Article Text

Abstract
Objective To identify the risk factors and characteristics of central serous chorioretinopathy (CSC) with subsequent macular neovascularisation (MNV) detected on optical coherence tomography angiography (OCTA).
Methods and analysis We included patients from six institutions who were initially diagnosed with CSC and subsequently did or did not develop MNV detected by OCTA. Potential influencing factors were identified by evaluating the patients’ baseline demographics, multimodal fundus imaging, treatment options, recurrence and outcomes in both groups.
Results We enrolled 176 eyes in 152 patients (112 men, 40 women; mean age: 52.1±10.4 years) with a mean follow-up of 30.4±16.3 months. Secondary MNV was present in 23 eyes (13.1%), and non-MNV was observed in 153 eyes (86.9%) by OCTA. Multivariate analysis revealed that older age (OR 1.06; 95% CI 1.01 to 1.11; p=0.014), chronic CSC (OR 3.05; 95% CI 1.12 to 8.30; p=0.029), leakage sites within the fovea on fluorescein angiography (OR 7.60; 95% CI, 1.89 to 30.48; p=0.004) and recurrent fluid within the first year (OR 5.12; 95% CI 1.66 to 15.77; p=0.012) were risk factors for subsequent MNV. Moreover, eyes with CSC complicated with MNV were characterised by poor visual acuity and low complete fluid resolution rates.
Conclusion The factors associated with MNV secondary to CSC were older age, higher rates of chronic CSC and recurrence, and foveal leakage points on fluorescein angiography.
- choroid
- macula
- neovascularisation
- retina
Data availability statement
Data are available on reasonable request. Datasets for this study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
The risk factors for central serous chorioretinopathy (CSC) have been widely studied, but the risk factors for CSC with secondary macular neovascularisation (MNV) are not well understood. Few studies have investigated the clinical manifestations of subsequent MNV in CSC and its influence on prognosis.
What this study adds
Recurrence within the first year and foveal leakage points on fluorescein angiography are risk factors for the formation of MNV in CSC. Moreover, CSC patients with secondary MNV have poorer vision and low complete resolution rates.
How this study might affect research, practice or policy
The identification of multiple risk factors may assist in early detection or intensive treatment for patients with CSC at high risk of MNV and avoid poor prognosis.
Introduction
Central serous chorioretinopathy (CSC) typically manifests as serous detachment of the neurosensory retina, often below the macula, resulting from a retinal pigment epithelium (RPE) barrier disorder and pachychoroid owing to hyperpermeable vessels.1 Chronic CSC or recurrent CSC frequently results in severe irreversible vision damage caused by photoreceptor impairment and RPE atrophy.1 2 Choroidal neovascularisation refers to abnormalities of blood vessels derived from choroidal capillaries, which penetrate through a break in Bruch’s membrane (BM) and proliferate into the space between the BM and the RPE or neurosensory retina.3 4 A panel of experts recently recommended a new definition of macular neovascularisation (MNV) to replace the old term of choroidal neovascularisation.5 In recent research, CSC has been considered a part of the pachychoroid spectrum disease and may be complicated by the secondary formation of exudative MNV6 7; however, the mechanism of secondary MNV has not yet been determined. Some studies have found an increased prevalence of MNV after treatment with laser8 9 or photodynamic therapy (PDT)9 10 in CSC, which may be caused by rupture of the BM after laser therapy or choroidal ischaemia and excessive vascular endothelial growth factor (VEGF) production after PDT.9
The emergence of optical coherence tomography angiography (OCTA), an innovative imaging technique that does not require a fluorescent dye, facilitates the visualisation of three-dimensional images of the retina and choroidal microcirculation.3 By comparing static tissue and locomotive blood cells, a split-spectrum amplitude-decorrelation angiography algorithm is implemented to improve the detection ability of blood flow signals and abnormal neovascularisation.3 11 Furthermore, the specificity and sensitivity of OCTA for detecting MNV are comparable with values obtained using invasive fluorescein angiography (FA).11
Although the risk factors for CSC have been widely described, limited research regarding the risk factors for CSC with secondary MNV has been performed, and few studies have investigated the influence of MNV on recurrence and clinical manifestations. Therefore, using OCTA technology in a multicentre study, we comprehensively evaluated the potential risk factors and clinical characteristics of subsequent MNV in CSC and explored its influence on prognosis.
