Article Text

Abstract
Aims Cancer is a well-known risk factor of venous thromboembolism (VTE). Some cancers are believed to be more thrombogenic. The purpose of this study was to investigate the characteristics of patients with incident gastrointestinal cancers (GI) and their associated 1-year risk and timing of venous thromboembolic events and the 1-year mortality.
Methods This study was a retrospective cohort study. Through Danish nationwide registries, all patients with first-time GI cancer diagnosis from 2008 to 2018 were identified. Incident VTE events were identified within a 1-year follow-up after GI cancer diagnosis using the Aalen-Johansen estimator. Cox proportional-hazard models were applied to investigate risk factors for VTE events and the impact of VTE on mortality.
Results A total of 87 069 patients were included and stratified by cancer types: liver (5.8%), pancreatic (12.0%), gastric (6.9%), small intestinal (1.9%), colorectal (61.8%), oesophageal (7.3%) and gallbladder (3%). Most VTE events happened close to onset of the cancer diagnosis with declining events by time. The 1-year cumulative incidence of VTE differed according to cancer type with pancreatic cancer being most thrombogenic (7.8%), and colorectal and liver cancer being the least (3.6%). Prior VTE, heart failure, chronic obstructive pulmonary disease (COPD), liver disease, chronic kidney disease (CKD) and diabetes increased the VTE risk. Overall, the patients with GI cancer had high 1-year mortality of 33.3% with patients with pancreatic cancer having the highest mortality (70.3%).
Conclusion We found that most VTE events happen close to onset of the GI cancer diagnosis and thrombogenicity differed by type of GI cancer, ranging from 7.8% in patients with pancreatic cancer to 3.6% in colorectal and patients with liver cancer. Prior VTE, heart failure, COPD, liver disease, CKD and DM were associated with increased risk of VTE.
- Gastrointestinal tumours
- Thromboembolism
- Cardiology
Data availability statement
Data are available on reasonable request. The data are stored at Statistics Denmark and research environments can apply for access.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Based Danish high-quality registries.
Large population size, n=87.069.
Residual confounding may influence the results.
Introduction
Venous thromboembolism (VTE) comprising deep VTE and pulmonary embolism is a well-established and potential life-threatening condition often observed in patients with gastrointestinal (GI) cancers.1 Although, the estimated incidence of VTE in particular has been reported high in patients with pancreatic and gastric cancer, it has still not been fully established which types of GI cancer are most prone to VTE. For instance, a newer prediction model, that still needs validation, found that patients with colorectal cancer have higher risk of VTE events than previously predicted.2 Moreover, as prognosis of GI cancer has improved and the risk of VTE correspondingly has increased,3 the timing of VTE events, that might be closely related to time of cancer diagnosis, has not been fully investigated.
Further, although low-molecular-weight heparin is recommended as thromboprophylaxis in patients with cancer, a treatment shift towards direct oral anticoagulant (DOAC) therapy is relevant in an era where the safety and efficacy of DOAC therapy has been well established.4 5
Studies on the VTE burden of cancer disease and the patient characteristics are warranted to ensure better understanding. Therefore, using nationwide Danish registers we sought to examine the 1-year risk and risk factors for incident VTE and the timing thereof in organ-specific patients with GI cancers. Further, we aimed to estimate the overall organ-specific mortality of patients with GI cancer.
Methods
Data sources
This study was a retrospective, observational, cohort study. In Denmark, every citizen is assigned a unique civil registration number at birth or on immigration.6 Using this number, it is possible to link several Danish nationwide registries at an individual level, thus making it possible to follow each citizen either at the hospital or at an outpatient clinic regarding diagnosis, migration, filled drug prescriptions or death. We leveraged information from the following registers: The Danish National Patient Register (DNPR) contains data on hospital admissions, visits to outpatient clinics and procedures or operations.7 The Danish National Prescription Register contains information on all filled prescriptions, including drug, quantity, strength, number of packages and dispensing date.8 Enrolment in the Danish registries is mandatory and does not require patient consent, making the datasets complete with no missing data at follow-up. The data are stored at Statistics Denmark and research environments can apply for access.
Study population
We included all Danish patients 18 years or older diagnosed with GI cancers between 1 January 2008 and 31 December 2018. GI cancer was divided into seven organ-specific groups: oesophageal, gastric, liver, gallbladder, pancreatic, small intestinal and colorectal. Patients were included at the date of first-time GI cancer diagnosis either at first hospital admission, or first visit to an outpatient clinic due to cancer. Patients not residing in Denmark at time of diagnosis and patients with GI cancer with unknown location were excluded. Patients with a primary, secondary or basic diagnosis were included. A detailed description of the GI cancer diagnoses used in the study is listed in online supplemental table S1.
