Article Text

Abstract
Objectives A post hoc gender comparison of transfusion-related modifiable risk factors among patients undergoing elective surgery.
Settings 23 Austrian centres randomly selected and stratified by region and level of care.
Participants We consecutively enrolled in total 6530 patients (3465 women and 3065 men); 1491 underwent coronary artery bypass graft (CABG) surgery, 2570 primary unilateral total hip replacement (THR) and 2469 primary unilateral total knee replacement (TKR).
Main outcome measures Primary outcome measures were the number of allogeneic and autologous red blood cell (RBC) units transfused (postoperative day 5 included) and differences in intraoperative and postoperative transfusion rate between men and women. Secondary outcomes included perioperative blood loss in transfused and non-transfused patients, volume of RBCs transfused, perioperative haemoglobin values and circulating red blood volume on postoperative day 5.
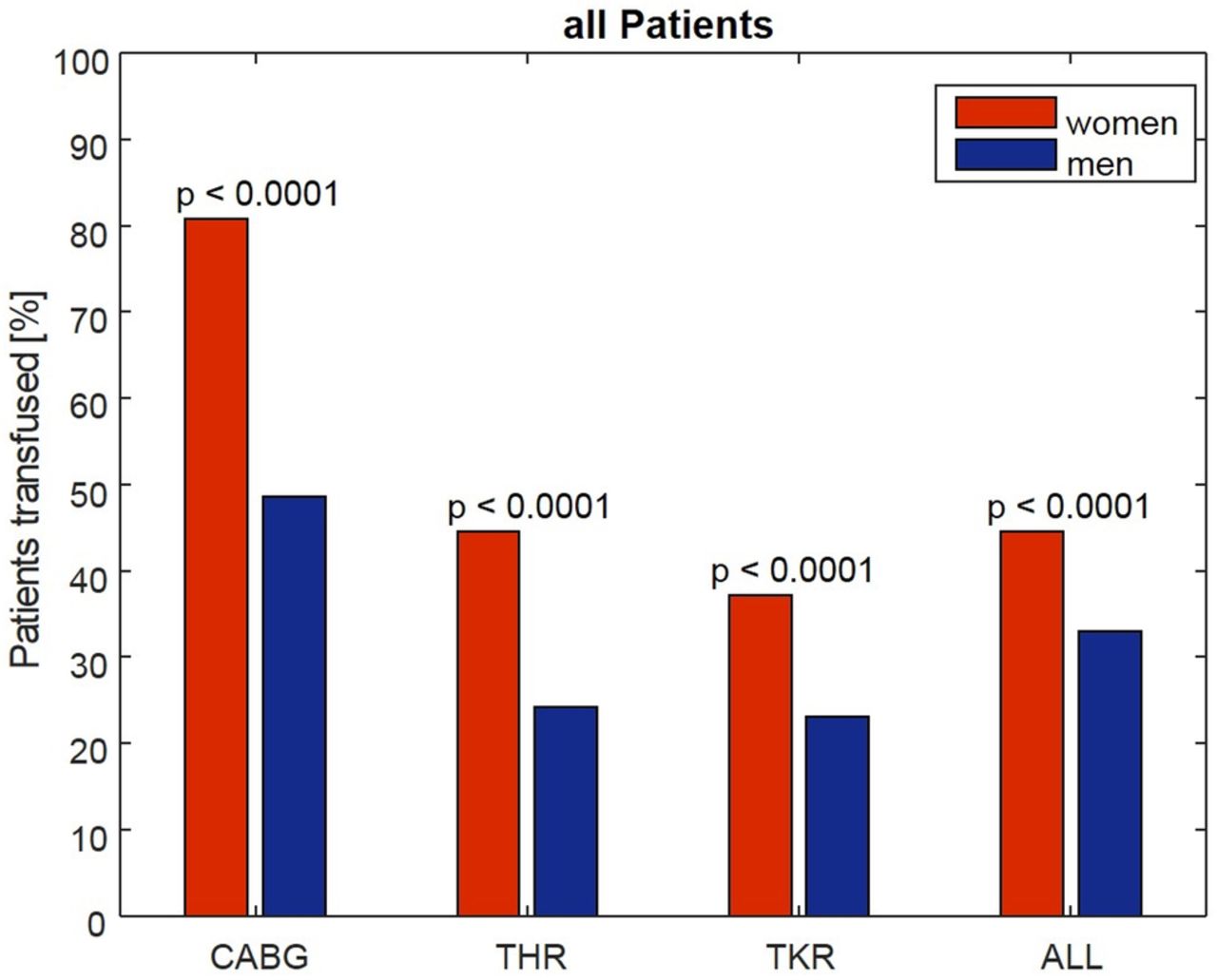
Results In all surgical groups, the transfusion rate was significantly higher in women than in men (CABG 81 vs 49%, THR 46 vs 24% and TKR 37 vs 23%). In transfused patients, the absolute blood loss was higher among men in all surgical categories while the relative blood loss was higher among women in the CABG group (52.8 vs 47.8%) but comparable in orthopaedic surgery. The relative RBC volume transfused was significantly higher among women in all categories (CABG 40.0 vs 22.3; TKR 25.2 vs 20.2; THR 26.4 vs 20.8%). On postoperative day 5, the relative haemoglobin values and the relative circulating RBC volume were higher in women in all surgical categories.
Conclusions The higher transfusion rate and volume in women when compared with men in elective surgery can be explained by clinicians applying the same absolute transfusion thresholds irrespective of a patient's gender. This, together with the common use of a liberal transfusion strategy, leads to further overtransfusion in women.
- Patient blood management
- gender
- transfusion
- overuse
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
It is a post hoc analysis using prospectively collected data from two similar and consecutive benchmark studies, including 6530 patients undergoing elective surgery in 23 centres.
