Article Text

Abstract
A patient impact project which successfully reduced the transient ischaemic attack (TIA) clinic waiting time from 9 to 3 days in an acute Welsh hospital, revealing the challenges faced and how alternative thinking and team work improved care given to our service users. Evaluating current situation, careful planning with multiple brainstorming meetings, 4 N chart and driver diagram with change ideas laid the foundation for this service improvement. Run charts, statistical process control and Pareto charts helped to identify the issues that are hindering the progress, which when rectified, reduced the clinic waiting times. Avoiding clinic cancellations by cross covering TIA clinics with mutual agreement among consultants and redeployment of ward staff to support clinics resulted in a positive impact to the patients. The average waiting time to see a patient in TIA clinic dropped from 9 days to just 3 days as a result of this, reflecting the hard-working and proactive nature of a team following a collaborative leadership journey. The service improvement initiative for ‘avoiding clinic cancellations’ was implemented in January 2017 and has reduced our waiting times by three times. Repeat analysis by six monthly Plan Do Study Act cycles revealed that this improvement is sustained.
- teamwork
- quality improvement methodologies
- patient-centred care
- healthcare quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Our stroke department is one of the busiest units in Wales with a major emergency department serving a population of more than half a million in South West Wales. All suspected acute strokes present to our emergency department, and if the symptoms are transient, patients are discharged on a transient ischaemic attack (TIA) pathway to be assessed in a rapid access TIA clinic. This avoids hospital admission and ensures early specialist review.
Rapid access TIA clinics were established locally in 2013, in one of the assessment rooms in medical admissions unit. These clinics run Monday to Friday, with an average of 20 new referrals every week. The clinic was struggling to meet the requirement of a timely assessment (less than 7 days). The average waiting time for a clinic appointment in 2016 was 9 days with many patients waiting up to 23 days and the organisation failed in its performance target. This resulted in an urgent need to change the current system thereby meeting Kotter’s first principle1for an organisational change.
Stroke is one of the leading causes of mortality and disability nationally, affecting an estimated 7400 people every year in Wales alone.2 TIA is referred as ‘mini stroke’ in layperson’s terminology and it is a warning symptom for an acute stroke. Since TIA causes only transient symptoms, people usually ignore these as ‘funny turns’, which is a great danger as one in 12 TIA sufferers will have an acute stroke within a week.2 The timely and appropriate treatment of a TIA will reduce the incidence of a disabling consequence. The EXPRESS (Early use of eXisting PREventative Strategies in Stroke) trial phase 2 results have revealed that early assessment of a TIA will reduce the risk of a stroke from 10% to 2%.3
The National Institute for Health and Care Excellence guidelines recommend that all TIA sufferers should be seen in specialist clinics as soon as possible and certainly within 7 days.4 Most Welsh hospitals do not have a 7-day TIA clinic, and hence realistically, we are aiming to see all referrals in less than 7 days.
Evaluation of the current TIA database and team brainstorming sessions have identified a variety of factors contributing to the performance failure. Increasing referrals without increase in resources, lack of clinic support staff or dedicated clinic space, clinic cancellations during physician’s on call duties or leaves and unnecessary steps in TIA referral pathway that are prone to delays were few of the issues identified.
Aim
To improve the efficiency of a rapid access TIA clinic assessed by reduction in waiting times to less than 7 days by implementing the service improvement change idea from January 2017.
Methods
Multiple brainstorming meetings with team members including consultant colleagues, stroke specialist nurses, secretaries, administration staff, radiology and vascular colleagues identified many factors that were influencing our performance failure. Increasing demand from the baseline year of 2013 is revealed in figure 1.