Materials and methods
Patients
We conducted a retrospective multicentre study that recruited CSC patients at the following six institutions from June 2013 to September 2020 (Japan Clinical Retina Study group): Hyogo College of Medicine, Kagoshima University, Kobe University, Nagoya City University Graduate School of Medical Sciences, Nara Medical University and Sapporo City General Hospital.
The diagnosis of CSC was mainly according to the presence of typical manifestations in multimodal imaging on OCT, FA and indocyanine green angiography (ICGA) as follows: (1) subretinal fluid (SRF) involving the macula, RPE changes, thickened subfoveal choroid on OCT; (2) single or multifocal leakage points on FA and ICGA; and (3) with or without choroidal vascular hyperfluorescence during the late phase of ICGA.12 Acute CSC was defined as the presence of visual symptoms within 6 months and with one or a few focal leakage points from the RPE, whereas chronic CSC was defined as having visual symptoms lasting for more than 6 months. We included eyes diagnosed as CSC with SRF that were followed up for at least 12 months without evidence of MNV confirmed by baseline OCTA. Eyes with intraretinal and subretinal haemorrhage or irregular RPE elevation indicative of MNV or polypoidal choroidal vasculopathy; a history of any retinal surgeries (except for PDT, focal laser or intraocular injection for treating CSC; cataract surgery) or other retinal and choroidal diseases, such as age-related macular degeneration, tilted disc, uveitis, angioid streaks, pathological myopia and diabetic retinopathy; and incomplete imaging information for important parameters were excluded. The acquisition and analysis of clinical data were implemented without the requirement for written informed consent because of the retrospective and observational nature of the study. Some patient data in this study partially overlapped with our previous research.13
Ophthalmic examination
A comprehensive retinal imaging evaluation consisting of FA, ICGA (HRA2; Heidelberg Engineering, Heidelberg, Germany), OCT (Spectralis HRA-OCT; Heidelberg Engineering), and OCTA was performed. The OCTA images were captured using a DRI-OCT Triton device (Topcon, Tokyo, Japan), Spectralis OCT 2 (Heidelberg Engineering), or AngioPlex (Carl Zeiss Meditec, Dublin, California, USA) to scan a foveal area of 4.5×4.5 mm or 6×6 mm. An artefact removal option was used for this study. Three-dimensional angiographic images were obtained after the instrument was aligned with the macula, and then the four vascular slabs, including the superficial retina, deep retina, outer retina and choriocapillaris, were segmented automatically. Sequentially, MNV was confirmed as evidence of abnormal signals consistent with the pathological vascular component at the level of the outer retinal slab or choriocapillaris slab.
Treatment and follow-up
Treatment was performed according to each doctor’s discretion. Treatment with PDT was mainly indicated when the eye had persistent SRF over 3 months with subfoveal or parafoveal leakage point or diffuse RPE leakage. Focal laser photocoagulation was performed in eyes with focal extrafoveal leakage. The initial treatment options, including PDT (PDT alone or PDT combined with anti-VEGF/focal laser), focal laser photocoagulation and intravitreal anti-VEGF injection monotherapy, recurrence status since the first fluid resolution in our institutes, and outcomes, such as final best-corrected visual acuity (BCVA) and OCT findings, were recorded. During the follow-up, the presence or absence of MNV was determined by OCTA.
Eyes that were initially diagnosed as CSC and developed secondary MNV comprised the subsequent MNV group. Eyes with CSC that did not develop MNV comprised the non-MNV group. A comparison of the clinical parameters and imaging data between the two groups was performed to identify the factors associated with developing MNV.
The following medical record data were collected from every subject: age, sex, history of systemic steroid use, smoking status, follow-up duration, bilaterality of disease, acute or chronic course, spherical equivalent, BCVA at baseline and final visit, and treatment. In addition, the following imaging parameters were analysed: central retinal thickness, subfoveal choroidal thickness on OCT, leakage sites (within or outside the fovea), the number of leakage points (single or multiple), intensity of fluorescein leakage (intense or non-intense) on FA, and choroidal vascular hyperpermeability (CVH) on ICGA at baseline.
Statistical analysis
Analyses were performed with JMP Pro (V.14.0.0; SAS Institute). For continuous variables, the mean and SD were calculated. For discrete variables, the frequencies and percentages in each category were calculated. Group differences were assessed using the Mann-Whitney U test for continuous variables and Fisher’s exact test or Pearson’s χ2 test for categorical variables. Independent variables with a p<0.05 and near-significance were used in the multivariate logistic analysis. Statistical significance was determined when the p value was <0.05. To facilitate statistical analysis, BCVA was converted to the logarithm of the minimum angle of resolution (logMAR). The Bonferroni correction was used to adjust for multiple comparisons.