The main focus was the gender differences in the transfusion-related modifiable risk factors such as anaemia, blood loss and transfusion of red blood cells (triad of adverse outcome).
Comparing absolute transfusion-related data and relative values in relation to the WHO's cut-off values enabled a fair gender comparison with baseline differences between men and women being eliminated.
Perioperative blood loss, including the so-called hidden blood loss, and red blood cell volume transfused were precisely calculated.
Owing to the observational character of the two benchmark studies, only routine parameters could be collected. As a consequence, several aspects of interest such as the causes of preoperative anaemia, cardiac comorbidities and data on transfusion outcomes could not be investigated.
Introduction
Women tend to live longer than men, but typically experience more stress, poorer health and more years with disabilities along the way.1 ,2 Furthermore, in clinical decision-making and therapeutic interventions, gender disparities are common. Women are less likely to receive coronary angiography and coronary interventions,3–5 implantable cardioverter defibrillators,6 dialysis and renal transplants7 ,8 or arthroplasties.9 Also, after surgical treatment, women have a higher risk for adverse outcomes and death, which may be at least partially attributable to a higher allogeneic transfusion rate.9–13
It is a matter of fact that women have a higher bleeding tendency14 ,15 and are more likely to be transfused than men.11–13 ,16–21 The latter phenomenon, together with the occurrence of perioperative blood loss and anaemia, may worsen their postoperative outcome. However, in contrast to other preoperative risk factors, these factors can be mitigated by adequate and timely prevention and treatment.
In the last few years, the modern concept of patient blood management has been developed by international experts and implemented worldwide.22 ,23 Its aim is to manage and preserve a patient's own blood by reducing the above-mentioned transfusion-related risk factors—anaemia, blood loss and red blood cell (RBC) transfusion—with the ultimate goal of improving the patient's outcome and safety.24 Therefore, identifying the underlying causes of the higher RBC transfusion rate in women and—as a consequence—enabling adequate and timely prevention and treatment might be of critical importance.
