
Patient pathway
Creating a PD assessment with clear triage criteria
Development of an integrated specialist PD assessment, which is available at first point of contact with trained assessors and clear triaging criteria for different treatment options.
Upscaling evidence-based treatments and support delivered across the system
To broaden and upscale current treatment offerings, recruit, and train individuals to deliver a range of evidence-based treatment for PD (eg, Structured Clinical Management and Dialectical Behaviour Therapy).
Recruit specialists to offer a programme of group-based skills sessions, to patients in both primary and secondary care, for patients with a lower level of need or on waiting lists for further treatment.
Develop peer-support worker roles to best support the needs for patients with PD across the system.
Waiting list reduction initiative in the CNS and Psychological Therapies Service.
Create guidance on the correct prescribing of medication for patients with PD.
System-wide
Improving staff knowledge and support
Providing training to understand PD and how to care for patients with PD to staff across the entire system.
Prioritising protected supervision time for all staff caring for patients with PD which is mandatory and has clear expectations.
Creating an anti-burn-out plan/policy that reflects the demand of the work, destigmatises burnout and supports its recognition.
Provision of a tiered approach for support with complex cases (includes professional meetings and complex case panels) and protected time for staff to attend these, open to all services across the system, including outside agencies, for example, social work.
Improving the leadership of PD care
Create a system-wide leadership structure which provides an oversight of developments with PD care, supports risk taking and overall provides ownership of this patient groups care.
Enhancing governance over consistent and collaborative working across the system
Develop an accessible system to provide advice and guidance to services, using feedback and communication from relevant staff and lived experience workers. This will be a highly responsive system that ensures that there is supportive communication between services and the needs of this population are met.
Facilitate conversations between services to decide on shared language when referring to this patient group, to ensure greater consistency across services and increase appropriate and effective responses to patients’ needs.
Creating a PD assessment with clear triage criteria
We proposed to integrate a specialist assessment into the patient pathway, with trained assessors to address the lack of PD assessments early in the pathway. This would encourage a whole system view on the available options and more intelligence on where to refer patients depending on their level of need rather than the level of risk, with the overall aim of improving patients’ timely access to treatment. This approach is supported by some of the change ideas discussed below.
Upscaling evidence-based treatments and support delivered across the system
Multiple suggestions were given to improve the range of treatments available throughout the care pathway to ensure as many patients with varying levels of need receive support as possible. One idea was to upscale the delivery of evidence-based treatments in CMHTs, by recruiting and training individuals to deliver both Structured Clinical Management and Dialectical Behaviour Therapy. Another idea was to recruit specialists that could offer group-based skills sessions in primary and secondary care to reach patients with a lower level of need and as well as those on waiting lists for therapy. This approach would reduce wait times for those patients and reduce inappropriate referrals to the CNS and Psychological Therapies Service. Alongside this it was suggested that guidance should be produced that would aid appropriate prescribing of medication, to prevent overprescribing in this patient group.
Improving staff knowledge and support
To address the fact that staff lack knowledge and confidence around providing PD care it was suggested that all staff caring for patients should be provided with training to further understand PD and how to care effectively for this patient group. This would also provide a more consistent approach that could be adopted across services. An integrated clinical supervision structure would provide further support for all staff supporting patients with PD. It was also suggested that a tiered approach for support with complex cases is developed, which includes professional meetings and complex case panels and protected time for staff to attend these. These resources could also be made available to third sector organisations, for example, social work.
Improving the leadership of PD care
To address issues around PD care not being prioritised or owned by services, it was suggested that a leadership structure should be created that provides oversight, encouragement, and support for any developments in PD care happening across the system. This would support a better culture towards patients with PD and ensure clear messaging that the care of patients with PD is a core business of the Trust.
Discussion
Summary of what has been found
We sought to take a systematic mixed-methods approach to understand the care pathways for patients with PD across the OHFT system, assess the gaps in care and set out areas for improvement that OHFT could carry forward. Patients with PD, carers and staff recognised challenges concerning entering the system, which was supported by quantitative data, from unsupported wait times to reaching the right team to support the patient’s recovery journey. We set out a comprehensive approach to supporting patients with PD to address these challenges. These included ensuring a specialised approach to triage and assessment for patients with PD, delivered by upskilled staff with additional PD-focused support. Alongside this, a comprehensive approach to structuring support for staff such as system-wide supervision and understanding how to use a range of evidence-based practices to best support patients with PD. We recognised the importance of recovery-oriented practice and the opportunities for incorporating peer support workers to provide holistic support. Collectively, these approaches provide an opportunity to recognise how to support patients with PD in a helpful and supportive way.