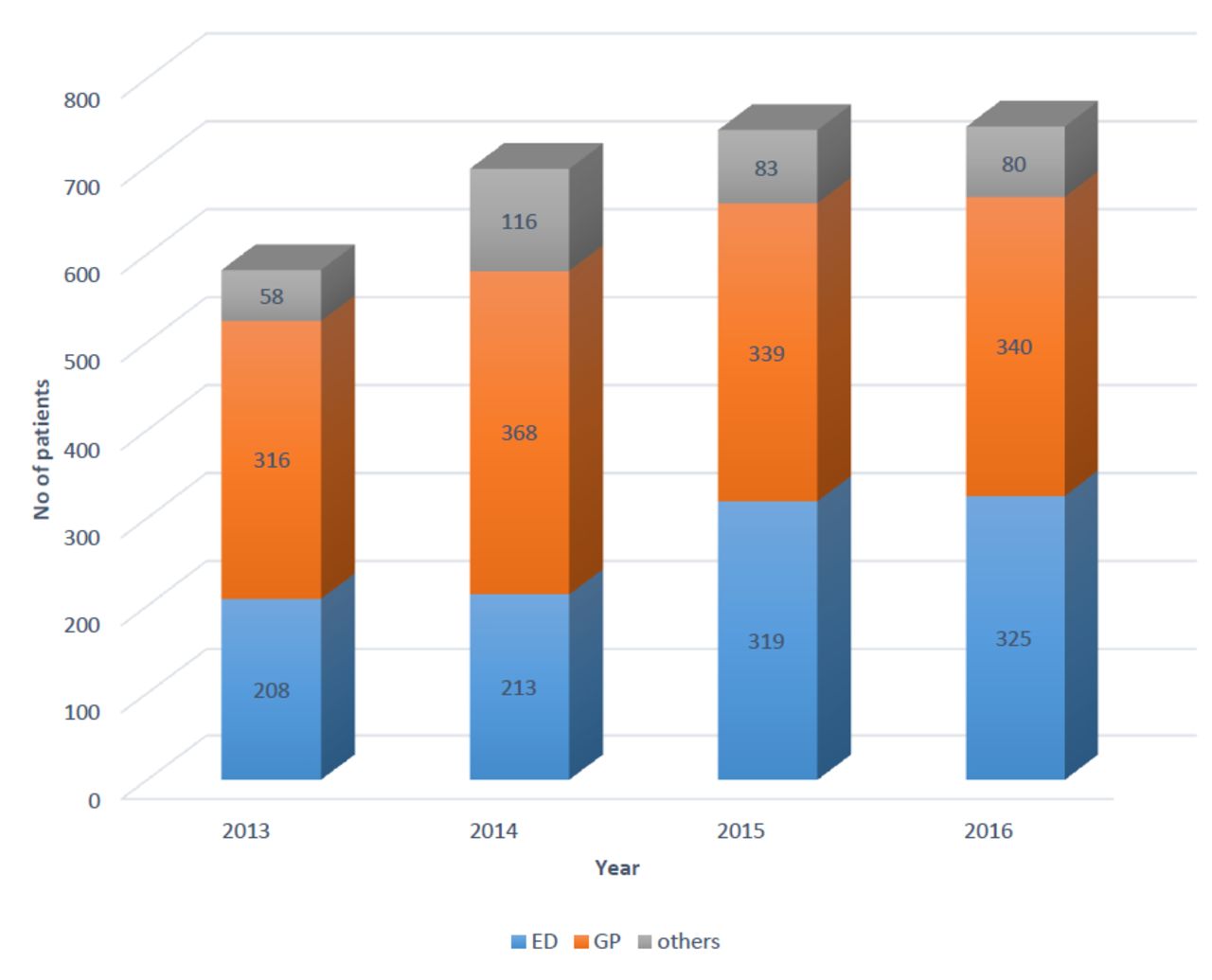
Axis: source of referrals; Y axis: number of patients, figure 1 reveals the volume and source of all referrals to transient ischaemic attack clinic from 2013 to 2016 (separated as ED (emergency department), GP (general practice) or ‘others’ including eye clinics or medical wards).
A TIA mimic is the term used for any condition that resembles or presents as a TIA to the initial assessor but not diagnosed as a TIA. This could include a variety of presentations, some of the common ones being postural hypotension, syncope, seizures, which could follow an alternative referral pathway. With the increase in number of referrals to the services, the percentage of mimics had also increased from 44.5% in 2013 to 60% in 2016, which meant that the patients with TIA were waiting longer to be assessed in clinic.
We looked at statistical process control (SPC) of number of referrals from emergency department against time from January 2013 to November 2016. This SPC chart revealed the increased number of referrals between 2013 and 2014, with a special cause flag (online supplementary figure 1). This could be because of increased awareness of stroke and TIAs, thereby referring any condition similar to or mimicking a TIA to the TIA pathway.
