Article Text

Abstract
Introduction The oligometastatic (OM) disease hypothesis of an intermediate metastatic state with limited distant disease deposits amenable for curative therapies remains debatable. Over a third of prostate cancer (PCa) patients treated with radical prostatectomy and postoperative radiotherapy experience disease recurrence; these patients are considered incurable by current standards. Often the recurrence cannot be localised by conventional imaging (CT and bone scan). Combined anatomical imaging with CT and/or MR with positron emission tomography (PET) using a novel second-generation prostate-specific membrane antigen (PSMA) probe, [18F]DCFPyL, is a promising imaging modality to unveil disease deposits in these patients. A new and earlier molecularly defined oligorecurrent (OR) state may be amenable to focal-targeted ablative curative-intent therapies, such as stereotactic ablative radiotherapy (SABR) or surgery, thereby significantly delaying or completely avoiding the need for palliative therapies in men with recurrent PCa after maximal local treatments.
Methods and analysis This ongoing single-institution phase II study will enrol up to 75 patients total, to include up to 37 patients with response-evaluable disease, who have rising prostate-specific antigen (range 0.4–3.0 ng/mL) following maximal local therapies with no evidence of disease on conventional imaging. These patients will undergo [18F]DCFPyL PET-MR/CT imaging to detect disease deposits, which will then be treated with SABR or surgery. The primary endpoints are performance of [18F]DCFPyL PET-MR/CT, and treatment response rates following SABR or surgery. Demographics and disease characteristics will be summarised and analysed descriptively. Response rates will be described with waterfall plots and proportions.
Ethics and dissemination Ethics approval was obtained from the institutional Research Ethics Board. All patients will provide written informed consent. [18F]DCFPyL has approval from Health Canada. The results of the study will be disseminated by the principal investigator. Patients will not be identifiable as individuals in any publication or presentation of this study.
Trial registration numbers NCT03160794
- radiation oncology
- radiation oncology
- radiology & imaging
- prostate disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study focuses on a subset of prostate cancer patients for whom no curative treatment options exist.
This study assesses both a diagnostic and a therapeutic intervention in biochemically recurrent prostate cancer: [18F]DCFPyL positron emission tomography-MR/CT, and prostate-specific membrane antigen-directed ablative therapy.
This study allows for either surgery or stereotactic ablative radiotherapy for treatment of prostate cancer oligometastases.
This study utilises a small sample size, however this is the a priori determined sample size based on estimated effect size.
Introduction
Prostate cancer (PCa) is the most frequent non-skin malignancy, and is one of the leading cancer-related causes of death in men.1 2 For patients with adverse pathological features or rising prostate-specific antigen (PSA) after radical prostatectomy (RadP), postoperative radiotherapy (PORT) either as adjuvant or salvage treatment, respectively, have been shown to be beneficial.3–5 At present, a significant proportion of patients (30%–60%) recur despite maximal local therapies (RadP plus PORT),6–8 most likely due to subclinical distant metastases developed prior to and/or during local treatments.
Oligometastatic (OM) disease, referring to a disease state where cancer has spread beyond the site of origin but is still confined to a limited number (eg, 5 or less) of metastatic disease deposits, is an increasingly accepted concept in oncology. Emerging evidence has shown that the addition of focal ablation of OM disease deposits to systemic therapies prolongs survival.9 10 However, rendering cure remains an elusive goal of the OM state hypothesis. In PCa, existing evidence supports the concept that decreased burden of disease predicts improved response to hormonal therapies and longer survival.11 Additionally, phylogenetic analyses have shown that metastatic deposits can be the source of further disease spread,12 and therefore their eradication could potentially cure the disease, or delay the emergence of lethal/castrate-resistant clones.13 There is also emerging evidence suggesting benefit from intensified targeted focal ablative therapies to limited sites of metastatic disease11 14–19 to delay the initiation of non-curative androgen deprivation therapy (ADT). The treatment modalities used for OM disease deposits are either surgery or stereotactic ablative radiotherapy (SABR), an advanced technique that delivers highly conformal and large doses of radiation over few (eg, 1–5) treatment sessions, with very high rates of local control and low rates of toxicity.14 20However, no prospective study has a priori defined a scenario following exhausting the available curative-intent therapies, to primarily evaluate if patients with OM PCa can be rendered into a state of ‘no evidence of disease’ with ablative therapies, which is a necessary step towards achieving cure.