The aim of our study was a gender comparison in patients undergoing elective surgery with special attention to differences in transfusion-related modifiable risk factors for an adverse outcome.24
Methods
The present analysis included data from patients enrolled in two Austrian benchmark studies on blood use in elective surgery.20 ,21 Both studies were prospective, observational multicentre studies with 23 participating centres, which were randomly selected and stratified by region and level of care. The study design, selection and recruitment of the centres, patient selection, data collection, quality management and first-line data analysis were similar in the two studies. The first study was conducted from April 2004 to February 2005, and the second study from July 2009 to August 2010. The present post hoc analysis was conducted without funding (whereas the original two studies on which the post hoc analysis is based were exclusively funded by the Austrian Ministry of Health).
In the two studies, we collected data from patients undergoing primary unilateral cemented or non-cemented total hip replacement (THR), primary unilateral non-cemented total knee replacement (TKR) or coronary artery bypass graft (CABG) surgery. Based on the Austrian Data Protection Commission's review, informed consent from individual patients was not necessary because only deidentified data were collected and complete patient confidentiality was maintained. After obtaining approval from the local ethics committee (Ethikkomission des Landes Oberösterreich, 15 July 2009), we consecutively enrolled all eligible patients aged 18 years or older. Our exclusion criteria were any other concomitant surgery, emergency surgery and an underlying coagulopathy documented by a history of bleeding and/or laboratory testing (international normalised ratio >1.5 or activated partial thromboplastin time >35 s).
Primary outcome measures were the number of intraoperatively and postoperatively allogeneic and autologous RBC units transfused and differences in transfusion rate between men and women (until postoperative day 5). Secondary outcomes included perioperative blood loss in transfused and non-transfused patients, volume of RBCs transfused, perioperative haemoglobin values and circulating red blood volume on postoperative day 5.
We collected the following demographic and clinical data from the hospital records: patient age, body weight and height, preoperative use of platelet inhibitors or anticoagulants, type of anaesthesia, duration of surgery, use of a cell saver and length of hospital stay. In addition, we obtained routinely measured perioperative haemoglobin and haematocrit values and the number of RBC concentrates transfused. To account for gender differences, we presented the haemoglobin values as percentages of the anaemia cut-off values given by the WHO (figure 1). Comparing absolute transfusion-related data and relative values in relation to the WHO's cut-off values (WHO; women 120 g/L and men 130 g/L)25 enabled a fair gender comparison with baseline differences between men and women being eliminated.

Boxplots for absolute versus relative haemoglobin values. The significant gender difference in haemoglobin values (left) disappears by using relative values according the WHO guidelines25 (right). Hb, haemoglobin.
The body surface area was calculated using the Du Bois formula.26 The Nadler et al27 formula was used to calculate the patients' blood volume. The total RBC volume was derived by multiplying the calculated blood volume with the corresponding haematocrit level. A factor of 0.91 was applied to correct the haematocrit value for peripheral blood sampling.28 The overall perioperative RBC loss was calculated by subtracting the RBC volume on postoperative day 5 from the preoperative RBC volume and by adding the total RBC volume transfused. Differences in the average haematocrit (range 56–65%) and volume (range 250–316.7 mL) of RBC units from different blood banks were accounted for by multiplying the volume by the mean haematocrit of the respective unit. To calculate the salvaged, washed and returned RBC volume during cell saver use, we assumed a haematocrit level of 60%.29 To adjust for baseline differences in the total RBC volume, the lost and transfused RBC volumes were analysed as percentages of the patient's total circulating baseline RBC volume (relative RBC volume).
We provided a web-based electronic data capture system for data acquisition with a training programme included. During the initiation visit, the study physicians—mainly members of anaesthesia departments—received special training on the system. Data were recorded directly into the study database. The system provided login names and passwords dedicated for registration of patients, monitoring of recruiting progress, query management and source data verification, as well as an internal communication platform. Automatic data entry plausibility checks and mandatory data items enforced high data quality and completeness. On-site Contract Research Organisation (CRO) monitoring on a regular basis (at least twice during the study period per centre) was performed with special focus on continuity of enrolment and patient selection criteria.21
Descriptive statistics for the data were presented as median and IQR, or absolute and relative frequencies (%). Differences between women and men were tested for statistical significance using the Mann-Whitney U test for continuous variables and the χ2 test for frequencies, respectively.