Supplementary file 1
Intervention
The project had many challenges with multiple stakeholder involvement. Analysing the existing TIA clinic database revealed the referral volume since 2013 progressively increased to a point in 2016 where services were collapsing. From January 2017, the team decided to put systems in place to improve clinic waiting time to less than 7 days. Brainstorming meetings with the wider team helped to develop a driver diagram with ideas for change ranging from increasing clinic slots, avoiding cancellations, dedicated clinic space, increase in supporting staff and appropriate use of specialist time in line with prudent healthcare principles.5
Stroke clinical nurse specialists were undertaking blood pressures and cardiac tracing in the clinic. During the intervention, band 3 healthcare support workers were trained to do these assessments, so specialist nurses can provide support to emergency department and stroke ward where their expertise was better used.
High engagement within the team was maintained at all times. This helped the team to create ideas that did not require additional resources. Team engagement resulted in each team member taking ownership of the ideas for change, which diminished resistance to change and we were able to see positive results.
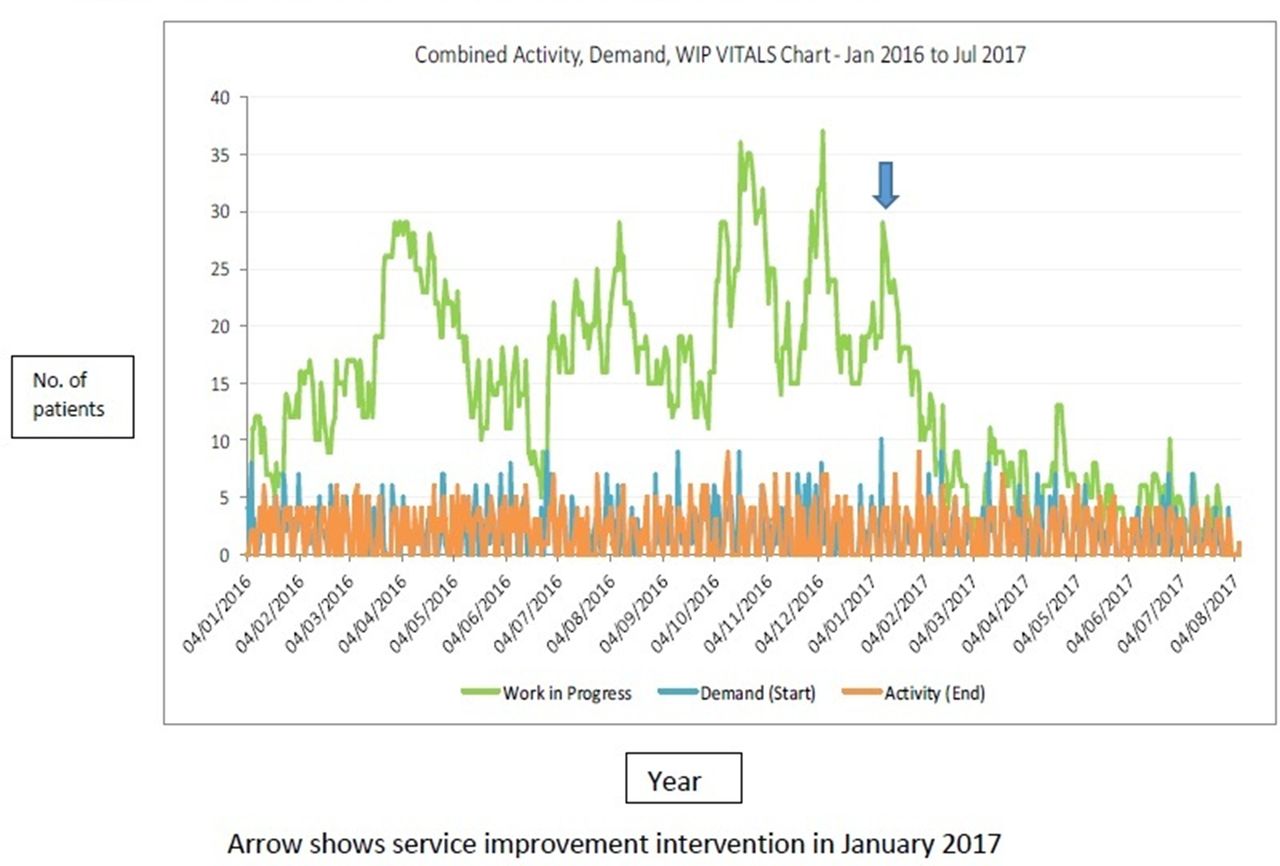
Figure 2 is a vitals chart revealing the relationship between clinic demand, activity and work in progress. This demonstrates that every time the clinic activity went down, the work in progress (number of patients waiting for an appointment) was going up. This was having adverse effect on clinic waiting times. There were multiple reasons for clinic activity to drop, key one being consultant leave and on-call duties.
