Article Text

Abstract
Objectives In this study, the frequency and consequences of aggressive assaults on employees in the German healthcare and welfare system were investigated.
Design A retrospective cross-sectional study.
Setting Employees in the German healthcare system and their experiences of violence and aggression were examined in this study.
Participants The sample consisted of 1973 employees from 39 facilities (6 facilities for the disabled, 6 hospitals and 27 outpatient and inpatient geriatric care facilities) who have regular contact with patients or clients.
Main outcome measures The frequency of physical and verbal violence towards employees and the consequences of aggressive assaults were analysed.
Results 56% of respondents had experienced physical violence and 78% verbal aggression. The highest frequency of physical violence was in inpatient geriatric care (63%) (p=0.000). Younger workers run a higher risk of being affected by physical violence than older colleagues (OR 1.8, 95% CI 1.3 to 2.4). There is also an increased risk of experiencing physical violence in inpatient geriatric care (OR 1.6, 95% CI 1.2 to 2.0). Around a third of workers feel seriously stressed by the violence experienced. The better the facility trained employees for dealing with aggressive and violent clients, the less risk employees ran of experiencing either verbal aggression (OR 0.5, 95% CI 0.4 to 0.7) or physical violence (OR 0.7, 95% CI 0.6 to 0.9). Training by the facility has a positive effect on experienced stress (OR 0.6, 95% CI 0.4 to 0.8).
Conclusions Violence towards nursing and healthcare personnel occurs frequently. Every third respondent feels severely stressed by violence and aggression. Occupational support provisions to prevent and provide aftercare for cases of violence and aggression reduce the risk of incidents and of perceived stress. Research is needed on occupational support provisions that reduce the risk of staff experiencing verbal and physical violence and the stress that is associated with it.
- Epidemiology
- Public Health
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
For many nursing and healthcare professionals, violence is part of their daily professional life.
-
In Germany, neither instances of violence nor the consequences of violence in the nursing and healthcare professions have yet been recorded systematically.
-
In this study, the frequency and consequences of violence on employees in the German healthcare and welfare system are investigated.
Key messages
-
Violence towards nursing and healthcare personnel occurs frequently. Over the preceding 12 months, 56% of respondents had experienced physical violence and 78% verbal aggression.
-
Employees in inpatient geriatric care had an increased risk of experiencing physical violence.
-
The feeling of stress is most marked among employees working in workshops for people with disabilities and in outpatient care.
-
Training by the facility has a positive effect on the stress that staff experience.
Strengths and limitations of this study
-
The response rate was especially low in participating hospitals.
-
That may have led, in the hospitals, to overrating of both the frequency of violence and the stress that it caused.
-
Given that it was a retrospective survey, the risk of a recall bias also cannot be ruled out.
Introduction
Workplace violence is considered an occupational burden worldwide,1 and for many people who work in the nursing and healthcare professions, aggression and violence are part of their everyday professional life.2 The International Labour Office 3 defines violence and aggression on the basis of criteria developed by the European Union4 on the subject of violence and aggression at work.5 These state that violence comprises ‘incidents where staff are abused, threatened or assaulted in circumstances related to their work, including commuting to and from work, and involving an explicit or implicit challenge to their safety, well-being or health’. The present study examines violence and aggression shown by patients/clients towards nursing and healthcare staff and employees in workshops and residential homes for people with disabilities. In this context, violence can include any form of verbal, physical or sexual aggression or physical violence.