Patient and public involvement
Patients or the public were not involved in our research.
Results
Clinical characteristics
A total of 176 eyes in 152 patients (112 men, 40 women) with a mean age of 52.1±10.4 years (range 31–82 years) were included in this study. Thirty-five patients had received systemic steroids (23.0%). Seventy patients (46.1%) had a history of smoking, and no records were available for this parameter for 20 patients. Fifty-two patients were diagnosed with bilateral CSC (34.2%). Among the entire cohort, 109 eyes (61.9%) were diagnosed as acute CSC and 67 eyes (38.1%) as chronic CSC. During a mean follow-up of 30.4±16.3 months (range 12–87 months), 73 eyes (41.5%) experienced at least one episode of recurrent SRF, and 23 of 176 eyes (13.1%) were confirmed as MNV and categorised as the subsequent MNV group.
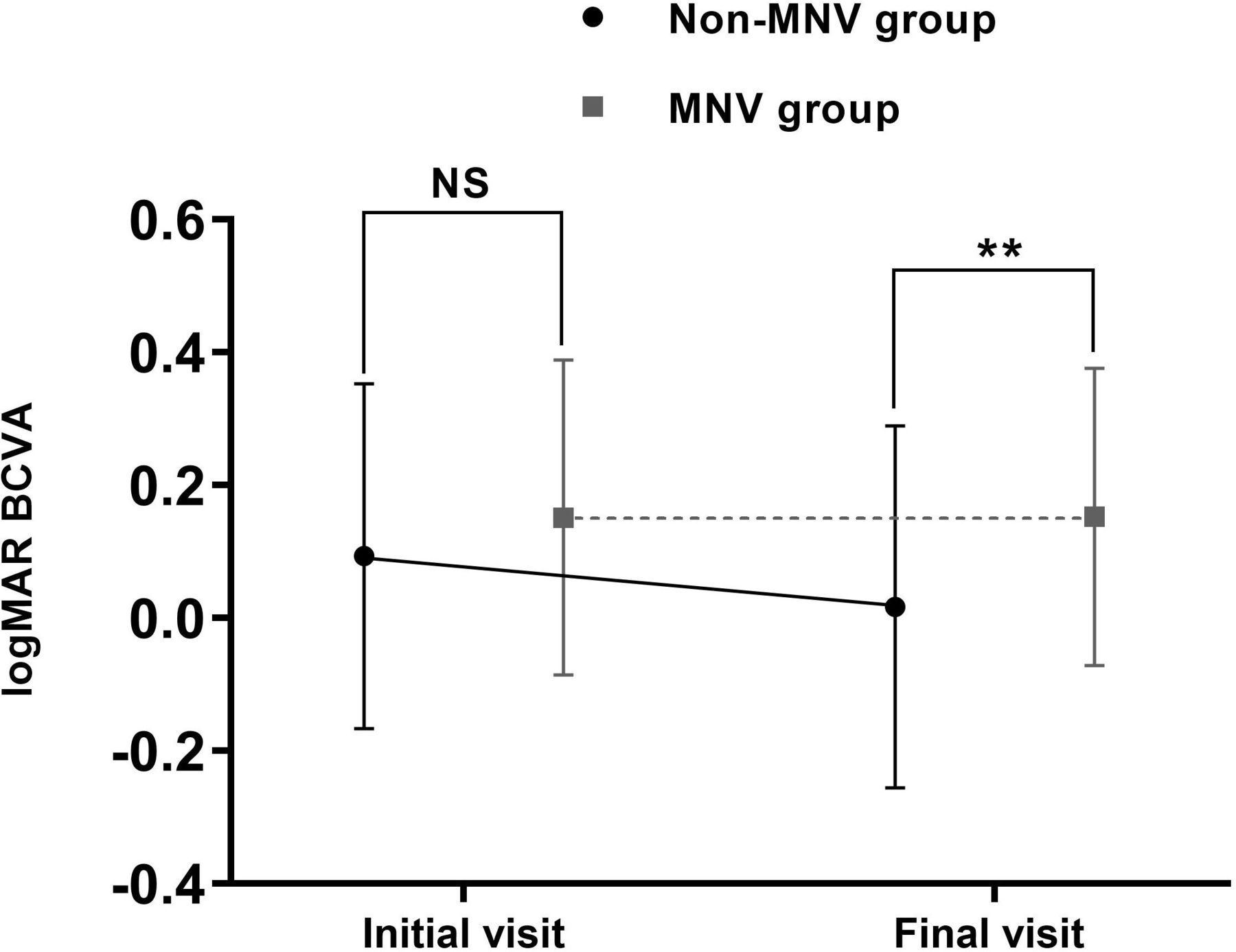
The baseline clinical characteristics and imaging manifestations of the patients in the two groups are demonstrated in table 1. Patients in the subsequent MNV group tended to be older (mean age: 57.2±10.7 years; range 38–81 years) than the patients in the non-MNV group (mean age: 51.3±10.2 years; range 31–82 years; p=0.015). Chronic CSC was observed in 13 of the 23 eyes (56.5%) in the subsequent MNV group and 54 of the 153 eyes (35.3%) in the non-MNV group (p=0.051). The mean baseline BCVA in the non-MNV group was 0.09±0.26 logMAR (range −0.18–1.40) compared with that of the subsequent MNV group with a logMAR of 0.15±0.24 (range −0.18 to 0.82; p=0.120; figure 1). There were no statistically significant differences in sex, systemic steroid use, smoking history, bilateral involvement and spherical equivalent between the two groups.