A key component of the OM disease definition is the existence of biomarkers that can detect small amounts of residual disease, coupled with effective imaging to localise the disease deposits at the earliest stages of spread. In PCa, such a biomarker exists (eg, PSA), and combination whole body MR techniques with molecular positron emission tomography (PET) imaging are highly promising for improved disease detection and localisation.21 22In addition, molecular imaging has reliably been shown to unveil distant disease not identified by conventional imaging (CT and bone scans).23 24 Studies have consistently suggested that prostate-specific membrane antigen (PSMA)-based probes are superior to choline-based PET probes in characterising distant disease, primarily in the post-prostatectomy setting.25 26 Importantly, PET-identified lesions were true positives in all cases with histologic confirmations.26 Recently, a second generation PSMA-targeted probe, [18F]DCFPyL, has been developed, and clinically tested with encouraging preliminary results, with increased sensitivity and better image definition than first generation PSMA probes.27 Although not yet validated for emerging PET/MR technology, improved lesion detection and definition has been shown for fused PET/CT compared with either modality alone,28 which is particularly relevant for detection, localisation and targeting of small, early lesions. Integrated PET-MR/CT with the PSMA probe is a promising imaging modality to enable the detection of early OM disease, to subsequently test the clinical value of curative-intent ablative treatments.
Currently, patients with recurrent disease following maximal local treatment (RadP and PORT) have no curative treatment options. We hypothesise that [18F]DCFPyL PSMA-targeted PET-MR/CT allows earlier detection and localisation of metastatic disease, and identifies a new molecularly defined OM state amenable to curative-intent SABR.
Methods and analysis