Background
In an overview of studies on violence and aggression towards healthcare workers by Zeh et al,2 11–96% of healthcare workers said that they had been affected by violence in the past 12 months. In the healthcare system, violence is not restricted to high-risk areas such as emergency rooms or psychiatric settings.1 ,6 ,7 Violence and aggression are also major problems for nurses in elderly care.8–12 Compared with other occupational groups, healthcare professionals are at a higher risk of violence or aggression.6 ,13 ,14 Within this context, nurses have been identified as the occupation at most risk of patient-related violence and nurses are exposed to the highest risk of violence.15 ,16 For example, Lau et al17 stated that between 60% and 90% of nurses reported experiencing verbal and physical violence. The perpetrators of workplace violence are primarily patients or their relatives.13 ,18–20 Farrell et al7 identified the perpetrators of either verbal or physical violence by patients in 74% and 97% of cases, respectively, followed by aggression shown by patient/client visitors in 35% and 7% of cases, respectively. There is also a large proportion of horizontal violence from other healthcare workers, professionals and other nurses.18 But horizontal violence was outside the context of this study. However, incident reporting of workplace violence and aggression in this setting is not routine practise and a high number of unreported cases must be assumed. The true incidence rate of patient/client-related violence is thus unknown.2 ,16 ,21 ,22
Work-related violence can negatively affect the psychological and physical well-being of the healthcare staff,23 ,24 job motivation and quality of care as well as cause longer periods of absenteeism and a deterioration of the work environment.5 ,25
Systematic research of the causes and consequences of aggression and violence towards employees in the healthcare system is just starting in Germany. Studies are often limited to investigations in mental health institutions or emergency care departments. Other areas of the healthcare system, such as care for elderly or for people with disabilities, are still being neglected in Germany and only a few studies have examined the threats and violence in elderly care.10 ,12 ,26 There are no data available for employees in outpatient care and in facilities which provide care for the disabled in Germany. There are also gaps in the research regarding the prevention of violence and aggression as well as aftercare for incidents against nurses and healthcare workers. Although there are training programmes for de-escalation management and educational measures for healthcare workers, the systematic evaluation and effectiveness of such approaches are rare.27 ,28 There is also a lack of care for victims following aggressive incidents.25
Aims of the study
The aim of this study was to give an overview about the burden of violence experienced by nursing and healthcare personnel in different settings in Germany. Therefore, we described the frequency, type and severity of verbal and physical, patient-related violence towards employees in general hospitals, inpatient geriatric care, outpatient care, workshops and residential homes for people with disabilities in the preceding 12 months, and we investigated the consequences of such incidents. In addition, the availability of measures for dealing with aggression and violence in the workplace are also analysed.
Methods
Study design
Between September 2008 and February 2009, a retrospective survey of employees in the German healthcare and welfare system and their experiences of violence and aggression in the preceding 12 months were carried out by means of a standardised questionnaire. All verbal and physical attacks by patients or clients were defined as an incident of aggression or violence.
Setting
Different institutions in the German healthcare and welfare system were asked to participate: general hospitals, nursing homes for the elderly, outpatient care institutions and facilities offering care for the disabled.
Participants
The sample consisted of 1973 employees from 39 facilities (6 facilities for the disabled, 6 general hospitals and 27 outpatient and inpatient geriatric care facilities). The survey covered employees who are in frequent direct contact with patients or clients and residents in the preceding 12 months. At some facilities, especially institutions offering care for the disabled, they also included housekeeping and cleaning staff, community service workers or interns who had regular direct contact with clients and residents.
Data sources and measurements
The experience of violence and aggressive behaviour and the measures taken for managing such situations were recorded via a self-administered questionnaire which was drawn up along Staff Observation Aggression Scale-Revised (SOAS-R) guidelines by Nijman et al.29 The questionnaire, along with a covering letter that described the purpose of the study, instructions for the participants and information about informed consent, were sent to the facilities and given by the supervisor to all employees who fulfilled the inclusion criteria. Participants returned the completed questionnaires to the investigator in envelopes provided within 2 weeks. The questionnaire used in this study was tested for comprehensibility and suitability in preliminary trials on 123 nursing and healthcare staff at a psychiatric unit, an inpatient care facility for the elderly and a facility for people with disabilities.25
Variables
The questionnaire contained 20 questions divided into three topic areas. The first block covered questions about the sociodemographic data of the participants, such as gender, profession, age, workplace setting and their qualifications and experience. In the second part, their experience of violence and aggressive behaviour from patients is surveyed. First, they were asked separately and retrospectively about physically and verbally aggressive behaviour. Further questions dealt with the type and purpose of the aggressive behaviour, measures taken to contain aggressive behaviour and the reporting of these incidents. The last block of questions covered the management of these episodes. It included questions about the physical and emotional consequences, general stress due to incidents, the support available in the institution and its utilisation as well as social support.
