Article Text

Abstract
Objective The adverse effects of poor social support on quality of life and adherence to treatment are established. However, the relationship between social support and depression is not well understood. In this systematic review and meta-analysis, we aim to examine the association between social support and depressive symptoms among type 2 patients with diabetes.
Design Systematic review and meta-analysis.
Data sources We searched PubMed, African Journals Online, Web of Science, and the Cochrane Library electronic databases. Some studies were also identified through manual Google search and Google scholar.
Eligibility criteria We systematically searched electronic databases for studies published up to October 2020. Only English-language articles were included.
Data extraction and synthesis Screening, data extraction and quality appraisal were conducted by two independent reviewers. A random-effect model was applied to estimate ORs with 95% CIs. The Higgins I2 test was used to assess the heterogeneity between the studies. The risk of publication bias was estimated using the Egger test. Leave-one-out analysis was done. Data were analysed using Stata V.11.
Results Seven studies were included in the meta-analysis. The findings from included studies revealed that poor social support increases the odds of depression among patients with diabetes (adjusted OR=2.14, 95% CI 1.34 to 3.43, p=0.003). There was no risk of publication bias (p=0.064), and heterogeneity was substantial (I2=70.7%). The leave-one-out analysis confirmed the consistency of the findings.
Conclusions Our meta-analysis revealed that patients who had poor social support were significantly associated with an increased level of depression. Additional studies exploring factors that might moderate or mediate this association are needed. Targeted interventions for comorbid depression should be implemented in clinical practice.
Systematic review registration We have submitted the protocol for registration at the PROSPERO on 9 October 2020. But we have not yet received a registration number.
- general diabetes
- depression & mood disorders
- social medicine
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
All relevant studies on the association between social support and depression among patients with diabetes were identified using varieties of sources.
Subgroup analyses were done to identify the sources of heterogeneity based on several important possible confounding factors.
A difficulty in combining all of the results due to substantial heterogeneity between studies.
Inconclusive results due to a small number of studies and the scarcity of multivariate analyses.
Introduction
Diabetes mellitus is a highly prevalent chronic disease that requires continuous medical care combined with patient self-management and family support.1 It is a major worldwide public health concern and this is probable to be among the five leading causes of disease burden by 2030.2 Similar to other chronic medical conditions, diabetes is complicated by emotional and psychological disorders. There is a bidirectional association between diabetes and depression. The presence of diabetes increases the probability of depression and stress. Similarly, depression and stress make the suffering people more vulnerable to becoming diabetic.3 4
Depression among patients with diabetes is highly prevalent. Studies revealed that about 20%–25% of patients with diabetes develop symptoms of depression.5 6 In Ethiopia, the incidence of type 2 diabetes and depression is increasing due to the national increase in obesity. In the country, an estimated 15%–20% of people with diabetes are struggling with depression.7–9
Depression in patients with diabetes is often associated with poor glycaemic control, poor medication adherence and rapid development of complications. But, depression is a modifiable risk factor. Therefore, reducing depression could improve glycaemic control and health outcomes in patients with diabetes. One of the possible strategies to reduce depression among patients with diabetes was strengthening social support.10–12
Social support refers to a psychosocial resource that is accessible in the context of interpersonal contacts and one’s social network.13 Social support can be either perceived availability of support in the future or actually received support in the past. Perceived social support refers to an individual’s expectancy to obtain support if required,13 14 and received social support refers to the past experience of actually obtaining support.15 16
Literature shows that social support plays a pivotal role in patients with diabetes and can contribute to the successful management of the disease.17–19 Social support helps with diabetes control and provides support for the necessary physical and dietary changes.20 The source of support can be family,21 friends, healthcare providers and religious leaders.20 22
A large body of literature has examined the relations between social support and depression. However, the exact nature and direction of these relations are not well understood. Despite the abundance of research on the predictor of depression among patients with diabetes, there is a scarcity of concrete evidence on the association between social support and depression among patients with diabetes in Ethiopia. The aim of this study was to assess the association between social support and depression among type 2 patients with diabetes.
