Article Text

Abstract
Objective Functional gastrointestinal disorders (FGIDs) are common during childhood and adolescence. When a somatic diagnosis is excluded, the healthcare system often terminates contact with the patient. The aim of the present study was to learn more about children’s and adolescents’ experiences with, and reflections on, the causes of their abdominal pain and what could possibly help them.
Design The study has a qualitative design. Interviews with open questions were carried out by the first author. The conversations were audiotaped, transcribed and analysed by means of qualitative content analysis.
Setting Children and adolescents referred from general practitioners located in urban and rural regions in two municipals in Norway. In 2016 and 2019, we had interviewed these children’s parents about their child’s abdominal pain. In spring 2020, the children and adolescents were interviewed.
Participants Twelve children and adolescents aged 10–18 years with FGIDs.
Results Eight of the children and adolescents had recovered from their abdominal pain, while four still had symptoms. They felt frustrated by not having a diagnosis and by the lack of available treatment. Some who had been absent from school for weeks to months felt isolated and depressed. Focusing on positive thoughts and activities was reported to improve the pain. The abdominal pain could be considered a manifestation of mental problems.
Conclusions Thinking differently about the symptoms reduced the FGIDs for the children and adolescents. The treating physicians as well as parents and teachers need to help the child focus on changing the mindset of pain.
- functional bowel disorders
- paediatric gastroenterology
- child & adolescent psychiatry
- qualitative research
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- functional bowel disorders
- paediatric gastroenterology
- child & adolescent psychiatry
- qualitative research
Strengths and limitations of this study
The first author had interviewed the children’s and adolescents’ parents two times earlier and she, therefore, knew their pain histories.
The first author carried out all the interviews.
The use of semistructured interviews enabled detailed information about the children’s and adolescents’ functional gastrointestinal disorders.
The sample size is small and only children from well-integrated families were interviewed.
Introduction
Functional gastrointestinal disorders (FGIDs) are characterised by pain and chronic or recurrent digestive symptoms without an underlying somatic disease or biochemical abnormality. The Rome criteria have become the standard for defining FGIDs.1 FGID diagnosis in childhood has no biological markers and is based exclusively on symptoms reported by the child and their parents.1 The pioneering paediatrician John Apley wrote in 1958: ‘It is a fallacy that a physical symptom always has a physical cause and needs a physical treatment.2 A study from 2020 of Egyptian children aged 4–18 years reported a prevalence of 30.4% of FGIDs, with irritable bowel syndrome the most common type of FGIDS.3 In 2016, the prevalence of FGIDs among children and adolescents aged 4–18 years in the UK was 23%.4
For a study published in 2018, we interviewed parents of 14 children aged 6–13.5 years with FGIDs.5 These children had been examined in a local hospital and were discharged without a somatic diagnosis. From that study, we concluded that FGIDs in children and adolescents are challenging for both the patient and their family, and that they often need long-term medical support.5 In 2019, we interviewed the same parents again.6 At that time, they continued to express needing a diagnosis and more information from physicians. All parents thought that the abdominal pain had a physiological cause, some parents thought, however, that problems at school or with friends could influence on the abdominal symptoms.5 6 Some confirmed that they had left the conversation with the child about FGIDs to the physician, the psychologist and the teacher, often because they thought it was too difficult for them as parents. The parents also stated that they did not know the reason to the child’s symptoms, but they suspected that it could be allergy or intolerance. The idea that mental problems could influence on the symptoms was seldom discussed with the child.5 6
In clinical work, however, questions about somatic and psychiatric symptoms should also be addressed to the children, as parents and teachers do not always recognise children’s symptoms.7 Thus, the aim of the present study was to learn more about the child’s and adolescent’s own experiences with FGIDs, not only how the pain affected their lives but also how the children and adolescents in retrospect reflected on the power that the pain had over them. To our knowledge, no previous in-person interview study has been conducted with children and adolescents with FGIDs whose parents have been previously interviewed two times about the same subject.
Method
The qualitative study was based on interviews conducted in Norway.
Patient and public involvement
Patients and the public were not involved in any ways.