Ethics
Participation in the study was voluntary. To ensure anonymity, no names or other identifiers were used. All participants gave their written, informed consent to taking part in the study, which had been approved by the Hamburg Medical Council's Ethics Commission.
Statistical methods
The data were analysed using SPSS V.16. Descriptive statistics were used to describe the sample. Associations between categorical variables were tested with χ2 tests. For the logistic regression models, we summarised the original visual analogue 10-step scales from 1 to 10 for the assessment of stress, social support and training by the institution into three categories: poor or low from 1 to 3, intermediate from 4 to 7 and good or high from 8 to 10. ORs and 95% CIs (at p<0.05) were calculated by means of logistic regression to determine the factors that might influence the frequency of violence and the stress experienced after assaults.
A possible influence of different response rates (selection bias) on findings for the occurrence of violence was estimated. For each work area, the figures submitted by facilities with a response rate above or below the average were compared with each other using the χ2 tests.
Results
In all, 6302 questionnaires were distributed (figure 1). The overall response rate was 31.3% (n=1973), with the highest response rate being from residential homes and workshops for people with disabilities (42%). The lowest response rate was found in hospitals (26%). The characteristic of the study population is described in table 1. The majority of the participants worked as nurses (46%) and were aged 40–49 (36%). Nearly half of the participants (48%) had been working in nursing or healthcare for more than 15 years.
Characteristics of the study population (n=1973)
