Article Text

Abstract
Purpose Pregnant and postpartum women living with HIV in South Africa are at high risk of dropping out of care, particularly after delivery. Population mobility may contribute to disruptions in HIV care, and postpartum women are known to be especially mobile. To improve engagement in HIV care during the peripartum period, we developed CareConekta, a smartphone application (app) that uses GPS coordinates to characterise mobility and allow for real-time intervention. We conducted a randomised controlled pilot study to assess feasibility, acceptability and initial efficacy of the app intervention to improve engagement in HIV care. This cohort profile describes participant enrolment and follow-up, describes the data collected and provides participant characteristics.
Participants We enrolled 200 pregnant women living with HIV attending routine antenatal care at the Gugulethu Midwife Obstetric Unit in Cape Town, South Africa. Eligible women must have owned smartphones that met the app’s technical requirements. Seven participants were withdrawn near enrolment, leaving 193 in the cohort.
Findings to date Data were collected from detailed participant questionnaires at enrolment and follow-up (6 months after delivery), as well as GPS data from the app, and medical records. Follow-up is complete; initial analyses have explored smartphone ownership, preferences and patterns of use among women screened for eligibility and those enrolled in the study.
Future plans Additional planned analyses will characterise mobility in the population using the phone GPS data and participant self-reported data. We will assess the impact of mobility on engagement in care for the mother and infant. We also will describe the acceptability and feasibility of the study, including operational lessons learnt. By linking this cohort to the National Health Laboratory Service National HIV Cohort in South Africa, we will continue to assess engagement in care and mobility outcomes for years to come. Collaborations are welcome.
Trial registration number NCT03836625.
- HIV & AIDS
- Epidemiology
- PUBLIC HEALTH
- Maternal medicine
Data availability statement
De-identified data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The study provides a rich dataset from a recent study cohort (2019–2021) of particular interest to those wishing to study pregnant and postpartum populations living with HIV and accessing public antenatal care in South Africa, or those interested in mHealth interventions.
The participant-reported data include few missing data.
The limited sample size (n=193) is a weakness of the study.
The study was conducted at a single site in South Africa, but one that should be representative of other public healthcare facilities in the area.
There is substantial missing GPS data.
Introduction
South Africa has the largest number of people living with HIV (PLWH) worldwide, constituting 7.7 million in 2018, of whom 4.7 million (61%) were women aged 15 years and older.1 Despite the availability of effective interventions, the rate of new HIV infections remains unacceptably high across sub-Saharan Africa,2 and retention in HIV care continues to be a significant challenge.3 Pregnant and postpartum women are at particularly high risk of dropping out of HIV care, especially in the postpartum period.4–9 Various studies have identified and documented barriers to engagement in HIV care, including medication side effects, complexity of dosing schedules, low patient education level, poverty, stigma, distance and transportation challenges, quality of care received and reliance on traditional medicines.10–13 However, one potential barrier to continuous engagement in HIV care and treatment that is gaining attention is the mobility of people between regions and countries.7 14 15 In 2011, UNAIDS and the International Organization for Migration, signed an agreement recognising HIV-related challenges faced by mobile populations with objectives to integrate human rights and the needs of mobile populations into national and regional HIV responses and to ensure universal access to HIV prevention, treatment, care and support.3
Population mobility has long been recognised as one of the main catalysts of the spread of the HIV epidemic.16–18 Recent studies have shown that the mobility of PLWH may also result in poorer response to HIV care and treatment initiatives, leading to an overall negative impact on the health and economic status of this population.3 19 20 In Lesotho, a study looking at barriers to access of PLWH migrating to South Africa found that roughly 25% had interruptions to their treatment.20 Our earlier work showed that among pregnant women, the postpartum period is a time of frequent mobility, which contributes to gaps in HIV care.7 21