Comparison of the clinical parameters and imaging findings between the non-MNV group and subsequent MNV group

{kind=link}
The logarithm of the minimum angle of resolution (logMAR) best-corrected visual acuity (BCVA) at the initial and final visits in central serous chorioretinopathy eyes with and without macular neovascularisation (MNV). The mean logMAR BCVA at the final visit was significantly worse for eyes with MNV (**p<0.001). Error bars represent the SD. NS, not significant.
Regarding the respective imaging results, no significant differences were found in central retinal thickness and choroidal thickness measured on OCT at baseline between the two groups (339.4±107.4 µm and 383.3±113.5 µm, respectively, in the subsequent MNV group and 362.3±138.1 µm (p=0.440) and 381.3±108.5 µm (p=0.870), respectively, in the non-MNV group). Regarding the FA findings at baseline, five eyes (21.7%) that developed leakage within the fovea in the subsequent MNV group were compared with ten eyes (6.5%) in the non-MNV group (p=0.015). However, the distribution of multiple leakage points (p=0.899) and the intensity of fluorescein leakage (p=0.194) between the two groups were not significantly different. Furthermore, areas of choroidal vascular permeability were detected in 19 eyes (82.6%) of patients with subsequent MNV and 123 eyes (80.4%) of patients without MNV (p=0.360).
Treatment regimens
The proportions and differences in treatment regimens between the two groups are summarised in table 2. In the non-MNV group, 89 eyes received PDT (58.2%), of which 10 eyes (6.5%) received PDT combined with focal laser treatment, two eyes (1.3%) received PDT combined with anti-VEGF therapy; 38 eyes (24.8%) received focal laser treatment alone, 2 eyes (1.3%) were treated with anti-VEGF therapy alone, and 24 eyes (15.7%) underwent observation. In the subsequent MNV group, PDT was performed in 15 eyes (65.2%), of which PDT was combined with focal laser treatment in 4 eyes (17.4%) and anti-VEGF therapy in 1 eye (4.3%); focal laser treatment alone was performed in 2 eyes (8.7%), anti-VEGF therapy alone was performed in 1 eye, and observation was performed in 5 eyes (21.7%). There were no significant differences in treatment options between the two groups (p=0.163).
Differences in treatment regimens and outcomes between the non-MNV group and subsequent MNV group
Recurrent macular fluid and outcomes
As shown in table 2, the mean follow-up time was 30.0±16.2 months (range 13–72 months) in the non-MNV group and 32.8±17.5 months (range 12–87 months) in the MNV group (p=0.602). Recurrent SRF was detected in 73 of 176 cases (41.5%) for the entire cohort, with 14 (60.9%) in the MNV group and 59 (38.6%) in the non-MNV group (p=0.043). Among these cases, nine eyes showed recurrence within the first year (39.1%) in the MNV group compared with 30 eyes (19.6%) in the non-MNV group (Bonferroni corrected p=0.104).
The mean number of recurrent SRF episodes was not significantly different between the two groups: 1.5±0.5 in the MNV group and 1.3±0.6 in the non-MNV group (p=0.364). Moreover, the average time to first recurrence (p=0.301), BCVA (p=0.311), central retinal thickness (p=0.945), choroidal thickness (p=0.838), leakage sites (p=0.303), numbers of leakage points on FA (p=0.419), and distribution of CVH on ICGA (p=0.581) at the initial recurrence did not differ significantly between the groups.