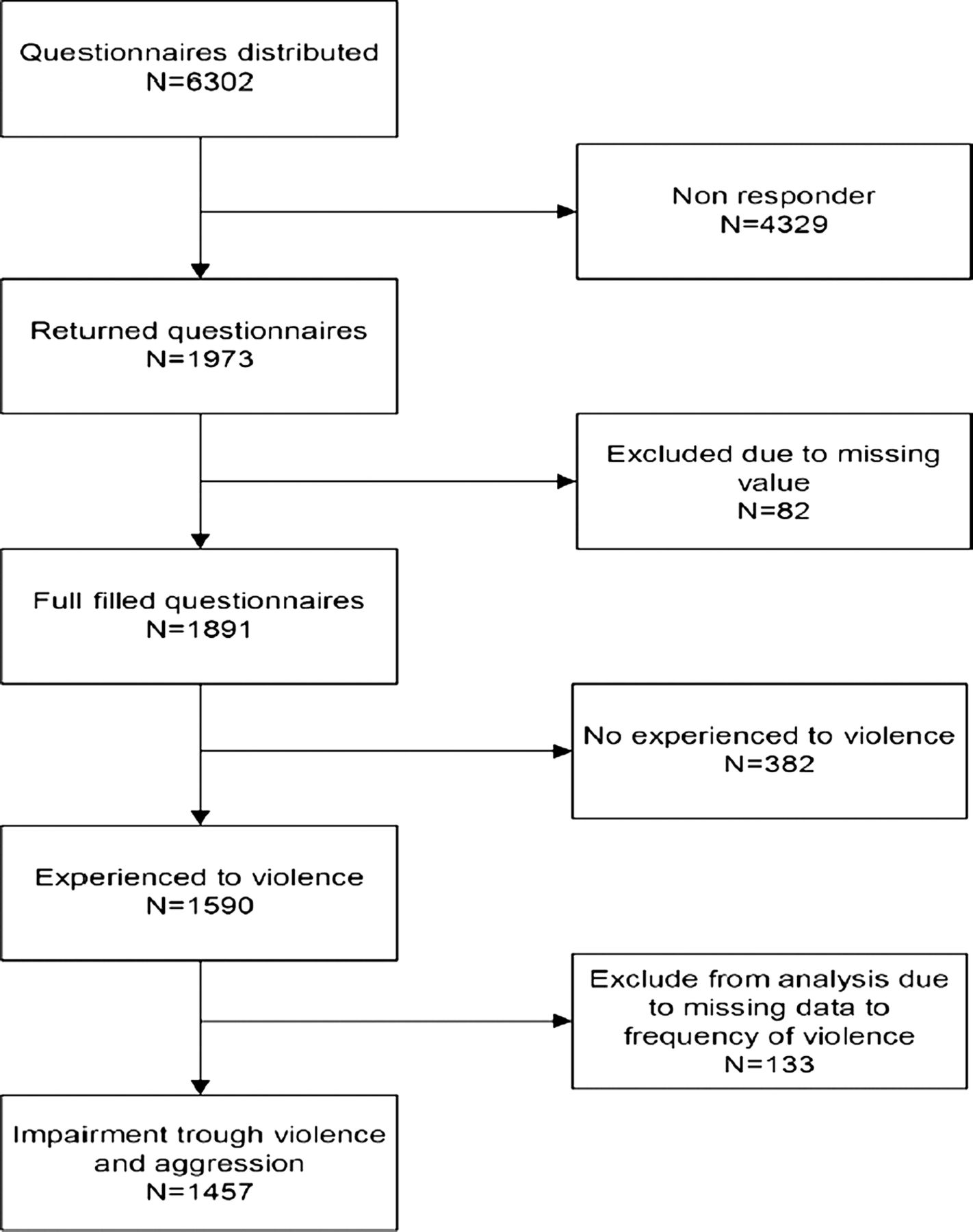
Flow chart ‘generation of the study population.’
Frequency of verbal and physical violence
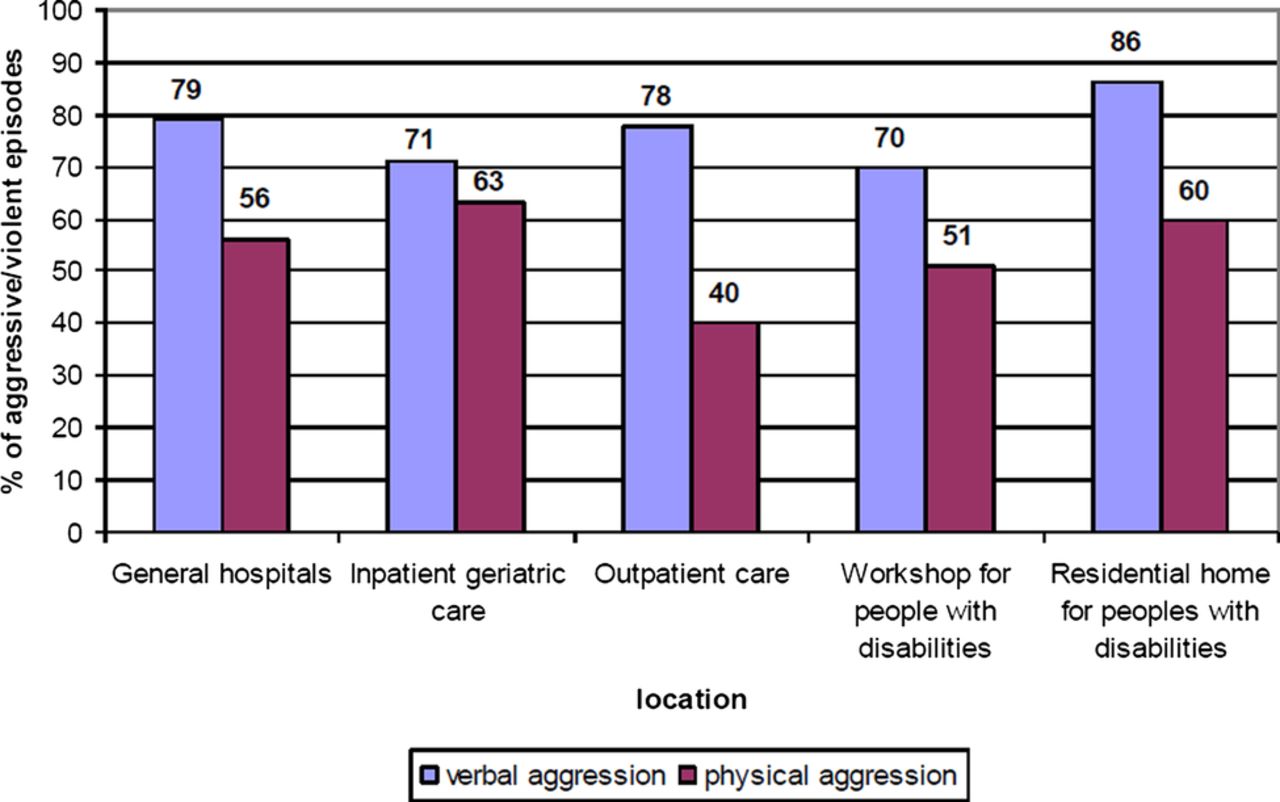
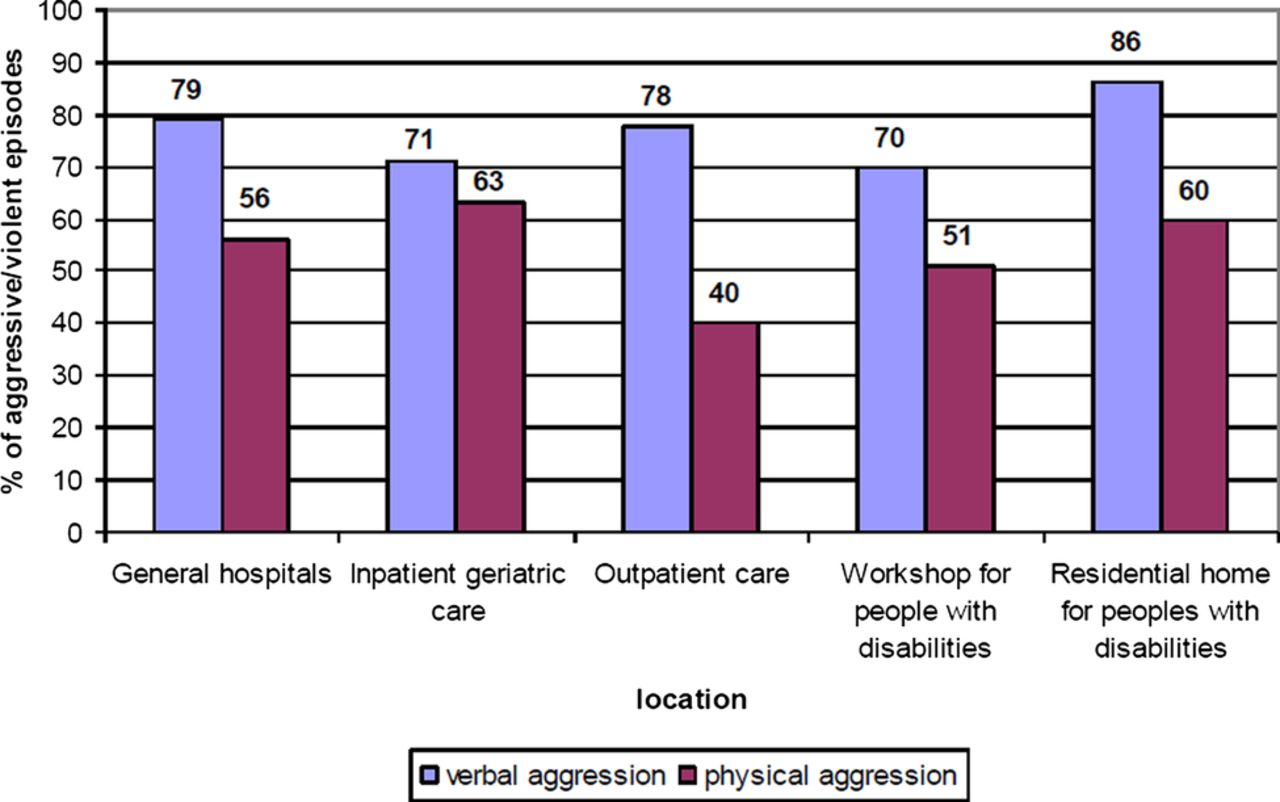
Over the previous 12 months, 56% of respondents had experienced physical violence and 78% verbal aggression. In all, 44% of respondents said they experienced physical violence and 68% verbal aggression once or more per month. The highest frequency of physical violence was found in inpatient geriatric care (63%) and the lowest in outpatient care (40%). These differences were statistically significant (p=0.000). Staff at residential homes for people with disabilities most frequently noted having experienced verbal aggression (86%). The lowest frequency of verbal aggression was, in contrast, reported by workshops for people with disabilities (figure 2).