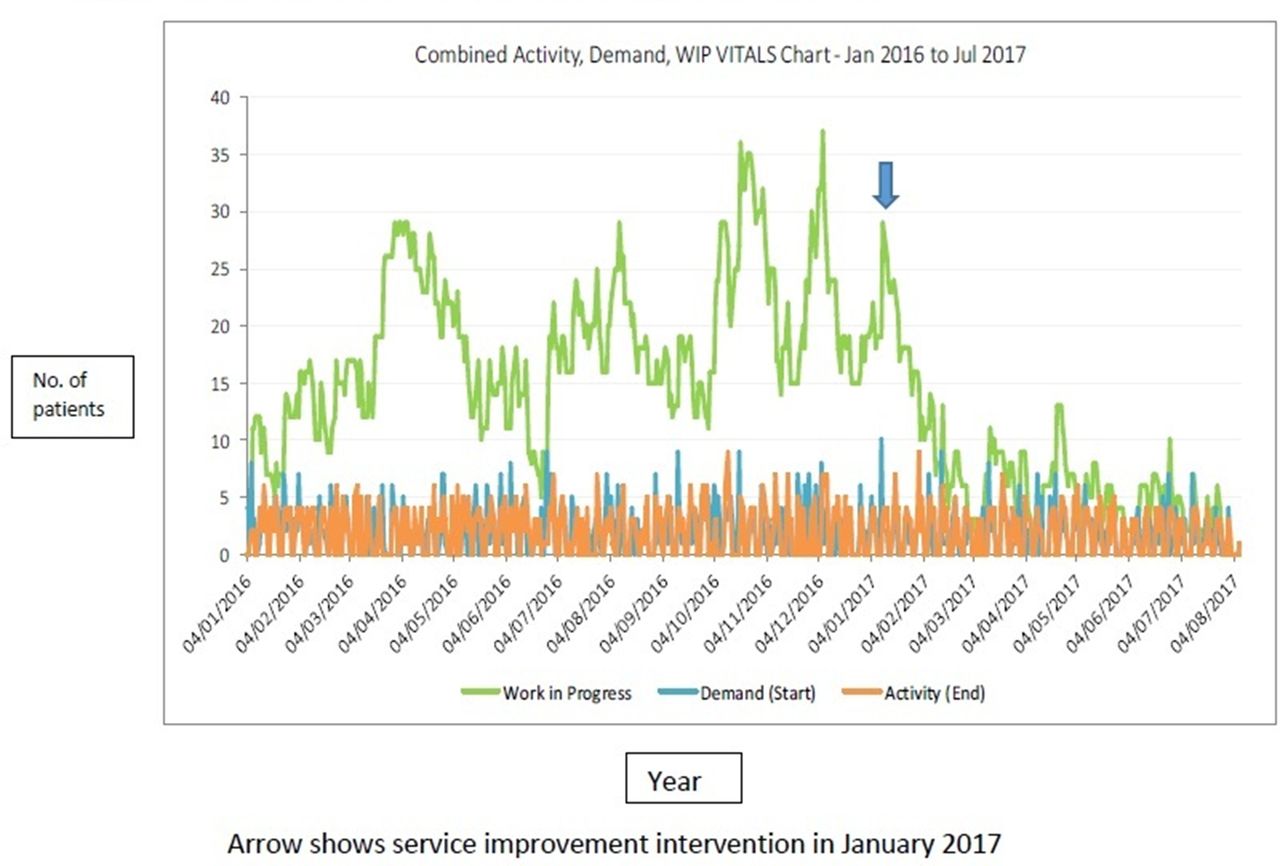
X axis—year, Y axis—number of patients. Vitals chart revealing the demand, activity and work in progress (WIP) of transient ischaemic attack clinic before and after the service improvement intervention in January 2017.