Participants
In 2016, the first author interviewed 15 parents of 14 children with FGIDs, aged 6–13.5 years.5 The children and adolescents had been referred by their general practitioner (GP) to a city hospital that serves around 500 000 inhabitants. Neither their GPs nor the hospital had found an explanation for these children’s pain. The only exclusion criterion for the study was an inability to communicate in Norwegian. Data saturation was discussed in the article from 2016.5 In 2019, all parents were interviewed again about the current situation for the children and their families.6 Even though 4 years had passed since the children and adolescents were examined in hospital for the first time, the parents’ described that some of the children still suffered from FGIDs.
In spring 2020, the families were contacted by phone, this time, for the purpose of interviewing the children. Among the 14 children whose parents had been interviewed, 12 agreed to participate (6 boys, 6 girls). At that time, the children were 10–18 years old. The two non-responders were a child with other physical challenges and a child who did not want to participate. Further recruitment details have been published previously.5
Interviews
The interviews were carried out by the first author, a female GP and child and adolescent psychiatrist. She presented herself as a researcher with no therapeutic involvement or treatment responsibilities. All interviews were conducted during May and June 2020 as video conferences due to the COVID-19 pandemic. Three children brought their mother to the interview. An interview guide was used and tested in one pilot interview but was not provided to the participants (figure 1). Field noted were made during the interviews. Repeat interviews were not carried out.

Interview guide (children and adolescents). GP, general practitioner.
Both the child/adolescent and their parents received written information about the study. The parents signed and returned the consent form. Participants over age 16 years signed on their own behalves. The audiotaped video conference interviews lasted 25–60 min. The transcripts were not returned to the participants for comments.
Data analysis
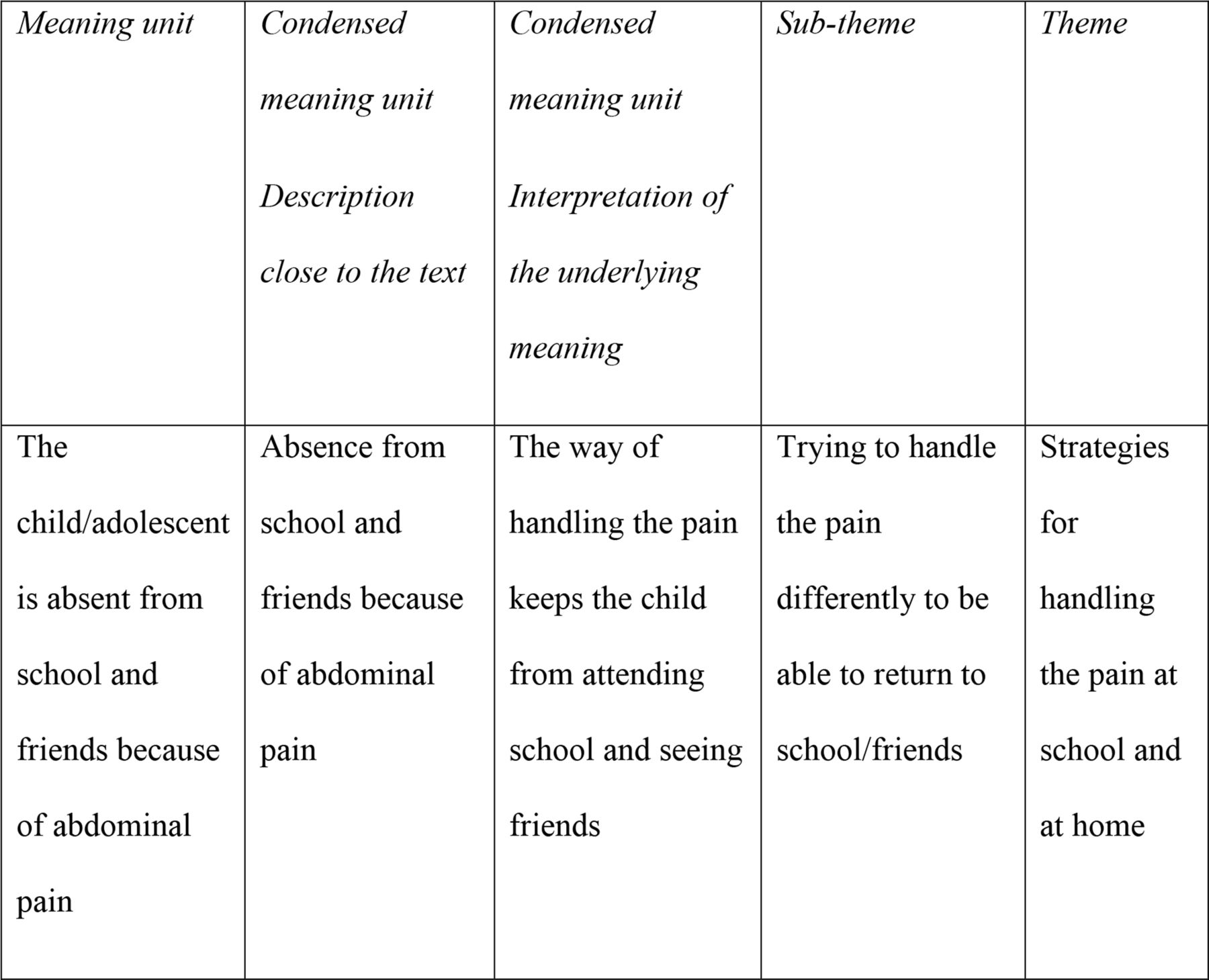
The first author recorded and transcribed the interviews. Both authors read the transcripts individually and collaborated on the analysis. Qualitative content analysis was applied, as described by Graneheim and Lundman.8 Meaning units were found, shortened and coded. The codes were grouped into categories and subcategories to identify three main themes as shown in figure 2. No software tools were used for analyses. The themes were derived from the data, not identified in advance.

{kind=link}
{kind=link}
Examples of codes, condensed meaning units, subthemes and themes.
Reporting of the study follows the Standards for Reporting Qualitative Research9 and includes the Consolidated Criteria for Reporting Qualitative Research checklist (online supplemental appendix 1).
Supplemental material
Results