As countries move toward the UNAIDS 95-95-95 treatment goals and beyond, how population mobility influences HIV and maternal care effectiveness remains crucial.22 Expansion of HIV treatment delivers undeniable health benefits, including substantial gains in life expectancy23; however, challenges arise in ensuring continuous, lifelong engagement in HIV care.24 Population mobility affects engagement in HIV care as a barrier to both individual access to healthcare facilities and the ability to determine if an individual is truly lost from care.25 Given the absence of linked data networks at healthcare facilities, individuals who drop out of care at one facility may continue at a second facility, known as ‘silent’ or ‘unofficial’ transfer5; this may underestimate engagement.4 ‘Tracing’ studies that evaluate outcomes among lost patients in the community provide further insight into retention in care by documenting patient movement across clinic sites, in many instances patients who are lost to follow-up continue to receive care at other, more local facilities.26–28
Mobile health (mHealth) technologies are increasingly being used as tools in the promotion of maternal and child health, including to support antenatal, delivery and postnatal care in communities.29 mHealth interventions can be useful for improving coverage of community-based maternal, neonatal and child health services where healthcare access challenges exist,30 particularly in resource-limited areas.31 32 mHealth applications are widely becoming effective methods to improve how clients and health providers exchange health information, and they also present opportunities to enhance the quality of maternal and child health services provision, particularly in under-resourced health systems.31 Globally, evidence shows that mHealth applications may be useful responses for successful maternal, neonatal and child health, including increased antenatal care attendance, postnatal care attendance and immunisation rates.33–35
Given this background, the study sought to develop an mHealth smartphone application (app)—CareConekta—to observe mobility within an observational cohort of pregnant women living with HIV and then assess the impact of an intervention among participants who travelled during the study period. The app was devised by the study investigators in parallel with a series of focus group discussions with potential users,36 developed as a beta version at Vanderbilt University Medical Center by Dr Martin Were and team, and then redeveloped and adapted by Jembi Health Systems in Cape Town. The CareConekta app prospectively characterises mobility and allows for intervening in near real-time. Regular ‘heartbeat’ signals from the phone’s GPS system provided the participant’s current location geo-coordinates, which were made ‘fuzzy’ by transmitting a random location within 1 km of each exact location to protect privacy. We conducted a randomised controlled pilot study to assess feasibility, acceptability and initial efficacy of the app intervention to improve engagement in HIV care. Full details of the study activities can be found in our published protocol.25
Cohort description
Study setting and dates
The study enrolled 200 women attending routine antenatal services at the Gugulethu Midwife Obstetric Unit (MOU), based at the Gugulethu Community Health Centre in Cape Town, South Africa. The MOU is a public-sector clinic operated by the Western Cape Department of Health that serves the township of Gugulethu, a peri-urban setting, as well as the surrounding informal settlements. Recruitment began in December 2019 and ended in February 2021. There was a 6-month pause on recruitment from March to September 2020 due to the COVID-19 pandemic, per the guidance of the local ethics board. Participant follow-up ended in November 2021.
Study eligibility and retention
Women were eligible for study participation if they met the following enrolment criteria:
Age ≥18 years.
Living with HIV.
In third trimester of pregnancy (≥28 weeks).
Able to speak and understand isiXhosa and/or English (demonstrated by asking the participant to read aloud the following sentence in either English or isiXhosa: ‘I can look up a new clinic on the phone’).
Own a smartphone that meets the technical requirements of the CareConekta app. (Android operating system, V.5.0 or later; cellular service on one of the four major local providers (Vodacom, Cell-C, Telkom, or MTN); can demonstrate use of GPS by opening a map app; can hold a battery charge (charging no more than two times per day).
Willing to opt-in to installation of CareConekta on her personal phone and mobility tracking.
Demonstrate basic smartphone-level literacy.
Willing to be randomised.
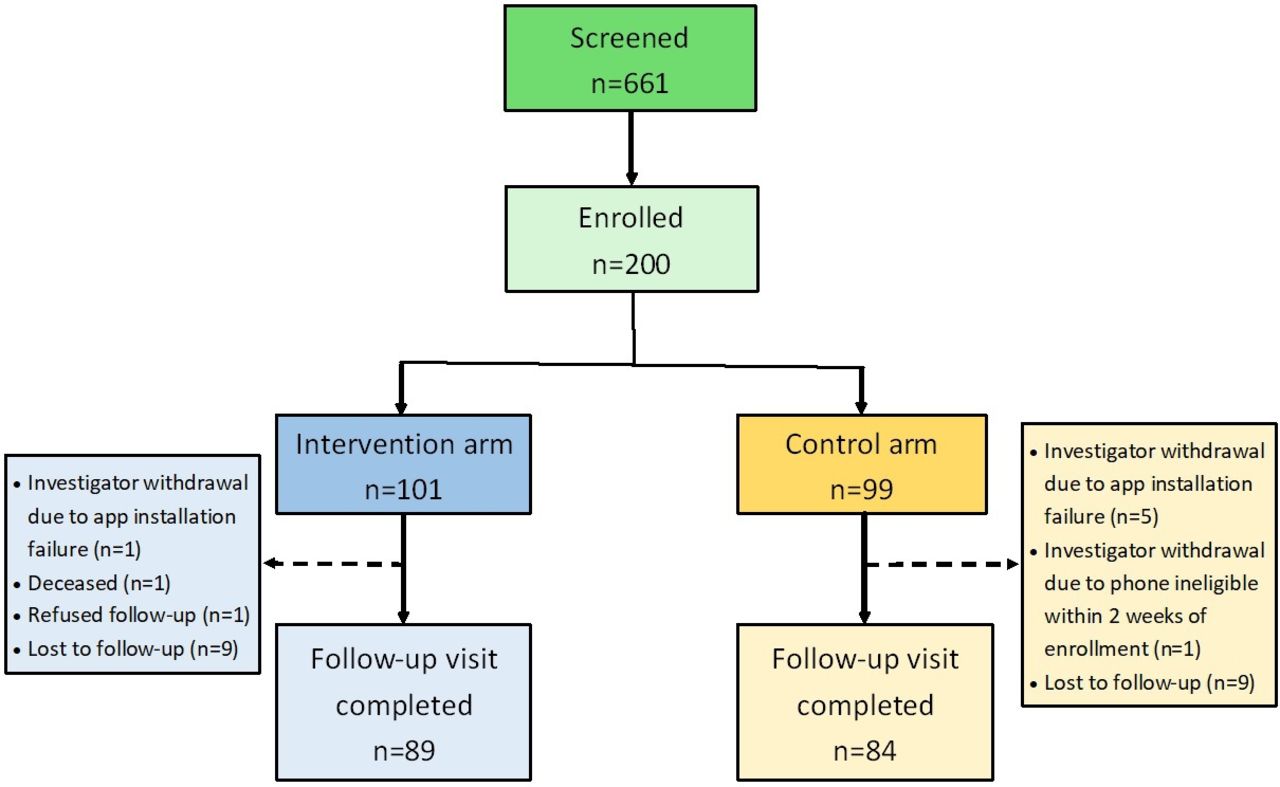
Of the 200 women enrolled, seven were withdrawn by the investigative team at enrolment due to app installation failure (n=6), or soon after (within 2 weeks) enrolment due to the participant changing to a phone that no longer met the study criteria (n=1). Of the 193 participants who continued in the study, 173 (89.6%) completed the study, 18 (9.3%) were lost to follow-up, 1 (0.5%) participant refused follow-up and 1 (0.5%) participant died. The full study flowchart is shown in figure 1.