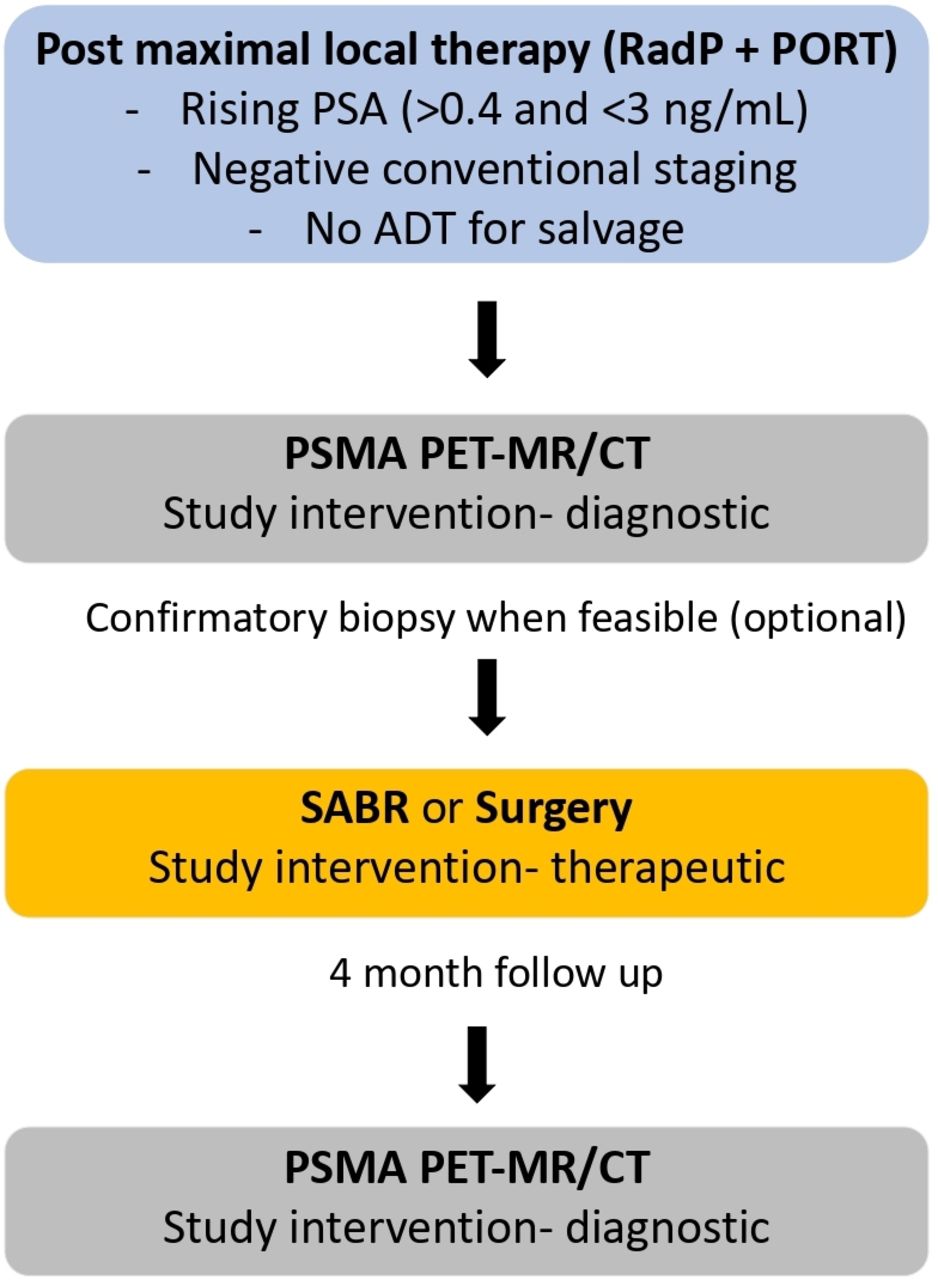
Eligible patients will include men who have had maximal local therapy (RadP and PORT) with rising PSA level between 0.4 and 3.0 ng/mL, negative conventional staging (CT and bone scan), and no prior use of ADT for salvage. All patients will undergo [18F]DCFPyL PET-MR/CT scans, with optional confirmatory biopsies if feasible to allow for pathologic and radiographic correlation. Patients with disease detected on PET-MR/CT that is deemed amenable to radical approaches will be treated with SABR or surgery (with no maximum number of lesions defined a priori to disqualify metastasis-directed treatment). All treated patients will undergo a follow-up [18F]DCFPyL PET-MR/CT 4 months following treatment (figure 1). PSA will be measured for assessment of biochemical response (none, partial or complete defined as <50%, ≥50% or 100% PSA decrease from pre-ablative therapy levels, respectively).

{kind=link}
Study schema. ADT, androgen deprivation therapy; PET, positron emission tomography; PSA, prostate specific antigen; PSMA, prostate-specific membrane antigen; PORT, post-operative radiotherapy; RadP, radical prostatectomy; SABR, stereotactic ablative radiotherapy.
Objectives
The study has two main objectives. The first is to determine if [18F]DCFPyL PET-MR/CT can identify early OM disease in patients with a rising PSA after standard-of-care maximal local therapies. The second is to determine if treating PET-MR/CT identified lesions with SABR or surgery is associated with favourable preliminary measures of clinical performance.
Endpoints
Detection rates and performance metrics of [18F]DCFPyL PET-MR/CT in the post prostatectomy and PORT setting.
Detection rate is defined as number of patients with positive [18F]DCFPyL PET-MR/CT (any PSMA uptake on either PET-MR or PET-CT) divided by the total number of patients who undergo [18F]DCFPyL PET-MR/CT imaging.
Proportion of patients achieving biochemical response.