Multivariate analysis was already performed in the two previous studies using logistic regression with RBC transfusion and multiple linear regression analysis with the relative volume of RBCs transfused (relative to the patient's estimated RBC volume) as the dependent variables. The independent variables included age, sex, body mass index (BMI), American Society of Anaesthesiology (ASA) physical status classification score, preoperative and lowest perioperative haemoglobin, type of anaesthesia, duration of surgery, usage of intraoperative cell salvage, infusion of washed versus unwashed shed blood, treatment with platelet (PLT) aggregation inhibitors and relative lost RBC volume. In CABG procedures, the number of bypasses, use of extracorporeal circulation and use of tranexamic acid were additional independent variables. Given the nature of the study, no formal sample size estimation was deemed necessary.20 ,21 In the current study, however, we conducted additional multivariate analyses on gender disparity and found only negligible differences.
We used Matlab, release 2015a (The MathWorks, Natick, Massachusetts, USA) for the statistical analysis. Box plots, bar charts and line diagrams were used to present the data graphically. A value of p<0.05 was considered to indicate statistical significance.
Minimising the risk of bias
Participating centres were randomly selected and stratified by region and level of care. Patients in each centre were enrolled consecutively. To ensure correct enrolment and adherence to patient selection criteria, onsite monitoring was regularly performed (twice per centre). During the initiation visit, the study physicians—mainly members of anaesthesia departments—received special training on the remote data entry system. Data were recorded directly into the study database.
Comparing absolute transfusion-related data and relative values in relation to the WHO's cut-off values enabled a fair gender comparison with baseline differences between men and women being eliminated. Differences in the average haematocrit and volume of RBC units from different blood banks were accounted for by multiplying the volume by the mean haematocrit of the respective blood bank.
Results
Patient characteristics and perioperative data
The present analysis included 6530 patients (3465 women and 3065 men; table 1), with 1491 patients (350 women and 1141 men) undergoing CABG surgery, 2570 patients (1424 women and 1146 men) undergoing THR and 2469 patients (1691 women and 778 men) undergoing TKR. Table 2 gives an overview of the demographic characteristics and perioperative parameters. Men were younger (except for those undergoing TKR) and taller than women, and they had a higher body surface area and a higher body weight. There were no gender differences in the BMI and the patients' overall health (American Society of Anaesthesiologists score). Women in the CABG group also had a significantly higher surgical risk of death (euroSCORE) than men. Tranexamic acid was the main antifibrinolytic agent used in the second benchmark study, and aprotinin was the one used in the first benchmark study. The prevalence of anaemia was also similar in both genders with the exception of patients undergoing CABG surgery; in this subgroup, preoperative anaemia was more common among women than among men (prevalence in women, 30.3% and prevalence in men, 23.7%). In younger patients below the age of 60, anaemia was more common in women, whereas at ages 70 years and older, anaemia was more common in men.
Patients included
Demographic data
Primary outcome variables
In all subgroups, the transfusion rate was significantly higher in women than in men (CABG 81% vs 49%, THR 46% vs 24% and TKR 37% vs 23%; figure 2). Also women received one or two RBC units more often than men (figure 3). Overall, the transfusion rates were significantly higher in patients with preoperative anaemia than in those with non-anaemia (total population: women 75% vs 38%, men 66% vs 25%; CABG: women 93.4% vs 75.4%, men 76.3% vs 40.0%; THR: women 77.0% vs 37.8%, men 60.7% vs 17.7%; TKR: women 65.4% vs 31.5%, men 51.8% vs 16.9%). Figure 4A, B shows the percentages of the transfused patients for the different surgical interventions, for patients with (top) and for those without (bottom) preoperative anaemia. Compared with the first study, the overall percentage of transfused patients and the mean number of RBC units transfused in the second study decreased in THR and TKR, but remained relatively unchanged in CABG surgery. Among the patients who received transfusions, there was no difference in the RBC volume as well as the number of units transfused between the studies. Usage of predonation of autologous blood in CABG procedures was negligible in the first (0.5%) and second studies (0.4%), and there was a substantial decrease of usage of predonation in orthopaedic patients from the first to the second study (THR, 11% to 4%; TKR, 8–3%, respectively).