Twelve children and adolescents aged 10–18 years were interviewed. Nine of the children had Norwegian parents and three had parents of foreign origin who had lived in Norway for several years. Two of the children lived with a stepparent. Eleven children had siblings; eight had one sibling, two had two siblings and one had three half siblings.
At the time of the interviews, eight children (four boys and four girls) had recovered from their abdominal pain; four (two boys and two girls) had improved symptoms. We also know—from our interviews with their parents—that the two non-participating children had recovered from their FGIDs.
We identified three main themes in the current interviews with the children and adolescents:
Feeling isolated and depressed.
Strategies for handling the abdominal pain at school and at home.
The need for a diagnosis and information.
Theme 1: feeling isolated and depressed
The pain prevented most of the children and adolescents from being social and participating in leisure activities. They reported that the pain controlled their lives in many ways. Some had told their friends about the FGIDs and that it could be difficult for them to go to school or participate in other activities. However, others did not want to inform their school or friends about the FGIDs because it made them different from other children. Consequently, they tried to hide their symptoms: I want to be like everyone else and not pay attention to the stomach pain (interview number 8).
Being dependent on having a toilet nearby could also be embarrassing for the children and restricted them from school or other activities, which in turn aggravated the situation. They felt isolated and the situation affected their mental state. These children and adolescents reported mental symptoms ranging from feeling sad to being deeply depressed and needing psychological treatment. The fact that the FGIDs hindered them from doing positive activities worsened their mental state: I love playing basketball, the fact that the stomach pain has stopped me from playing during long periods made me deeply depressed (interview number 6).
The FGIDs could cause major consequences for the whole family, such as work absence, economic impacts and worried siblings. The children reported having a bad conscience, feeling guilty and ashamed of their family’s difficult situation. This became another burden, in addition to the FGIDs and absence from school and social life, which further reduced their mental state.
Some of the adolescents reported seeing the abdominal pain as a manifestation of mental problems. Reaching this insight had been time-consuming and required professional assistance but was described as a sort of revelation leading to a new understanding of a complicated problem.
Some reported escaping from their mental problems by using somatic symptoms. The youngest children in the study also seemed to be aware of this phenomenon: The stomach pain came in the evening or in the morning on days when I should do something difficult at school (interview number 7).