Methods
Searching
We systematically searched PubMed, African Journals Online, Web of Science and the Cochrane Library databases for articles published up to October 2020 (online supplemental file 1). Additionally, we searched via Google search for non-indexed articles and appropriate grey literature (evidence not published in commercial publications, including theses and dissertations, research and committee reports, government reports, conference papers and ongoing research), and also through checking references of one systematic review on the prevalence of depression among patients with diabetes in Ethiopia.23
Supplemental material
We used the Medical Subject Heading (MeSH) Terms and free-text terms for the search strategy. The search terms were used separately and in combination using Boolean operators like ‘OR’ or ‘AND’. We search in PubMed using the following search phrases: (((((Depression[MeSH Terms]) OR (depress*[MeSH Terms])) OR (“Mental disorder”[Text Word])) OR (“Mood disorder”[Text Word])) AND (((((“Social Support”[MeSH Terms]) OR (“Community support”[MeSH Terms])) OR (“psychosocial support”[MeSH Terms])) OR (Predictors[MeSH Terms])) OR (“Risk Factors”[MeSH Terms]))) AND ((Diabetes Mellitus) OR (Diabetes[MeSH Terms])).
Eligibility criteria
We included observational studies providing information on the association between social support and depression in samples of people suffering from diabetes.
Inclusion criteria
Studies were selected according to the following study characteristics: study design, participants, exposure/interventions, comparators, outcomes (PECO/PICO framework):
Study design
All epidemiological studies (cross-sectional, cohort, case–control) reporting associations between social support and depression were included.
Population
Participants in the included studies were adults (age ≥18 years) with diabetes mellitus.
Intervention/exposure
In the current study, the exposure can be either perceived or received social support. Perceived social support refers to the subjective perception of support being available from one’s friends, family, teammates who may assist if needed. On the other hand, received social support refers to support actually received. In the majority of the included studies, the level of social support was assessed by using the Oslo-3 social support scale by asking the patients to rate the level of support they received from family and friends. It is validated in different African countries.
Comparators
The comparator group was patients with diabetes who had poor social support, which is defined as Oslo-3 social support score 3–8 or either the study used the term low or mild or poor.
Outcome measure
The main outcome of interest was depression. We included all studies, which assessed depression by self-report measures or diagnostic interviews. The self-report scales including the Patient Health Questionnaire,24 Beck Depression Inventory25 and the Centre for Epidemiologic Studies–Depression Scale were used.26 Depression was assessed with the Hospital Anxiety and Depression Scale-Depression. The diagnostic interviews were based on the criteria of the Diagnostic and Statistical Manual of Mental Disorders or International Classification of Diseases27
We included studies reported in English languages and carried out in Ethiopia. Articles that met the criteria were considered irrespective of their publication status that is published, unpublished or grey literature.
Exclusion criteria
Articles were excluded if (1) depression could not be distinguished from anxiety or distress, (2) OR or relative risk (RR) could not be calculated, for example, we excluded studies that reported only mean of depression measures, (3) used rating scales to assess depressive symptoms if these did not provide a standardised cut-off value for clinical depression, (4) studies showing data overlap with other studies included in the meta-analysis, in order to prevent bias due to data duplication. Reviews, letters and duplicate studies were also excluded.
Data extraction
A structured data extraction format was developed to collect relevant data from eligible papers. The data were extracted by two independent reviewers (GD and AA), and they assessed the methodological quality of each paper. The following study characteristics were extracted from the studies: first author, publication year, region (state) where the study was conducted, study design, sample size and effect estimate (OR or RR) and 95% CI. Any disagreements between the two reviewers on the extraction of the data were settled through discussion and consensus. In addition, the variation was also resolved by involving a third reviewer (MLE).