{kind=link}
{kind=link}
Frequency of verbal and physical violence by workplace.
Type of violence
In all sectors, employees most frequently experience verbal aggression. Threatening gestures are also reported mainly by employees in facilities for people with disabilities (residential homes, 50%; workshops, 42%). In contrast, staff at inpatient facilities for the elderly (52%) and in hospitals (42%) most frequently reported being at the receiving end of pinching and scratching. Employees at inpatient facilities for the elderly more frequently reported being hit (35%) than respondents employed in other areas (Table 2).
Types of violence in the preceding 12 months by workplace
Management of episodes of violence in the 12 months preceding data collection
In all sectors, the employees affected mainly responded verbally to verbal and physical assaults, calling on the people who assaulted them to change their behaviour. Both medication and requests for support were most frequent in hospitals (34% and 34%, respectively). The police were called 57 times (6%) by hospital staff and 18 times (10%) by employees in residential homes for people with disabilities.
Reporting accidents
Only 41% (n=816) of the episodes of violence were reported, 60% (n=789) to a supervisor and only 2% (n=38) registered as an occupational accident with the statutory accident insurers.
Emotional and physical consequences
In all work areas, the majority of employees reacted with anger and annoyance to the violence that they experienced in the 12 months preceding data collection. At facilities for people with disabilities, their second most frequent reaction was a feeling of disappointment (workshops, 46%; residential homes, 30%), and in other work areas a feeling of helplessness. Staff at inpatient facilities for the elderly most frequently claimed to have been subjected to physical violence (32%) and pain for less than 10 min (20%; table 3).
Consequences of verbal or physical violence for the study participants by workplace
Training and social support provided by the facility
In total, 27% of respondents (27%) said they felt that their facility had prepared them particularly well for situations involving aggressive or violent clients (table 1). In contrast, 65% stated that the support given by colleagues was good. In hospitals and in residential homes for people with disabilities, 42% and 11%, respectively, of the respondents stated that they had received no instructions on how to deal with violence.
Risk factors for experiencing physical and verbal violence
Younger workers under 30 years run a higher risk of being affected by physical violence (OR 1.8, 95% CI 1.3 to 2.5) or verbal aggression (OR 1.9, 95% CI 1.3 to 2.9) than older colleagues.
Another risk factor for physical and verbal violence is the work sector. Compared with inpatient nursing staff, employees at inpatient geriatric care units also run a higher risk of experiencing verbal aggression (OR 1.7, 95% CI 1.0 to 2.9) and there is also an increased risk of experiencing physical violence (OR 2.2, 95% CI 1.6 to 2.9). Employees who have been trained by their facilities in how to deal with violence run a lesser risk of experiencing physical and verbal violence (OR 0.7, 95% CI 0.6 to 0.9; OR 0.5, 95% CI 0.4 to 0.7) than staff in facilities where no such training is provided (table 4).