Theme 2: strategies for handling abdominal pain at school and at home
Nearly all the interviewed children had experienced FGIDs both at home and at school. The frequency and intensity of their pain differed markedly, independent of where they were. School absence affected both their academic situation and daily contact with friends. The FGIDs made it difficult to concentrate on schoolwork. Three of them (two boys and a girl) missed several weeks of school, while four always remained at school despite their stomach pain. Two adolescents reported that their teachers were unaware of their FGIDs and how it affected them: I had a lot of absence from school. I do not think the teachers knew much about the pain. I had to explain to the teacher myself each time (interview number 9).
In some cases, the parents had informed their child’s school about the FGIDs and had made arrangements, so that it was easier for the child to stay at school during pain episodes: We had arranged with school that I could sit in another room and read when I had stomach pain. Therefore, I never left school because of stomach pain (interview number 1).
The children reported both that they thought they experienced FGIDs because they did not like school, and, the opposite, that they missed going to school when they stayed home because of pain. Some reported having used the FGIDs to convince their parents that they needed to stay home from school: If I wanted to stay home from school the next day, I asked for some food that gave me stomach pain (interview number 3).
The children had different ways of handling their pain at home. It could be reduced or worsened by food or drinks like milk, wheat products and vegetables. Others reported positive effects of a warm bath, lying down on the floor to relax or going to the toilet. Eight children had taken analgesics, with varying effects. Two reported that medicine reduced their FGIDs, while six were unsure. Some of the children reported handling their FGIDs by shifting their focus from the pain to a positive activity, such as football, gaming, etc. Some children had discussed these methods with their parents or a psychologist, while others experimented on their own: The pain was reduced when I distracted myself. When I played football, I never noticed the pain. I was so set on playing (interview number 1); When I was gaming with my friends, I stopped thinking about the stomach pain (interview number 6).
Even the younger children reported that thinking about their pain made it worse: I thought hurts, hurts, hurts and then the pain became worse. Then I did something I liked to do, and the pain disappeared (interview number 9).
However, they also reported that there often was nothing to do but wait until the pain disappeared. No medicine or other treatments were available at school; therefore, it was better to go home: I usually call my mother, who picks me up and we go home (interview number 7).
Based on the information provided by the children, parental involvement and interventions varied. Few had the impression that they had discussed the pain with their parents. However, many said there was not much the parents could do because nothing helped their FGIDs.
None of the children in our study had involved their siblings in their FGIDs. Nor had they thought much about the fact that their symptoms could have a marked effect on their siblings.
Theme 3: the need for a diagnosis and information
These children and adolescents were clear in their expressions that they needed to know what was wrong with their stomach. They reported that uncertainty about their diagnosis made the situation worse. It was difficult for them to understand that there was no medicine or treatment to reduce or remove the pain and provide a more predictable daily life. During pain periods, they never knew how the day would go or whether they would be able to participate in various activities. Some were afraid of having a serious disease, which they feared further examinations would reveal. Some shared these thoughts with their parents, while others kept them to themselves.
Some children even asked questions of the interviewer because they did not know who else they could talk to, except for their parents: There was a girl at school who had cancer. I thought that I also could have something similar. I did not know who I could ask about this (interview number 6).
These children and adolescents emphasised that information concerning their symptoms and diagnosis from physicians was important. They felt they had been well cared for in the hospital, even if some missed out on receiving information because it was not communicated on their level. When the FGID diagnosis and other information were conveyed to the child in a way they understood, this positively affected their abdominal pain: When they found out what this pain was, I started to feel better at once and the pain disappeared gradually (interview number 12).
Some parents tried to explain and discuss the FGIDs with the children. However, direct psychoeducation from the doctor was important to the children and could change their situation. Explanations that these symptoms were not dangerous, that the pain would be reduced over time and that it was important to go to school improved their situation. Drawings of the intestinal tract, stool quality, etc were remembered by the youngest children and helped them understand more of their symptoms: I asked the doctor. She said she thought the pain would gradually be reduced and disappear. That helped me a lot. Until then, I had thought the pain always would be there (interview number 1).
Three of the children had talked to a child and adolescent psychologist, another had requested an appointment, but this request was not fulfilled. Two children sought guidance from a family member with psychological expertise.