Risk of bias (quality assessment)
The methodological quality of each study was assessed using the Newcastle-Ottawa quality assessment tool adapted for a cross-sectional study.28 The tool has three indicators. The first section is graded out of five stars and assesses the quality of the methodology of a study. The second part of the tool is graded out of three stars and assesses the comparability of the studies. The last part of the tool is graded from two stars and measures the quality of statistical analyses of original studies. Using the tool as a protocol, two independent authors evaluated the quality of the original articles. Thus, the maximum for each study is 9, with studies having less than 5 points being identified as representing a high risk of bias. Those studies with medium (fulfilling 50% of quality assessment criteria) and high quality (≥6 out of 10 scales) were included for analysis.
Outcome of interest
The outcome of this systematic review and meta-analysis was to assess the association between social support and depression.
Statistical analysis
The relevant data were extracted from each paper using Microsoft Excel V.2013 format and then analysed using Stata (V.11.0) software. The primary articles were summarised using the forest plot. The magnitude of heterogeneity across the studies was assessed using I2 value. I2 ranged between 0% (no heterogeneity) and 100% (high heterogeneity), with values of 25%, 50% and 75% suggesting low, medium and high heterogeneity, respectively. To weigh up the relative impact of each individual study, a leave-one-out sensitivity analysis was performed by excluding one study at a time and assessing the alteration in pooled results. Potential publication bias was also assessed subjectively by funnel plot and objectively using Egger’s regression test. In Egger’s tests, a p value of less than 0.05 indicates the presence of publication bias while a p value ≥0.05 indicates that there is no publication bias. As all of the included studies were cross-sectional, OR with 95% CI was used to report the association between social support and depression.
Patient and public involvement statement
Patients were not directly involved in the design of this study. As this is a protocol for a systematic review, no participant recruitment will take place, their involvement in the recruitment and dissemination of findings to participants was not applicable.