Type of surgery and percentage of patients transfused. CABG, coronary artery bypass graft; THR, total hip replacement; TKR, total knee replacement.

Percentage of patients receiving a given number of RBC units (indicating that women received one or two RBC units more often as men do, mostly at the expense of the percentage of patients who did not receive any transfusion. RBC, red blood cell.

(A and B) Transfusion rate in patients with anaemia (top) and non-anaemia (bottom). CABG, coronary artery bypass graft; THR, total hip replacement; TKR, total knee replacement.
Secondary outcome variables
The absolute blood loss among patients undergoing CABG was comparable in both genders, and that among patients undergoing orthopaedic surgery was slightly lower in women than in men. In contrast, the relative blood loss among patients undergoing CABG surgery was considerably higher in women than in men; it was also slightly higher in women in the THR group, whereas it was similar in both genders in the TKR group. The absolute RBC volume transfused was higher in women than in men among patients undergoing CABG surgery and equal in both genders among orthopaedic patients, whereas the relative RBC volume transfused was twice as high in women compared with men in the CABG group, and it was also elevated in women undergoing orthopaedic surgery. On postoperative day 5, absolute circulating blood volumes were significantly higher in men whereas relative blood volumes were significantly higher in women in all categories (table 3).
Transfusion-related variables (all patients)
In transfused patients, the absolute RBC loss was lower in women than in men in all surgical categories, but the relative RBC loss was higher in women than in men in CABG surgery (52.8% vs 47.8%, p<0.0001) and comparable in both genders in orthopaedic surgery. The absolute RBC volume transfused was slightly higher in men. However, the relative RBC volume transfused was significantly higher in women than in men (26.4% vs 20.8%; p<0.0001; table 4 and figure 5A–C). The absolute preoperative RBC volume was ∼30% higher in men than in women, and the RBC volume on postoperative day 5 was ∼20% higher in men. On the other hand, on postoperative day 5, the relative RBC volumes were elevated (by ∼5%) in women in all surgical subgroups when compared with men.
Transfusion-related variables (transfused patients only)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A–C) Boxplots for absolute and relative RBC volumes: lost (left) and transfused (right) for CABG (top), THR (middle), TKR (bottom)—women versus men for transfused patients only. CABG, coronary artery bypass graft; RBC, red blood cell; THR, total hip replacement; TKR, total knee replacement.
In transfused patients, the absolute preoperative haemoglobin values were generally lower in women, and relative haemoglobin values were comparable except for the TKR subgroup. The lowest measured haemoglobin (nadir haemoglobin) value was slightly lower in women than in men in orthopaedic surgery, whereas the relative values were higher in women than in men among those undergoing CABG surgery. On postoperative day 5, the absolute haemoglobin values were slightly higher in men (except for CABG patients). In comparison, the relative haemoglobin values on postoperative day 5 were elevated in women in all surgical categories (table 4).
Predictors of transfusion
Apart from female sex, the relative lost RBC volume, relative preoperative haemoglobin and the lowest relative postoperative haemoglobin are strongest and independent predictors for RBC transfusion in all procedures (table 5). Regional anaesthesia was a significant factor in THR, ASA score was significant in TKR, and BMI and PLT inhibitors were significant predictors for transfusion in CABG.
Predictors of transfusion
First versus second study
Compared with the first study, in the second study the overall percentage of transfused patients and the mean number of RBC units transfused decreased in THR and TKR, but remained relatively unchanged in CABG surgery. Among the patients who received transfusions, there was no difference in the RBC volume and the number of units transfused between the studies.
Transfusion rate in THR procedures decreased in seven centres while it increased in one centre compared with the first study. Eight centres had decreased transfusion rates in TKR. In CABG, transfusion rate significantly increased in one centre and decreased in another centre compared with the first study. Usage of predonation of autologous blood in CABG procedures was negligible in the first (0.5%) and second studies (0.4%), and there was a substantial decrease of usage of predonation in orthopaedic patients from the first to the second study (THR, 11% to 4%; TKR, 8% to 3%, respectively).20 ,21
Discussion
The present study identified a higher transfusion rate in women compared with men in three surgical categories. Other findings of this study are:
Although the absolute perioperative blood loss was higher in men in all subgroups, the relative blood loss was comparable between the genders in orthopaedic surgery, and in the CABG subgroup, it was higher in women.