Complete response is defined as an undetectable PSA (<0.05 ng/mL) in two consecutive measurements (at least 2 weeks apart).
Partial response is achieved if a patient has >50% PSA decline in two separate measurements (at least 1 month apart).
Metabolic [18F]DCFPyL response rate 4 months after ablation.
Treatment-related toxicities incidence as defined by the National Cancer Institute Common Toxicity Criteria for Adverse Events version 4 (CTCAE V.4.0).
Time to initiation of salvage ADT after SABR.
Inclusion criteria: (all criteria must be met)
Age>18 years.
Eastern Cooperative Oncology Group performance status 0–2.
Histological evidence of prostate adenocarcinoma on previous radical prostatectomy.
History of PORT, either adjuvant or salvage, without or with concomitant/adjuvant ADT. In case of the latter, at least 12 months after completion of combined modality treatment (eg, PORT with ADT) elapsed.
Three documented PSA rises, at least 1 month apart.
PSA value >0.4 ng/mL and ≤3 ng/mL within 4 weeks of enrolment.
Normal serum testosterone level ascertained within 4 weeks of enrolment.
Absence of metastatic disease: radiological studies (CT abdomen and pelvis, and bone scan) without evidence of regional or distant metastases within previous 4 months.
Exclusion criteria: (any single of these will render patient ineligible)
Significant comorbidities rendering patient not suitable for curative ablative approaches.
Prior history of non-skin malignancy, unless treated curatively and deemed without evidence of disease for at least 5 years.
Contraindications to MRI.
Unable to lie supine for at least 60 min to comply with imaging and treatment.
Impaired renal function (calculated GFR ≤30 mL/min).
Sickle cell disease or other haemoglobinopathies contraindicating the use of [18F]DCFPyL.
Prior use of any form of ADT for salvage.
Interventions
This is an ongoing single institution Canadian study at an academic hospital. All patients will undergo PET-MR/CT scan within 6 weeks of registration. Results will be reported to the treating physician and patient (non-blinded). Treatment recommendations will consist of surgery or SABR or no ablative therapy (if lesions are not amenable) at the physician and patient’s discretion and with multidisciplinary tumour board discussion (non-blinded and non-randomised). For the former, selective or extended nodal dissection is left to the treating surgeon’s discretion. For the latter, the prescription dose will be 30 Gy in three fractions to all lesions, or 27 Gy in three fractions in order to meet organs at risk dose constraints. The dose scheme is in keeping with the one used for concomitant treatment of multiple metastases in ongoing studies at the time of trial conception (NRG-BR001- clinicaltrials.gov NCT02206334). Intensity-modulated radiation therapy or volumetric modulated arc therapy and daily image guidance (MR or cone beam CT) will be the preferred radiation delivery technique as per current institutional practice for OM ablation. Treatment planning will be done using CT simulation (PET/CT simulation will be acceptable). Immobilisation will be as per disease location and site-specific protocols.
For radiotherapy planning to any site, the gross tumour volume (GTV) will be defined as all visible gross disease based on morphologic imaging (MR/CT). PET information could be used for further delineation of the GTV at the discretion of the treating physician. No additional margin is mandated to be added to the GTV for microscopic spread of disease (ie, clinical target volume (CTV) is equal to GTV), but a 3-mm expansion on the GTV for the CTV is allowed at the discretion of the treating physician. CTV for lymph nodes will be defined as the entire involved lymph node. Regional or elective nodal irradiation are not allowed in the trial. A planning target volume (PTV) will consist of an expansion of the GTV/CTV of 8–12 mm in the craniocaudal direction and 5–10 mm in all other directions. Dose will be prescribed to the isodose encompassing 95% of the PTV, commonly within 60%–90% isodose line, to ensure adequate coverage, rapid fall-off outside target and avoidance of extreme hotspots. For treatment to multiple (>1) lesions, a composite plan will be obtained for normal tissue dose evaluation. All plans must be peer-reviewed as per institutional practice.