Value of our process
We demonstrate some key learning points when undergoing a large-scale complex problem diagnosis to understand the whole system, identify gaps and propose areas for change. First, we used QI methodology to take a systematic approach, including appropriate stakeholder engagement and infrastructure for decision-making. Our focus was to ensure that the right people were involved to provide their expertise in co-designing what is needed to improve healthcare for patients with PD and the services they access. Throughout the process, we used relevant tools, such as process mapping to visually understand the relevant pathways and driver diagrams to display what is essentially our agreed theory of change. Finally, we used a mixed-method approach at all stages. The quantitative data provided an objective understanding of the patient pathway and informed discussions at each stage. To complement the data, we used qualitative approaches to fully use staff expertise in providing services and patients, carers and families to keep them at the centre of all the change ideas discussed.
Limitations and challenges
There are three limitations associated with this paper. First, we describe the experience of one NHS Trust and the infrastructures and pathways specific to its system, this may differ between mental healthcare organisations and contexts. Despite this limitation, there will likely be similar challenges across mental health organisations and our methodological approach is transferrable across mental health services. Indeed, we have provided sufficient detail for any relevant organisation to follow the steps provided. Second, our findings were limited somewhat by available data. In some instances, we could not provide data specific to patients with PD and were limited by the quality of the data collected. However, our mixed-method approach and consistent stakeholder engagement provided ample opportunities to understand our system fully, identify meaningful areas for improvement and suggest possible change ideas.
Third, the scope of this paper was to describe the methods used to assess the current provision of care for individuals with PD and give an orientation around areas of improvement that OHFT could carry forward. This means in this phase we did not consider the resources associated with change ideas and decisions around what changes to take forward and in what order, based on feasibility. Nor did we implement any of the change ideas outlined. In addition, due to this being the initial assessment phase some change ideas are broad so would take further thinking and analysis in future working groups, for example, around what evidence-based treatments could be delivered or what peer support roles would involve.
Next steps
Following the production of the list of gaps in care and potential change ideas, three workstreams were identified to carry this work forward:
A task and finish group to define what clinical and system changes would take place in the first year of implementation (April 2021–April 2022).
A working group to design new guidance for prescribing of medication for patients with PD.
A working group to address improving the culture around and language used in PD care.
Considerations for next steps in the first and third workstream could be around refining these areas of change towards evidence-based change ideas, deciding which should be taken forward and the order they should be addressed. Careful consideration should be taken here to ensure that additional resource is utilised in the most effective way to maximise patient safety, care and experience as well as staff well-being.
Refinement of change ideas could include quantifying what is possible with the given resource, for example, how many specialists would need to be recruited to deliver group-based skills sessions across the patient pathway and how many specialist assessments could take place each month. This would determine which areas of change are realistic and feasible with available resource. This process could also be informed by research and best practice to specify and enhance the clinical effectiveness of proposed change ideas.
Once refined and resource determined, it could then be considered which change ideas are cost neutral, save money, cost money or involve investing to save. This could then be used to inform a prioritisation matrix, to outline the order change ideas should be implemented. Prioritisation of ideas could also consider the balance between clinical effectiveness and clinical efficiency. Increasing patient flow through the system is important but not at the expense of clinical effectiveness or patient safety, so those ideas that strike the best balance could be prioritised.
There has been significant progress within the first workstream, as work has been taken forward by the Service Change and Delivery team to directly inform the implementation of a new PD pathway across Buckinghamshire services. Details associated with this work may form a future paper.
Conclusion
In recent years, mental health services and healthcare have focused on promoting QI to systematically approach large scale changes. National initiatives such as decreasing suicide and increasing various aspects of patient safety require trust-wide responses.25 Understanding how to tackle large-scale complex problems in healthcare requires complex approaches and complex solutions. To this extent, this paper provides a template and is translatable when carrying out an assessment of the system to try to understand complex pathways and deriving potential stakeholder informed areas for future improvement. We hope that sharing our methods will help mental health services take the first step in approaching system-wide improvement work.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to mention and thank all stakeholders that contributed to the project. This includes patients, carers and staff involved in the focus groups, as well as members of the steering group. We appreciate and value the ongoing time and commitment you dedicated to this project.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MM was a member of the project team, involved in various project activities and drafted the manuscript. DFH contributed to the development of the manuscript format and assisted with drafting the manuscript. HT was a member of the project team, involved in various project activities and reviewed and refined the manuscript. CV advised on the manuscript development and assisted with drafting parts of the manuscript. DM was the project lead and reviewed and refined the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.