Furthermore, the relative RBC volume transfused was significantly higher in women in all surgical categories, especially in CABG surgery.
This was accompanied by a higher relative nadir haemoglobin value and a higher haemoglobin value on postoperative day 5 in women.
In addition, the calculated relative postoperative RBC volume in women was ∼5% higher than that in men across all surgical groups.
There was no gender difference in the overall prevalence of preoperative anaemia as defined by the gender-specific WHO cut-off values.
Anaemia, blood loss and transfusion of RBCs constitute a triad of risk factors for adverse patient outcomes.24 ,30–35 Each of these three parameters represents a risk factor in itself and their combination may further potentiate the risk of an adverse outcome.36 Within this triad, a vicious cycle is set in motion: blood loss and bleeding induce anaemia or exacerbate pre-existing anaemia. Anaemia triggers transfusion, and transfusion—besides having many other adverse effects—increases the risk of re-bleeding, potentially leading to additional blood loss, as shown in several studies.34 ,37–40 The intention of breaking this vicious cycle by modifying these risk factors has led to the development of the concept of patient blood management, which is based on three pillars: optimisation of the patient's endogenous RBC mass; minimisation of diagnostic, interventional and surgical blood loss and optimisation of the patient's tolerance of anaemia.22 ,41 In most clinical scenarios, application of just the first two pillars is sufficient to address all three risks of the triad. Optimisation of the RBC mass and the reduction of blood loss keep the haemoglobin levels of most patients above a level where transfusion might be considered. However, addition of the third pillar can further reduce transfusion rates.42
With regard to the optimisation of the patient's endogenous RBC mass (first pillar), women generally seem to be less susceptible to anaemia-induced adverse events than men. For example, in normal life, the lowest risk for mortality occurs at haemoglobin values between 130 and 150 g/L in women and between 140 and 170 g/L in men.43–46 In a cohort of 6880 elderly patients without severe comorbidities, mild and moderate anaemia was significantly associated with a higher mortality in men but not in women.32 ,47 In a recent publication focusing on non-emergent CABG surgery, a low haematocrit and blood transfusion were significant predictors for major morbidity in men, whereas in women blood transfusion was the only predictor of major morbidity.32 In non-cardiac surgery, the mortality was higher in men than in women at similar haemoglobin levels.
The prevalence of preoperative anaemia in the present study was similar in both genders, so this factor cannot explain the higher transfusion rates in women. The fact that the prevalence of anaemia among women was similar to that among men might be attributable to the higher age of the patients included in the study,48 because the higher prevalence of low haemoglobin values observed in younger women disappears with increasing age. After the age of 75 years, men have, in fact, a higher prevalence of anaemia than women, with the prevalence among men being highest at age 85 years and older.49 ,50
The observation that anaemia is associated with a poor prognosis in many disorders is not a sufficient reason to assume a cause-and-effect relationship. Anaemia of chronic disease in particular may be associated with an adaptive physiological response.51 ,52 The treatment of mild-to-moderate anaemia of chronic disease may therefore not always bring the desired improvement or may even increase the mortality in some cases.53 Nevertheless, optimisation of the preoperative blood volume up to the WHO cut-off values should be an integral strategy to reduce the transfusion requirements in both genders.54 ,55
The amount of perioperative blood loss (second pillar) depends on the surgical technique, the management of perioperative coagulation and the blood conservation techniques used. The degree of acute blood loss that patients can safely tolerate is inversely related to their baseline haemoglobin concentration and the decrease of their RBC volume.56 A decrease of at least 50% from the preoperative haemoglobin level during cardiac surgery is associated with adverse outcomes even if the absolute haemoglobin level remains above the commonly used transfusion threshold of 7.0 g/dL.57
In the present study, the absolute blood loss was smaller among women than among men in all surgical subgroups, but the relative perioperative blood loss was 5% higher among women than among men in the CABG subgroup, and it was comparable between men and women in the orthopaedic surgery subgroups. The higher blood loss among women undergoing CABG surgery may be attributable to the extreme haemodilution associated with extracorporeal circulation. As women have a lower BMI than men, their haemodilution during the operation is more profound, and women therefore tend to receive more transfusions during and after the CABG operation.18 Nevertheless, the differences in blood loss alone cannot explain why the RBC volume transfused among women was twice that among men in the CABG group and 25% higher than that among men in the orthopaedic surgery groups (table 4).