Supplemental material
Outcome measures
The primary outcome was first incident VTE event. All VTE events on the date of cancer diagnosis and within 1 year thereafter were identified. VTE events included were first registered diagnosis of either deep VTE or pulmonary embolism. Diagnose codes used are listed in online supplemental table S1.
Comorbidities and medications
Relevant comorbidities, prior VTE, chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), heart failure, ischaemic heart disease, atrial fibrillation and prior non-GI cancer were identified 5 years prior to first GI cancer date using the DNPR. Relevant medications included oral steroids, antipsychotics and OAC treatment and were identified 180 days prior to first GI cancer date using The Danish National Prescription Register. Diabetes (DM) was defined from use of a diabetes medicine and hypertension was defined from usage of at least two antihypertension medicines. Diagnose-and ATC codes for comorbidities and medication use are listed in online supplemental table S1,S2.
Statistical analysis
Descriptive tables and charts were employed to describe the study population (first hospital contact due to GI cancer) and categorical variables summarised with counts and percentages.
The timing of the VTE incidence was estimated using the Aalen-Johansen estimator, taking the competing risk of death and emigration into account, and depicted graphically. Further, the cumulative incidence was investigated at certain time points and reported.
The 1-year risk of VTE was estimated and stratified by GI cancer groups and age groups using the Aalen-Johansen estimator and presented graphically and by counts and percentages with corresponding 95% CI.
Risk factors for the primary outcome were examined using multivariable survival analysis by Cox proportional-hazards models, presented as HRs with corresponding 95% CI. The risk factors included in the analysis were sex, age, a history of VTE, heart failure, peripheral vascular disease, COPD, CKD, diabetes and hypertension. Mortality was high in this patient category but use of the Cox model enabled censoring. Further, patients that emigrated were censored. Assumptions for proportionality were tested and verified with graphical test by visual inspection of log-minus-log plots.
The incident 1-year mortality was investigated compared with index date and presented as counts and percentages. The impact of a VTE event on mortality was examined using Cox proportional-hazards models, using the exposure group as time dependent covariates. The models allowed patient-switching regarding exposure groups. The Cox model was multivariable and adjusted for sex, age, a history of VTE, heart failure, peripheral vascular disease, COPD, CKD, diabetes and hypertension.
Analyses and data processing were performed with R. statistics (R Core Team (2015). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL http://www.R-project.org/.)
Patient and public involvement
No patients were involved in this study. Only registers were applied.
Results
Study population
A total of 88 122 patients were identified with GI cancers from 1 January 2008 to 31 December 2018 of which 1053 were excluded. The final cohort consisted of 87 069 patients and a detailed description of the baseline characteristics is given in table 1. A total of 5070 (5.8%) patients had liver cancer, 11 351 (12%) pancreatic cancer, 5990 (6.9%) gastric cancer, 1638 (1.9%) small intestinal cancer, 54 024 (61.8%) colorectal cancer, 6357 (7.3%) oesophageal cancer and 2639 (3%) had gallbladder cancer (figure 1). The groups were relatively homogeneous on age (median age ranged from 68.2 to 72.4 years). Men experienced more oesophageal, liver and gastric cancer and less gallbladder cancer than their female counterparts. Comorbidities were evenly distributed, except from patients with liver and pancreatic cancer having more diabetes. A prior VTE event ranged from 1.9% to 4.1% in small intestinal and pancreatic cancer patients, respectively. Baseline use of OAC therapy ranged from 7.5% to 9.3% in small intestinal and patients with liver cancer, respectively. The mean duration of follow-up time was 271 days (SD±137 days).