Follow-up
Patients will be assessed post surgery or during SABR treatments as per standard practices. Patients will be assessed in follow-up at 2 weeks, 1, 2, 3 and 6 months following surgery/SABR (table 1). Each follow-up will include history, physical examination, PSA and total testosterone measurements, CTCAE V.4.0 toxicity assessment and grading, and optional research blood and urine biomarker study samples collection. All patients will undergo follow-up [18F]DCFPyL PET-MR/CT 4 months following ablation. Additional follow-up visits and/or staging investigations can be scheduled at the discretion of the treating physician.
Schedule of enrolment, interventions and assessments
Statistical analysis
Sample size
Two primary study endpoints will both be evaluated in this trial, with initial design based on the therapeutic component of it. This study will employ a phase II non-randomised clinical trial design with a Simon’s statistical design.29 In stage 1 of accrual, 12 response-evaluable patients (defined as patients with OM disease detected on [18F]DCFPyL PET-MR/CT) will be enrolled in the therapeutic component of the study (therapeutic endpoint 2: proportion of patients achieving biochemical response). The null (H0 <5%) and alternate (Ha >20%) treatment-response hypothesis rates were reasoned as clinically meaningful and sufficient to guide decisions to pursue (or not) subsequent studies. Based on alpha and beta set at 0.1, the probability of rejecting the null hypothesis when it is true is 10%, and the power to detect a response rate of 20% or higher is 90%. Therefore, the expected sample size with this design is 12 patients when the null hypothesis is true, and 37 patients when the alternative hypothesis is true. In other words, the intervention (ablative therapy) will be rejected at the end of the stage 1 of accrual if no responses are seen, and the study will be stopped. Otherwise, an additional 25 response-evaluable patients will be accrued. Accrual will be completed when either 37 patients have been treated with ablation (SABR or surgery), or 75 patients have been accrued to the study, whichever occurs first. The investigational treatment approach will be deemed effective if four or more objective responses are observed.
The literature on [18F]DCFPyL PET-MR/CT in detecting disease in the setting of a rising PSA post-maximal local therapies with negative conventional imaging is limited. Therefore, at time of trial conception, we cannot accurately calculate the number of patients who need to be scanned (diagnostic endpoint 1: detection rates and performance metrics of [18F]DCFPyL PET-MR/CT in the post-prostatectomy and PORT setting) in order to detect those with positive findings that are amenable to curative-intent ablative therapies. We conservatively estimate a 50% detection rate based on prior studies using PET/CT and less sensitive imaging probes in a clinically similar scenario.30 Thus, given the maximum sample size for the therapeutic endpoint is 37 patients, up to 75 patients will be scanned. The trial will be stopped once 75 patients have been accrued to the study (or when 37 patients have been treated with ablation, whichever comes first). If the detection rate is lower than 50% with [18F]DCFPyL PET-MR/CT, then the clinical feasibility and utility will be questionable.
Data analysis
Demographics and disease characteristics will be summarised and analysed descriptively. Response rates will be described with waterfall plots and proportions. Additionally, biochemical relapse-free survival will be calculated using the Kaplan-Meier method. Delay to salvage ADT will be estimated based on the time interval from intervention to PSA returning to baseline values, including ascertainment of doubling times pre-ablation and post-ablation. Cox multivariable regression analyses will be used to determine baseline factors predictive of biochemical response and assessment of time to failure data. We used the Standard Protocol Items: Recommendations for Interventional Trials checklist when writing our report.31
Patient and public involvement
No patient or patient advisor was involved with study design, recruitment or conduct.
Ethics and dissemination
Ethics approval
The study received ethics approval from the Princess Margaret Cancer Centre Research Ethics Board (REB #16–5532), all patients provided written informed consent (online supplementary appendix 1) with a clinical research data and regulatory coordinator and had the option to provide written informed consent for optional tests (research blood and urine biomarker study samples and biopsies) (online supplementary appendix 2), and the PSMA-targeted probe ([18F]DCFPyL) has approval from Health Canada. The WHO Trial Registration Data Set is in online supplementary appendix 3.