With regard to the tolerance of anaemia (third pillar), it is possible that the ability to compensate for low haemoglobin values differs by gender. Moreover, to the best of our knowledge, neither cut-off values nor transfusion guidelines exist for postmenopausal women.58 ,59 Several authors have suggested that anaemia in women beyond menopause should be defined by a higher haemoglobin threshold, similar to that used for men.44 ,60 ,61 Current transfusion guidelines revolve around absolute haemoglobin values and do not account for this phenomenon, nor do they consider the special needs of women in general.59 ,62–64 In fact, in routine clinical practice, similar transfusion triggers are applied in both genders.65
The present study has several limitations. First, it is a post hoc analysis that uses data from two similar consecutive benchmark studies.20 ,21 Second, because financial resources were limited, postoperative outcomes could not be studied. Third, because of the observational character of the two benchmark studies, only routine parameters could be collected. Therefore, several aspects of interest such as the causes of preoperative anaemia could not be investigated.
A main strength of the study is the fact that the perioperative blood loss was calculated and the so-called hidden blood loss is therefore included in the analysis. Moreover, we compared absolute transfusion-related data and relative values (in relation to the WHO cut-off values).25 This enabled a fair gender comparison because baseline differences between men and women were eliminated.
The present findings—that women had a higher postoperative RBC volume in all surgical groups and higher intraoperative and postoperative haemoglobin levels, together with a higher relative RBC volume transfused—are clear indicators that the transfusion strategies applied in women were too liberal. These results could have a significant impact on blood usage levels and possibly lead to improvements in outcome and patient safety. Gender-specific transfusion thresholds and dosing are neither recommended by guidelines nor common in clinical practice. Therefore, the findings of this study might be generalisable across most transfused populations. Once clinicians are aware of the fact that women tend to be overtransfused, measures can be taken to address this matter. These include the correction of preoperative anaemia, the reduction of perioperative blood loss by optimising the surgical technique, the reduction of the transfusion volume (eg, by implementing a single-unit strategy) and the use of lower haemoglobin values as transfusion triggers. Such strategies may dramatically reduce the transfusion rate among women while improving outcome and patient safety.
Conclusion
The higher transfusion rate and volume in women, compared with men, in elective surgery can be explained by clinicians applying the same absolute transfusion thresholds irrespective of a patient's gender even though women have a lower baseline RBC volume. This, together with the common use of a liberal transfusion strategy in elective CABG and orthopaedic surgery despite the recommendations in relevant guidelines, leads to overtransfusion in women. Given the possibility to pre-empt transfusions through the treatment of modifiable risk factors by applying the patient blood management concept, a beneficial change in practice is warranted. Given the accumulating evidence on transfusion outcomes from meta-analyses of RCTs,66–69 comparing liberal versus restrictive transfusion thresholds, a prospective randomised controlled trial (RCT) comparing gender-specific transfusion thresholds and targets with current standard of care is warranted.
References
Footnotes
Contributors HG initiated and implemented both benchmark studies, designed data collection tools, and wrote and revised the paper. He is a guarantor. GS wrote the statistical analysis plan, analysed the data and revised the drafted paper. SN cleaned and analysed the data. PK monitored data collection for both trials, drafted and revised the paper. AH implemented both benchmark studies and revised the drafted paper.
Competing interests AH lectures for Vifor Pharma and TEM international.
Ethics approval Ethikkomission des Landes Oberösterreich, 15 July 2009.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.