{kind=link}
CareConekta study flowchart.
Patient and public involvement
Development of the study design, intervention and outcome measures of the CareConekta study were informed by earlier developmental work with pregnant and postpartum women in public health facilities in South Africa, including the study site.36–38 The goal of this early research was to understand preferences for and initial acceptability of proposed interventions. Participants were not involved in the design or recruitment of the CareConekta study. Results will be shared with the study site leadership and staff, and with the Gugulethu community advisory board for community-level dissemination.
Ethical considerations
The study protocol and all activities were approved by the institutional review boards of Vanderbilt University and the University of California, San Francisco, and the Human Services Research Committee of the University of Cape Town. All women provided written informed consent, which included explicit consent for GPS location tracking, prior to study participation.
Data collection and study measures
Participant-reported data were collected through face-to-face or telephonic (due to COVID-19 restrictions) interviews at enrolment and study end (approximately 6 months after delivery). All interview questions were categorical or short answer. Questionnaire data were collected directly on a tablet or laptop computer, and entered into a secure, encrypted REDCap database.39 Additionally, we collected GPS data from the CareConekta app, clinical data from the South African government-mandated Maternity Case Record and the infant Road to Health card, and additional routine electronic medical record (EMR) data from the Western Cape Department of Health. By using routine EMR data, all patients will have an engagement in care outcome at 6 months, even if the participant does not attend the final study visit. A summary of data fields collected in the study is shown in table 1.
Data fields collected in the CareConekta study
Study participant characteristics
Characteristics of the enrolled participants are shown in table 2.
Characteristics of participants in the CareConekta cohort in Gugulethu, South Africa (n=193)
Findings to date
An early analysis explored smartphone ownership, preferences and patterns of use among enrolled and not enrolled women screened for eligibility in the study, and found that smartphone ownership among women attending routine antenatal services in this region was high (87%) and phone sharing was limited.40 Additional planned analyses will characterise mobility in the population using the phone GPS data, and participant self-reported data. We will assess the impact of mobility on engagement in care for the mother and infant. We also will describe the acceptability and feasibility of the study, including operational lessons learnt.
Additional ongoing cohort activities include merging the CareConekta dataset with the South African National Health Laboratory Service (NHLS) National HIV Cohort. The NHLS has maintained laboratory test results for nearly all patients receiving care in the public health system in South Africa since 2004.41 By linking to this open national cohort, we will continue to report treatment outcomes, such as HIV viral load and CD4, at time periods well beyond the initial data collection period, such as at 24-month and 48-month follow-up. This dataset linkage also allows for long-term prospective analyses of mobility on a national level, since data for clinics throughout South Africa are reported to NHLS.
Data availability statement
De-identified data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Vanderbilt University IRB: 181640; University of California, San Francisco IRB: 18-26811; University of Cape Town HSRC: 659/2018. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors are most grateful to the study participants, without whom this work would not be possible. We also wish to acknowledge the Western Cape Department of Health and their provincial data center that facilitate longitudinal patient follow-up. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the article. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or other parties.
References
Footnotes
Contributors KC and NN wrote the initial draft of the paper. KC, TKP and LM provided accountability and oversight to all study procedures. KC is the study principle investigator and TKP is the site PI. SN, SM and MM contributed to data collection and management. CSC and LM contributed to study design and consultation. All authors have approved this manuscript. KC is the author responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.