Results
Searching results
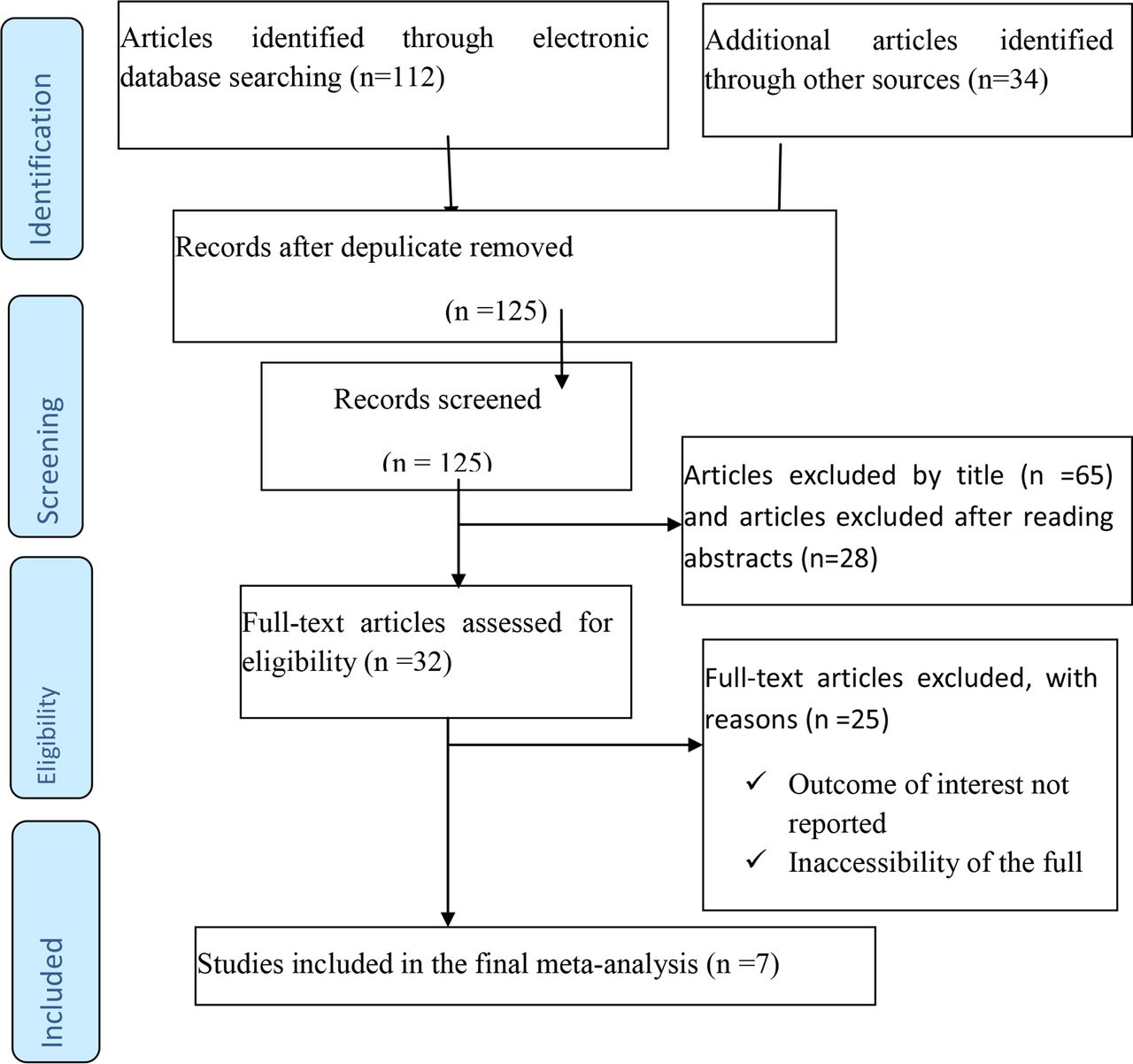
Our search identified 146 published articles, of which 112 articles were found in the electronic databases; the remaining were found in university libraries and reference lists. Of the total identified, 21 articles were excluded at the initial assessment. After evaluating the titles and abstracts, 93 studies were excluded because they were irrelevant to this meta-analysis. Furthermore, 32 full-text articles were assessed for eligibility. After excluding 25 records with insufficient or irrelevant data, 7 studies were included in the meta-analysis (figure 1).

Flowchart of study selection for systematic review and meta-analysis on the association between social support and depression among patients with diabetes in Ethiopia.
Study measures
For the aim of this review, we allowed the broadest definition of ‘social support’ employed by the studies under review, defining it as having friends and other people, including family and religious leaders, to turn to in times of need or crisis to give you a broader focus and positive self-image. We also allowed the broadest definition of ‘depression’ employed by the studies under review. Our principal summary measure was the odds of ‘depression’, that is, an OR either directly reported or calculated from the study outcomes presented.
Characteristics of original studies and quality assessment
As described in table 1, in the present meta-analysis, a total of 2543 study participants were included to estimate the pooled effect size of the association between social support and depression. The sample size ranged from 260 to 421. All seven studies pooled in the meta-analysis were cross-sectional in design. Of the seven studies included in the final analysis, three were conducted in Addis Ababa8 29 30 and two were conducted in the Amhara region.31 32 All of these studies were conducted from the year 2016 to 2020. Among the seven studies, four studies provided a clear definition of social support. Two studies described measurements of social support (Oslo-3 social support scale). The quality assessment with Newcastle-Ottawa Scale assessment tool indicated that all studies had a moderate risk of bias, with scores ranging from 7 to 8 and none of the included studies was excluded from the meta-analysis (table 1).