Overall, the final BCVA was significantly worse in the subsequent MNV group (0.15±0.22 logMAR; range −0.18 to 2.00; p<0.001; figure 1). Additionally, the final OCT results showed that the rate of incomplete fluid resolution (17 eyes; 73.9%) in the MNV group was significantly higher than that in the non-MNV group (48 eyes; 31.4%) (p<0.001). The specific distributions of the OCT manifestations are shown in table 2.
In the multivariate analysis, older age (OR, 1.06; 95% CI 1.01 to 1.11; p=0.014), chronic CSC (OR 3.05; 95% CI 1.12 to 8.30; p=0.029), leakage sites involving the fovea on FA (OR 7.60; 95% CI 1.89 to 30.48; p=0.004) and recurrent SRF within the first year (OR 5.12; 95% CI 1.66 to 15.77; p=0.012) were independently associated with subsequent MNV (table 3).
Risk factors associated with the development of macular neovascularisation in patients with CSC in the multivariate logistic analysis
Discussion
Although FA and ICGA remain the primary methods to detect MNV,1 OCTA may be used instead of conventional angiography as a noninvasive and rapid technique.14 OCTA has enabled the detection of concurrent type 1 MNV in eyes with CSC at a higher rate than expected, and the corresponding OCTA B-scans simultaneously provide valuable information for identifying the depth and thickness of MNV and accompanying fluid.3 15 In this study, cases presenting with MNV or polypoidal choroidal vasculopathy at the first visit were excluded by OCTA, and the incidence of subsequent MNV was 13.1%, which is within the range of 2%–24% reported in previous studies.16–19 Our study found that older age, chronic CSC, recurrent SRF episodes within the first year or leakage within the fovea on FA were associated with secondary MNV. Worse visual acuity and incomplete fluid regression were more prominent in CSC patients with subsequent MNV.
A recent single-centre study analysed the OCT risk factors for macular complications in eyes with ‘resolved’ chronic CSC and revealed that intraretinal hyperreflective foci, inner choroidal attenuation and presence of macular complications in the fellow eye are associated with an increased risk of MNV development.20 Our multicentre study focused on the active episode of CSC using multimodal imaging, which may be conducive to the timely diagnosis, treatment and management of patients in the active stage.
Our findings are consistent with other studies showing that patients in the subsequent MNV group were older than those in the non-MNV group.10 18 21 Flat RPE elevation, which suggests MNV, was observed frequently in patients with CSC aged 50–70 years.22 Dansingani et al reported that senility and fragility of the BM and RPE in older patients might cause susceptibility to subsequent neovascularisation.23 In this study, we found no obvious gender predominance in the prevalence of MNV, with incidence rates of 13.4% in men and 15.0% in women, as confirmed in a previous report.24 However, this result was in contrast to another study reporting that the incidence of MNV was higher in women with CSC.25 Hence, further research is warranted to address this discrepancy.
Chronic CSC predisposes patients to the emergence of MNV.19 26 Our study showed that 56.5% of eyes in the MNV group had chronic CSC, and the rate was higher than that in the non-MNV group. Fung et al reported that the development of MNV is more common in older patients with long-term CSC.27 The theoretical mechanism is a defect in the BM caused by chronic RPE changes and detachment that stimulates the proliferation of endothelial cells from the sub-RPE area.28 Remarkably, acute CSC cases accounted for 43.5% of the cases in the MNV group, suggesting that we should not neglect the possibility of neovascularisation in acute CSC.
Leakage points within the fovea were associated with secondary MNV, and to our knowledge, this interesting association has not been confirmed previously. The proportion of patients with leakage points starting from the fovea was only 6.5% in the non-MNV group compared with 21.7% in the MNV group. A previous study discovered that most leakage points were located 0.5 mm from the central fovea and the upper nasal quadrant in CSC, and the authors suggested that such a disturbance potentially stemmed from abnormal structures in the superjacent retina or the subjacent choroid.29 It is well known that a leakage point typically indicates a defect in the underlying RPE,30 31 and changes in the RPE were confined to the areas of CVH and thickened choroid by ICGA and OCT.32 Lee et al identified that the majority of MNV lesions were located in the subfoveal and juxtafoveal regions.24 Consequently, it is speculated that foveal leakage points may be a potential predictor of MNV.