Discussion
Twelve children and adolescents with FGIDs were interviewed, after their parents had been interviewed in 2016 and again in 2019. Eight of the children had recovered from the FGIDs and four had reduced symptoms. Three of the adolescents had weeks or months of school absence. We noted that all children were concerned about keeping in contact with friends and being able to continue sport activities and hobbies. They underlined that focusing on something positive could reduce the pain. Their FGIDs could also hide other difficulties, such as psychological problems, which manifested as pain. Information and psychoeducation from their physicians were important to these study participants.
Theme 1: feeling isolated and depressed
Many of these participants reported feeling lonely, socially isolated and sad; some even reported deep depression. Research supports the concept that recurrent and persistent abdominal pain can be a prodrome of depression and anxiety, or vice versa, in young people.2 7 10 It is also well known that loss of pleasure, changes in life and stressful life events are factors that may lead to depression or other psychiatric symptoms. We could not determine whether our participants’ psychosocial issues preceded their somatic complaints or resulted from them. The biopsychosocial model of illness is based on this complex interplay of genetic, environmental, physiological and psychological factors and their influence on symptoms.1 11
Consistent with other studies, it is safe to assert that adolescent patients with chronic somatic reports are more likely to experience significant anxiety, depression and psychosocial or environmental stressors.12 Some of the children and adolescents in our study expressed a deep sense of despair and hopelessness, which may lead to serious and long-lasting problems. Physicians should, therefore, be careful to investigate these symptoms.12
Besides having FGIDs, we found that these children felt ashamed of not being in school and guilty about their parents’ missing work. Some of these children kept such feelings to themselves because they thought they were too embarrassing to talk about. According to studies by Khan, it is important to identify emotional or psychological stressors to help both the child and their parents understand the child’s reactions and feelings and to support the child in this process.13 In our experience, openness about such issues with school, friends, etc often improves the child’s situation.
It has been emphasised that the goal of managing FGIDs is to provide a satisfactory quality of life through support, education, medications, and better coping skills. Reassurance about the positive outcomes of FGIDs and positive aspects of the child’s health are crucial.13
Theme 2: strategies for handling the abdominal pain at school and at home
Providing the child and their parents with information about the importance of trying to attend school, even on days when the child has abdominal pain, is a prominent part of treatment for FGIDs.14 15 Being at home instead of at school or work may seem like the easiest solution; three of the adolescents in our study had months of school absence. Some of the youngest children in our study reported calling their parents and being brought home when their FGIDs increased at school. Our study illustrates that it is difficult for parents to refuse to pick their child up from school during pain periods. As stated by Lowth, the child should not associate pain with removal from normal activities but should understand the importance of maintaining routines and staying at school during pain periods.14 Others have emphasised that teachers need reassurance and information that the abdominal pain is functional, while acknowledging that it is genuine. The advice is clear: pain during class should be managed through continuation of the usual routine.16
Parents’ reaction to their child’s pain is increasingly recognised as an important moderator of the child’s outcomes and has become an area for clinical intervention.17 According to van Tilburgh, a supportive and understanding home environment is important for helping the child recover from pain. Parents look to clinicians for help and are open to discussing both medical and behavioural approaches to their child’s pain. Their role may be difficult, and they also need physician support.18 Some children and adolescents in our study had talked to their parents about their FGIDs, but most reported not having helpful conversations about hope for recovery. The fact that all parents stated that the pain mainly had physiological causes gave the children little support in the belief that it also could have mental causes.5 6 Parents should be advised to reduce concerned responses to their child’s pain and to focus on distraction instead.19 Lowth stated that the most important therapeutic steps are to explain the diagnosis, develop strategies to cope with stress and provide reassurance that there is no serious underlying disease.14 Others have described that the parents’ acceptance of a biopsychosocial model of illness is important to the resolution of FGIDs in children.16 20
The children in our study had not involved their siblings in their FGIDs and did not think it was important to do so. Similarly, Gan found that many siblings were overlooked, and that they experienced difficulties with schoolwork, decreased school attendance, academic dysfunction and perceived differences in peer and teacher interactions. A school-based sibling support model combining sibling and teacher, psychoeducation and individualised psychological support has been suggested, in which parents and schools are advised to normalise the siblings’ experience and reaction, with consistent support.21