Characteristics of original studies
The effect of social support on depression
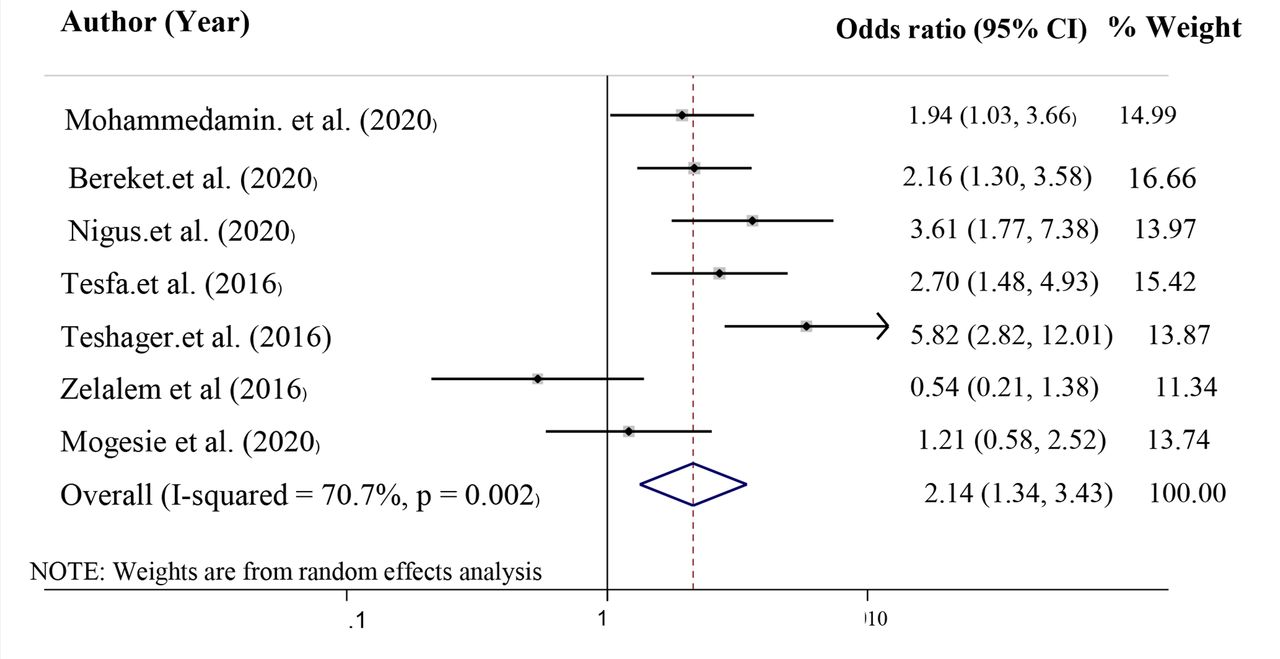
Significantly high heterogeneity was revealed across studies (I2= 72.6%, p = 0.201), which means that using a fixed-effects model would have led to an unreliable estimate. Therefore, we used a random-effects model to estimate the pooled effect of social support on the depression reported by the seven studies with inverse variance. The crude and adjusted ORs for the association between social support and depression were reported by seven studies. The result of this meta-analysis showed that social support had a statistically significant association with depression. The odds of having depression were two times higher among patients who had poor social support compared with patients who had good social support (OR=2.14, 95% CI 1.34 to 3.43, p=0.003) (figure 2).

The pooled OR for the association between social support and depression among patients with diabetes.
Subgroup analysis
To identify the sources of heterogeneity, we performed subgroup analyses based on several important confounding factors. We performed a subgroup analysis based on sample size, the study region of the country, mean age and prevalence of depression. In the stratified analysis by sample size, a significant association was only found among studies that used a large sample size (≥400 samples) (OR= 2.64, 95% CI 1.37 to 5.10), but not among studies that used a small sample size (<400). Similarly, in the stratified analysis by geographic location (region), a significant association was only found among studies done in regions other than Amhara and Addis Ababa (OR= 2.07, 95% CI 1.40 to 3.08), but not in Amhara and Addis Ababa (table 2).
Subgroup analyses for included studies
To detect the studies which influence the overall estimate of our meta-analysis, we also performed sensitivity analysis (online supplemental file 2).