The team had multiple meetings and jointly decided to cross cover another consultant’s TIA clinics by making their supporting professional activity sessions flexible so that this can be taken at a time when all colleagues are around. Nursing support for the TIA clinic was resourced from band 3 healthcare staff on the acute stroke ward.
Results
In 2016, the average waiting time (figure 3) was 9 days with an upper control limit of 23 days, and some patients were waiting much longer, up to 90 days (red diamonds for outliers on chart). This is the year when our organisation failed in its TIA clinic waiting time target. The service improvement intervention (avoidance of clinic cancellation by consultant cross cover, with support provided by trained healthcare assistants from ward F, re-deploying specialists nurses to attend acutely unwell patients), was implemented in January 2017.

{kind=link}
![[bmjoq-2017-000237-SP1.jpg]](https://bmjopenquality.bmj.com/content/bmjqir/7/4/e000237/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
{kind=link}
{kind=link}
Statistical process control chart of improvement in transient ischaemic attack clinic waiting times since January 2017.
The average waiting time to see a patient in TIA clinic dropped from 9 days to just 3 days with all patients seen in less than 7 days (figure 3). The Plan Do Study Act cycle was repeated every 6 months, the last cycle in February 2018, when the average waiting time was 2.5 days with all patients seen in less than 7 days, confirming that the service improvement is sustained.
Ethical consideration
The stroke sentinel national audit programme from the Royal College of Physicians is a national audit that every health board in Wales has signed up to perform and report widely and this incorporates the TIA services. The local TIA database is stored on health board’s shared folder and permits access only to those personnel directly involved in providing TIA services. The project was registered locally with the audit department.
Limitations
Although the service improvement project has achieved its primary aim, we were keen to achieve an improvement in the number of inappropriate referrals or TIA mimics to the services. The TIA mimic referrals to the service have been around 60%, which has not improved. Regular education of junior doctors is undertaken by the team to continue the improvement work. Analysing the alternative diagnosis from TIA clinic helped us to plan appropriate referral pathways for TIA mimics, thereby tightening our pathway to ensure that the limited resources are used appropriately.
There are other factors in this journey that we would like to improve including one stop TIA clinics, TIA administration support, electronic referrals, which the team are working towards achieving. Our patient feedback has revealed 100% satisfaction with the current TIA services.
Conclusion
Teamwork and alternative thinking has helped us to reduce the TIA clinic waiting times by threefold, now that TIA sufferers are seeing a specialist three times faster in our locality. Overall, this patient impact project was a positive learning process, improving our team building and leadership skills. We have been able to use the quality improvement techniques learnt in the improving quality together6 training sessions effectively to deliver this project. The learning and practical experience gained from the project will be a valuable component of any service improvement project that we undertake in the future.
Acknowledgments
Special acknowledgements to our Radiology and Vascular colleagues for their support in seeing patients quickly; also our TIA secretaries and administration staff for maintaining the TIA database and obtaining patient feedback. Special thanks to Jayne Coady for encouraging the band 3 role and to Nicola Williams and Helenna Jarvis-Jones for supporting this initiative. Our gratitude to Wendy Rees, Gareth Barbour, David West and Jonathan Baglow from medicine service group for their support in organising team meetings, analysing the data and contribution throughout the project including acquiring a new clinic space.
Footnotes
Contributors MK: planned and led the project. AJ: assessed database and helped with charts. TA, SC, PMES: contributed in brainstorming meetings and implementation of change ideas. KW: managed the stroke clinical nurse specialist role in clinic. SY: envisioned the extended band 3 role in clinic and provided training for the same.
Funding The Quality Improvement project was undertaken as part of medical leadership programme organised by AcademiWales, which aims to harness the talents of leaders in public services across Wales. ABMU health board fully sponsored the leadership learnings. The service improvement project did not need any additional funding, but we were able to acquire a new clinic space once the project was successful. This required a small funding to refurbish the clinic area, giving us the opportunity to increase our clinic activity to match the demand.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.