Baseline characteristics of the study cohort
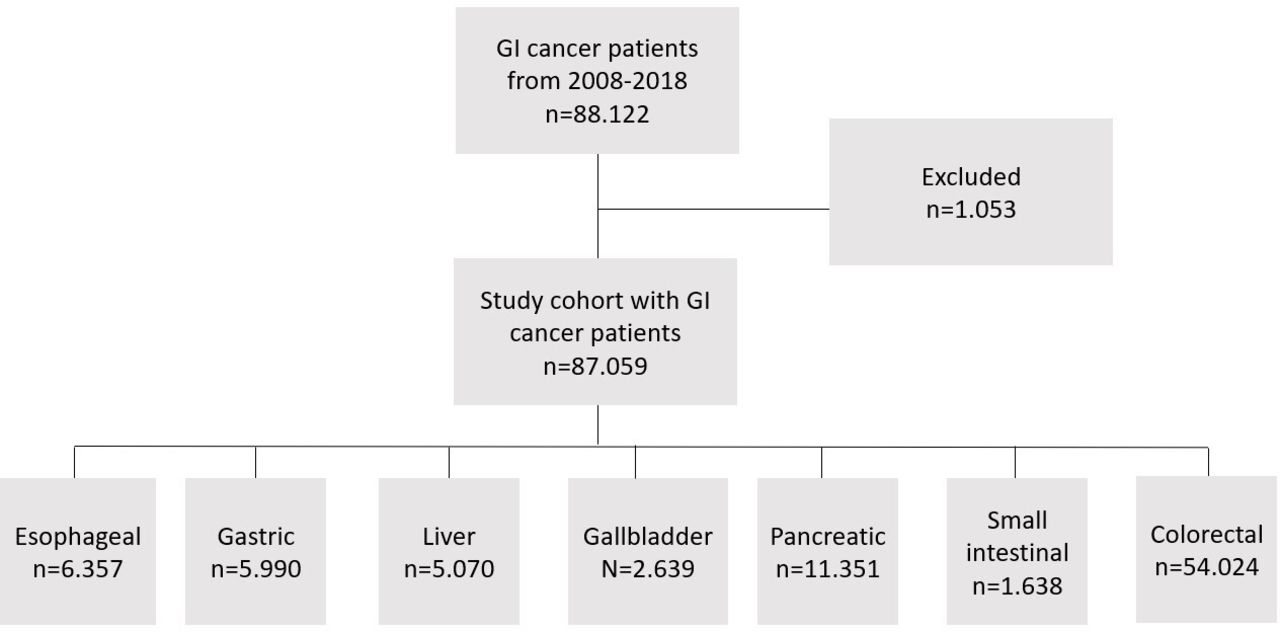
Flow chart. Study cohort comprised patients with GI cancer from 2008 to 2018 and further divided into organ-specific cancers. GI, gastrointestinal.
Timing of incident VTE
In total 3827 patients experienced a VTE event during the 1-year follow-up, corresponding to an absolute VTE risk of 4.4%. Figure 2 shows that the incidence of VTE was highest in the initial period after index GI cancer diagnosis. Table 2 emphasises that most VTE events happen in the initial 120 days; the cumulative incidence of VTE after 120 days compared with 365 days varied from 54% in patients with oesophageal cancer to 74% in patients with pancreatic cancer.
One-year incidence of VTE and mortality and 120-day incidence of VTE in patients with gastrointestinal cancer

The cumulative 1-year VTE incidence rate for all GI cancer types, demonstrating the timing of the VTE event. The x-axis depicts days and the y-axis depicts incident VTE events. GI, gastrointestinal; VTE, venous thromboembolism.
Incident VTE by GI cancer groups: primary results
Figure 3 depicts the 1-year cumulative incidence of VTE by GI cancer groups. There was a substantial difference ranging from 3.6% in patients with liver or colorectal cancer to 6.4% and 7.8% for patients with gallbladder and pancreatic cancer (figure 3 and table 2).

The cumulative 1-year VTE incidence rate in patients with GI cancer by cancer type. The x-axis depicts time in days and the y-axis depicts the cumulative 1- year VTE incidence. GI, gastrointestinal; VTE, venous thromboembolism.
Of significant patient characteristics and comorbidities and their Hazard ratios HR (95% CI), age over 79 years 1.58 (1.52 to 1.65), a history of previous VTE 1.09 (1.02 to 1.16), heart failure 1.14 (1.09 to 1.19), COPD 1.12 (1.08 to 1.16), liver disease 1.40 (1.33 to 1.46), CKD 1.23 (1.16 to 1.30) and DM 1.08 (1.05 to 1.11) were associated with an increased risk of a VTE event (figure 4). Male sex decreased the risk of an event 0.98 (0.96 to 1.00).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forrest plot of comorbidities that influence the risk if a VTE event. COPD, chronic obstructive pulmonary disease; VTE, venous thromboembolism.
Mortality
A total of 29 130 (33.3%) patients died. Table 2 shows that mortality was highest in patients with pancreatic cancer (70.3%) and lowest in patients with colorectal cancer (20.6%), respectively.
The impact of a VTE event on death, examined by the multivariable Cox analysis, showed an HR of 1.45 (95% CI 1.40 to 1.50).
Discussion
In this nationwide study, we examined the timing and 1-year incident VTE risk in organ-specific patients with GI cancer and their mortality. We found that most VTE events happened close to the onset of GI cancer diagnosis and a wide variation in thrombogenicity by organ-specific GI cancer type with highest risk for VTE in patients with pancreatic cancer. We found a high overall 1-year mortality in the GI cancer population, and we found that a VTE event increase the mortality risk.
The timing of VTE events after cancer diagnosis is poorly elucidated. A Danish registry-based study from 2021 investigated this among patients with ovarian cancer and observed that that most VTE events seem to happen close to onset of ovarian cancer diagnosis.9 A relatively large amount of our incident VTE events happen at diagnosis of GI cancer. Whether patients are admitted due to VTE or GI cancer is unknown. But after taking this into account, we still find that the risk of VTE is highest within around 120 days after onset of GI cancer diagnosis.