Supplemental material
Supplemental material
Supplemental material
Subject discontinuation/withdrawal
Subjects may voluntarily discontinue participation in the study at any time. If a subject withdraws from the study, the clinical and laboratory evaluations (including optional blood, urine and tissue) collected before withdrawal will be retained; no new information will be collected without subject consent. If a subject is removed because of an adverse event, they should remain under medical observation as long as deemed appropriate by the treating physician.
Confidentiality
The names and personal information of study participants will be held in strict confidence. In all research records, subjects enrolled will be assigned a code to maintain confidentiality. The code will include the study enrollment number. The link of the study number and identifiable information will be stored in a separate password-protected file within University Health Network (UHN) network. All research data will be protected under secure password, or kept under lock and key in the research office. No records bearing patient identification will be provided to anyone outside of the institution except regulatory agencies. Patients will not be identifiable as individuals in any publication or presentation of this study. Study data will be destroyed 25 years after study completion. Blood, urine and tissue samples will be stored at UHN. The principal investigator will have access to the final trial data set.
Data safety and monitoring
The principal investigator will assume responsibility for monitoring the progress of the trial and the safety of participants. This trial may be monitored on a random basis by the staff of the data safety and monitoring committee, and audited by the Research Ethics Board (REB) or regulatory inspectors, all of which will be permitted and facilitated by the investigator. The investigator will grant the host institution’s REB and safety and monitoring committee full attributions to stop the study if deemed necessary by their operational procedures. Data will also be submitted to the UHN REB annually for continuing review and at the completion of the study.
Protocol amendments and trial publication
Any modifications to the trial protocol must be approved and enacted by the principal investigator (current version: 1.0 amendment 4 on 16 August 2019). Protocol amendments will be communicated to all participating investigators, REB and trial registries by the principal investigator. Any communication or publication of trial results will be led by the principal investigator. Professional writers will not be used for either abstract or manuscript preparation.
Discussion
The current treatment of patients with rising PSA in the setting of postmaximal local therapies (eg, RadP and PORT) and negative conventional imaging investigations is non-curative, consisting of palliative hormonal and chemotherapy treatments. This study is rooted in the principle of ‘imaging with a therapeutic drive’: assessing a novel imaging modality and molecular tracer to unveil and localise OR PCa amenable to curative-intent ablative therapy. This two-stage phase II study will allow for an assessment of the accuracy of [18F]DCFPyL PET-MR/CT in detecting and localising otherwise occult disease and the quantification of the response of ablative treatments (surgery or SABR) to molecularly defined OM PCa disease deposits. Data from this study will contribute evidence towards the ongoing debate of the existence of a curable OM PCa state, and will inform the design of subsequent studies to expand the therapeutic armamentarium for men with recurrent PCa despite maximal local therapies.
References
Footnotes
Twitter @r_glicksman, @aleberlin2
Contributors Initial draft of the protocol and critical review of the manuscript: RMG, UR, JV, PWC, NEF, RGB, DG, AF, RH, TS, DH, CC, MG, PW, AB, SB, DV, DAJ and AB. Initial draft of the manuscript: RMG and AB. All authors read and approved the final manuscript.
Funding This work was supported by: (1) Terry Fox Canadian Comprehensive Cancer Centre Network (TF4CN) Pilot Project, Terry Fox Research Institute (TFRI); (2) Abbvie CARO Uro-Oncologic Radiation Awards (ACURA); (3) Astellas Prostate Cancer Innovation Fund, University of Toronto and (4) The Princess Margaret Cancer Foundation. The funding bodies have no role in study design, collection, management, analysis, interpretation of data, writing the manuscript or decision to submit the report for publication.
Competing interests UM declares a competing interest with Point Biopharm Inc. as a consultant.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.