Supplemental material
Publication bias
In this meta-analysis, we checked publication bias using a funnel plot of asymmetry and Egger’s test. We found no evidence of publication bias after using a funnel plot of asymmetry and Egger’s test. For all studies, the funnel plot was symmetrical (figure 3). No publication bias was shown by Egger’s test (p=0.266) or Begg’s test (p=0.453).

{kind=link}
{kind=link}
{kind=link}
The funnel plot for included studies.
Discussion
Although many primary studies have tried to identify the determinants of depression among patients with diabetes, the association between social support and depressive symptoms remains unclear. To fill this information gap, this is the first meta-analysis to assess the association between social support and depression in Ethiopia. This meta-analysis of seven studies, involving 5543 participants, showed a significant association between social support and depression. For patients with diabetes with poor social support, the odds of developing depression were more than double that of participants with good social support. The relationship between social support and depression in our analysis is consistent with the findings of primary studies done in different parts of the world that reported that poor social support is associated with the onset and relapse of depression.33–36 This positive effect of good social support on depression is also consistent with a previous meta-analysis that reported psychosocial interventions reduced depressive symptoms in individuals with diabetes.37 Social support, whether from a trusted group or valued individual, has been shown to reduce the psychological and physiological consequences of stress and may enhance immune function by reassuring the person that help is available and, thus, enhance the individual’s coping abilities in dealing with depression.35 38 39 Social networks, whether formal (such as a church or social club) or informal (meeting with friends) provide a sense of belonging, security and community. In Ethiopia, ‘Iqqub’ and ‘Idir’ are among the most important social and financial institutions that provide a much wider range of services, including financial and material assistance and consolations for a member in the event of difficulties as well as entertainment in the case may be.40 In general, good social support is associated with decreased morbidity and mortality of several chronic illnesses including diabetes. Therefore, these local social networks should be strengthened to reduce the burden of depression among patients with diabetes.
The significant association between social support and depression was still existent in further subgroup analyses stratified by the mean age of participants, which suggests that our findings are relatively stable among the young and older population. However, the effect size (OR) was larger in studies with participants’ mean age ≤45 years compared with mean age >45 years. However, this should be interpreted cautiously because the CI for both effect sizes overlap with each other. In the stratified analysis by sample size, a significant association was only found among studies that used a large sample size (≥400 samples), but not among studies that used a small sample size (<400). To detect the studies which influence the overall estimate of our meta-analysis, we performed a sensitivity analysis. In the sensitivity analysis, no significant change in effect size was reported when excluding any individual study suggesting homogeneity of the pooled effect estimates.
Our analysis adds to the literature by combining and highlighting studies relevant to Ethiopian experiences. Ethiopia has unique spiritual and social structures that have the potential to influence the level of social support for patients with diabetes and their ability to cope up with depression and stress.
This meta-analysis had several limitations. First, our search generated only a modest number of research. Second, our data sources were observational studies, thus restricting our ability to explore fully the influence of unmeasured confounding variables. For example, participants with social support may also have poor adherence to antidiabetic medication and healthy behaviours like physical exercise. Both of these could independently affect the risk of depression. Third, our findings were the pooled effect of many cross-sectional study designs, which are limited in their ability to draw on causal inferences. Finally, and most importantly, the reviewed studies lacked consistent measurement methods and definitions for social support, which may have increased the heterogeneity of our findings.
Conclusion
This meta-analysis has emphasised the important role of social support in reducing depression among patients with diabetes in Ethiopia. We recommend additional investigation of social support and its measurement among patients with diabetes because there is a heterogeneity of social support measurements in the literature. Therefore, in the future, social support framework must be applied to classify social support measurement and to improve the mental health outcomes of patients with diabetes.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @MengistBelayneh
Contributors GD: conception of the research protocol, literature review, data extraction, data analysis, interpretation and drafting of the manuscript. AA and MLE: data analysis and reviewing the manuscript. BM: reviewing the revised manuscript. All authors have read and approved the manuscript. GD acts as guarantor for the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.