Our findings that patients with upper GI cancer, especially patients with pancreatic and gastric cancer, were more susceptible to VTE events compared with patients with lower GI cancers, are in line with previous findings.10 11 Gallbladder cancer is often omitted when assessing the risk of VTE, probably due to the relatively small population, but our findings suggest, that it is among the most thrombogenic cancer groups. Khorana et al developed a prediction score (The Khorana score), which has been validated to predict which types of organ-specific cancers are more thrombogenic, dividing cancers into very high risk (eg, pancreatic and gastric cancers), high risk (eg, lung cancer) and low risk (eg, colorectal cancer).12 Our results support the Khorana score which states that gastric and pancreatic cancers are more thrombogenic than for instance colorectal cancers and our VTE incidence rates are comparable.12 On the other hand, in colorectal cancer, we found an incidence of VTE events of up towards four times higher, compared with the Khorana study.10 This might be due to the difference in the study design, leading to a median follow-up time of 73 days in the Khorana study. At the present time, the Khorana score is still the most used prediction model, when it comes to predicting VTE events in patients with cancer. This is despite the fact that the score is based on non-contemporary data with a limited patient population.10 Nonetheless, since the introduction of the Khorana score, it has been vigorously tested, for instance in a recent meta-analysis that concluded that the Khorana score remains valid.13 More precise prediction models that still require prospective validation are on the way. One difference for instance is colorectal cancers have been upgraded to ‘high risk of VTE’.2
Regarding risk factors, our data showed that patients with prior VTE, heart failure, COPD, liver disease, CKD and DM had an elevated risk of VTE. This might indicate that newly diagnosed patients with GI cancer with one or more other risk factor might benefit from primary prophylactic OAC treatment. This study and other similar studies are important due to the current investigation in whether patients with cancer should be administered primary thromboprophylaxis treatment due to the increased risk of VTE events. Previously, the prophylactic effect of low-molecular-heparins in VTE incidence in patients with cancer have been studied. A comprehensive review was conducted in 2016 and showed a significant reduction in VTE incidence without a significant increase in major bleeding events.14 A limited number of clinical studies have been conducted examining the effect of prophylactic OAC treatment in patients with cancer, and currently, there is no consensus regarding the effect of prophylactic OAC in patients with cancer. This is exemplified in two recent studies with comparable protocols displaying deviating conclusions using non-vitamin K antagonist oral anticoagulants; one study found a significant risk reduction of VTE incidence, the second found no significant risk reduction.4 15
Our high mortality is comparable to previous studies. A global surveillance study of cancer survival was published in 2014. They examined various cancer types including gastric and colorectal cancer and their estimated 5-year survival. Their data included the Danish registries, and they found a 5-year survival probability of 18% and 57% in patients with gastric and colorectal cancer.16
Strengths and limitations
There are several strengths in this study; first, our population is an unselected GI cancer population from nationwide registries, limiting selection bias markedly compared with most of the studies examining the subject. Second, the registries provide a large population resulting in high-quality real-world data. Third, the registries have been tested vigorously and validated with high positive predictive values of first time VTE and the GI cancer diagnosis.17 18 However, there are some limitations to the study; even though the registries have been validated, misclassification bias has not been fully eliminated. Residual confounding might affect our results; in our registries, we do not have access to parameters like body mass index, smoking status and clinical factors such as eGFR, hepatic lab values and blood pressure. We do not have valid data available on chemotherapy and use of low-molecular heparins, as these are hospital administered. Patients might die from VTE at home without being diagnosed as some patients are classified terminally ill. Lastly, our registries lack valid information on cancer stages and metastasis.
Conclusions
We found that occurrence of VTE events happens close to onset of the GI cancer diagnosis and that pancreatic, gallbladder and gastric cancers were the most thrombogenic among the GI cancer types. Prior VTE, heart failure, COPD, liver disease, CKD and DM were associated with increased risk of VTE. We observed a high mortality, and we found that mortality was further increased by a VTE event.
Data availability statement
Data are available on reasonable request. The data are stored at Statistics Denmark and research environments can apply for access.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @JacobTonnesenMD
Contributors MLH and JT conceived the study idea. JT, MLH, MHR, PVR and JP designed the research. JT performed the statistical analysis and wrote the manuscript. JT, PVR and JP contributed to the programming. All authors, including ML, NN, JS and GHG, critically revised and approved the manuscript. JT is the guarantor.
Funding This study was sponsored by Pfizer Denmark and Bristol Myers Squibb Denmark. Grant number is not available.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.