The children and adolescents in our study who had been referred to a child and adolescent psychologist or psychiatrist reported positive experiences. Other studies have found that various psychological therapies reduce pain. Cognitive behavioural therapy has effectively reduced the recurrent abdominal and other types of pain.19 22 Other methods like relaxation exercises and hypnosis have also been tried.13 The current focus is increasingly on pain-specific cognitions and coping strategies, including disease threat and catastrophising.23
Theme 3: the need for a diagnosis and information
A study from 2018 stated that the most important step in treating FGIDs is a correct diagnosis.24 The participants in our study also emphasised that diagnosis and information about the disease are crucial to improving their situation. One challenge with this diagnosis is helping patients understand that even if there is no underlying organic disease, FGIDs cause symptoms such as abdominal pain. One study noted that children need medical treatment to relieve their symptoms, even if there is no organic cause for them.24 In a study among children with functional nausea and their mothers, they also expressed the desire for a clear medical diagnosis and treatment and recognised the significant impact of the symptoms on the adolescents’ mental health and social functioning.25 A Canadian study from 2013 also emphasised that uncertainty about the diagnosis was difficult for families where a child suffered from FGIDs.26
The importance of children’s needs and rights to information about their diseases and symptoms are manifested in the United Nations Convention on the Rights of the Child from 1989, in which article 24 ‘Health and Health Services’ describes children’s and adolescents’ right to.27
Information dissemination has been discussed elsewhere. Damm stated that effective communication skills are important when assessing and treating a child’s subjective pain symptoms. Without the child’s contributions to the conversation, understanding the nature and severity of their pain is difficult.28 We found that the patients’ understanding and acceptance of information about their symptoms is crucial to their treatment course. Physicians’ reassurance that their young patients have understood the information they provided is also important. Street stated the importance of physicians providing both qualitative and quantitative information.29 This was underlined by an adolescent in our study who reported that from nearly the first moment when his physician explained that his pain was not serious, it decreased and gradually disappeared. This also coincides with other researchers’ report that communication is the most common and essential medical ‘procedure’30 and that, furthermore, effective and adapted communication is essential for accurate diagnosis, successful treatment and enhanced patient satisfaction.31
Strengths and limitations
The interviewer is herself a GP and child and adolescent psychiatrist and has long experience conversing with children and adolescents. She introduced herself as a researcher without clinical responsibility for the interview subjects’ symptoms. Due to the COVID-19 pandemic, the interviews were conducted as video conferences. This could reduce spontaneous statements and non-verbal communication, however, is could make it easier for the children and adolescents to provide sensible information. The children and adolescents had been examined in hospital 4 years before the interviews. We think that they could have forgotten some details about their FGIDs, but the retrospective view of the situation gave valuable considerations and reflexions about their FGIDs and what had reduced the symptoms. Three of the youngest children sat together with their mothers during the interview, which could influence some of the answers, especially the questions about the parents’ involvement in the pain situation. However, the presence of the mothers seemed to make these children less nervous and more relaxed in the interview. The analysis could have been affected by the fact that we knew from our two earlier studies that the parents thought the symptoms were mainly a physical condition.
Conclusion
FGID in children and adolescents is a complex disorder that affects their home, school and friend situations. These children often feel isolated, sad and depressed, and they need more information and better explanations about their symptoms. Treating physicians, schools and parents must all be familiar with the child’s situation. Treatment should include adapted psychoeducation, referral to a child and adolescent psychologist may also be necessary.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Acknowledgments
We are grateful to all children and adolescents who participated, and to their parents, for sharing their experiences with us.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Both authors meet the ICMJE criteria for authorship. The paper was conceived by AB and MB. MB applied for ethics approval. AB carried out the interviews and transcribed the text, and both authors participated in the analysis. AB drafted the article, and MB revised it critically.
Funding This study was supported by a grant from The Norwegian Committee on Research in General Practice (grant number N/A). The funders were not involved in the study design, analysis, interpretation of data, the writing process or the decision to submit the manuscript for publication.
Competing interests None declared.
Ethical approval The Norwegian Regional Committee for Medical and Health Research Ethics—REC South-East C—approved the study (reference number 2020/93964). The study followed the operational principles of the Declaration of Helsinki and adhered to the Belmont Report principles (ie, respect for persons, beneficence, justice) in obtaining valid informed consent from parents. Parents gave written consent to participate. Children and adolescents were informed about the study through an information letter. Children 16 years and older signed their own consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.