CVH, choroidal vasodilation and increased choroidal thickness are representative characteristics of pachychoroid spectrum diseases.33 In this study, neither choroidal thickness nor the presence of CVH at baseline differed significantly between the MNV and non-MNV groups. The lack of association with CVH was consistent with the findings of Lee et al24; however, another report25 showed that CVH was detected more frequently in the MNV group while choroidal thickness was not significantly different in CSC with and without MNV. Matsumoto et al reported thinner choroidal thickness in PNV compared with that in CSC.34 Considering these results, it appears to be difficult to predict subsequent MNV using baseline choroidal thickness and CVH.
Full or half-fluence PDT has proven pivotal in the treatment of CSC.35 In this study, the majority of patients were referred from primary clinics to our major hospitals due to their visual complaints, which might explain the relatively higher rate and earlier timing of PDT. However, PDT might cause choroidal ischaemia and induce subsequent MNV.9 The initial treatments in the two groups in this study were not substantially different, and a risk of PDT was not confirmed. We found a high recurrence rate of CSC associated with MNV of 60.9%. Yeo et al hypothesised that choroidal ischaemia resulting from recurrent episodes of CSC could induce the development of secondary MNV.21 In the study by Fung et al, the mean time between CSC diagnosis and MNV detection was 139 months.27 Because it was difficult to confirm a cause–effect relationship between SRF recurrence and MNV development, we considered recurrence within the first year as a potential factor suggesting earlier development of MNV. Taken together, it is possible that the recurrent SRF accumulation and chronic course cooperatively led to the attenuation of the inner choroid and choriocapillaris, causing an ischaemic microenvironment that promoted VEGF release and consequent neovascularisation.21 23 In addition, the senility and fragility of the BM-RPE complex in older patients allow choroidal vessels to penetrate the sub-RPE space.23
Few studies have explored the recurrence characteristics of CSC in relation to MNV. In the subsequent MNV group, Final BCVA was significantly worse, and the rate of incomplete fluid resolution was significantly higher compared with those in the non-MNV group in the current study. A recent report showed that the anti-VEGF response was highly variable and often incomplete for secondary MNV in CSC.36 However, the results suggested that earlier detection of MNV and prior anti-VEGF treatment would result in better treatment responses. Of note, the proper diagnosis of MNV in pachychoroid eyes may be challenging using ICGA because of the hyperfluorescent presence of late washout compared with late plaque hyperfluorescence in age-related macular disease associated with MNV, whereas OCTA provides a useful diagnostic method for the identification of neovascular networks and flat irregular pigment epithelial detachment in pachychoroid eyes.37 38 Consequently, early identification of MNV using OCTA and prompt therapy are recommended to prevent a poor prognosis.
There were several limitations to the current study. Given the inadequacy of retrospective studies, short follow-up period, comparatively limited cases of neovascular CSC and lack of a standard methodology for reviewing the entire course of each participant in this study, our findings may lack generalisability. Because the exact time of MNV occurrence was unknown, we chose multivariate logistic regression analysis rather than a multivariate Cox regression model to estimate risk factors in the MNV group. Prospective and bias-free investigations are warranted to evaluate the characteristics and prognosis of patients with CSC under the influence of MNV.
In conclusion, our multicentre clinical research provided essential insight into the risk factors for MNV development, including older age, chronic course, SRF recurrence within the first year and foveal leakage points on FA. CSC patients with MNV were characterised by poorer visual acuity and a higher rate of incomplete fluid resolution. A longitudinal clinical study is required for further investigation.
Data availability statement
Data are available on reasonable request. Datasets for this study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The current study was performed following the Declaration of Helsinki and approved by the ethics committees of all participating facilities (Hyogo College of Medicine (No. 3251), Kagoshima University (No. 190273), Kobe University (No. B190181), Nagoya City University Graduate School of Medical Sciences (No. 60-19-0204), Nara Medical University (No. 1464) and Sapporo City General Hospital (No. R01-059-592)).
Acknowledgments
We thank Claire Barnes, PhD, Jane Charbonneau, DVM, and Melissa Crawford, PhD, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
References
Footnotes
Presented at The findings in this study were presented at the 125th Annual Meeting of the Japanese Ophthalmological Society, Osaka, Japan, 8 April 2021–11 April 2021.
Contributors Designing and conducting the study: YK and FG. Writing the manuscript: XZ. Collecting the data: XZ, TA, HT, AM, SK, TN and TK. Analysis and interpretation of the data: XZ. Critical revision of the manuscript: FG, YK, TK and AM. Guarantor: YK.
Funding This study was supported by grants from the Japan Society for the Promotion of Science (19K09963) and the Hyogo Innovative Challenge Project at Hyogo College of Medicine.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.