Frequency and ORs and 95% CIs for verbal and physical violence (n=1891)
Risk factors for the experience of stress
Out of 1891 employees who had experience of verbal and physical violence, 434 participants gave no further information about this experience in the preceding 12 months. Of 1457 participants, around a third of employees feel seriously stressed by the violence experienced. This feeling of stress is most marked among workers in workshops for people with disabilities and in outpatient care (38% and 37%, respectively). Women are more frequently stressed than their male colleagues by the violence they experience (OR 1.5, 95% CI 1.1 to 2.1). In contrast to hospital staff, employees in outpatient (OR 1.3, 95% CI 0.9 to 2) and inpatient healthcare for the elderly (OR 0.5, 95% CI 0.4 to 0.8) feel stressed more often. The frequency of violence experienced also relates to the sense of personal stress. Those who experience physical violence on a daily basis are affected by stress (OR 3.0, 95% CI 1.6 to 5.5; table 5).
Frequency and risk factors influencing stress in the employees affected by violence and aggression (n=1457)
The better the facility is at training employees for dealing with aggressive and violent clients, the less risk employees run of experiencing either verbal aggression (OR 0.5, 95% CI 0.4 to 0.7) or physical violence (OR 0.7, 95% CI 0.6 to 0.9). Good training by the facility in question has a positive effect on the stress that staff experience (table 5).
Discussion
For the first time, a study has been conducted in Germany that analysed violence and aggression in various healthcare and welfare settings. In line with international literature,16 ,25 ,30 this study showed that violence and aggression towards healthcare staff is frequent. In all, 56% of the respondents had experienced physical, and 78% verbal, violence. There were major differences between employment sectors.
Inpatient geriatric care and outpatient care for the elderly
The highest prevalence of physical violence was found in inpatient geriatric care, and the lowest in outpatient care. Mullan and Badger12 found in their study of violence and aggression towards staff working with older patients that 51% of the staff had experienced an incident of violence. Studies performed in Swedish nursing homes give prevalence values of between 11% and 40%.31 ,32 Josefsson and Ryhammar10 analysed the threats and violence towards staff in Swedish public elderly care homes and found that 48% of nurses had experienced indirect threats of violence, 40% direct threats and 45% had witnessed violence and threats towards other staff. In the German study by Franz et al,25 a high prevalence of violence and aggression towards staff in two nursing homes was found. Overall, 83.9% of the staff experienced physical violence and 90.3% verbal aggression. These rates are higher than in the present study (63% and 71%, respectively). Studies have shown that violence and aggression are more likely to occur among older people with cognitive impairment than among those with no cognitive impairment.33 Most of the aggressive behaviour occurs in direct care situations, such as bathing or showering, oral hygiene, dressing, etc. The rising number of dementia patients in care homes for the elderly could also be a reason for the increase in violence in inpatient geriatric care. In the literature, some authors stated that older people with dementia are sensitive to changes in the environment and workplace factors such as being short staffed or staff being rushed.33 Overcrowding, too much noise, locked doors and a lack of space and privacy, or inexperienced caregivers, can trigger aggression.26 ,32 ,33
Residential homes and workshops for people with disabilities
Employees in residential homes for people with disabilities showed the highest rates of verbal aggression (86%) compared, for example, to workshops for people with disabilities (70%). Franz et al25 found a prevalence of 77.4% for physical violence and of 42% for verbal aggression in workshops for people with disabilities. Similar rates were found for residential homes for people with disabilities, which varied between one-third and 80%.34 ,35
Experience of violence in several working groups
In addition to nursing staff, we also interviewed people working in other professions, such as social workers. As described in other studies, nursing staff are the most prominent high-risk group,36 but people in pedagogic positions also report a high prevalence of aggression and violence. These results underline how important it is to deal with this issue of workplace violence and aggression towards nursing staff, and show that other professional groups who have frequent contact to patients and clients should not be neglected.
Gender
In an Italian study, 49% of the nurses had experienced aggression in the previous year, and this happened more often to female nurses (52%) working in emergency care units and in geriatric and psychiatric units.30 In contrast to Zampieron et al,30 we found no higher risk of aggression and violence towards female nurses. In line with our study, Lundström et al35 also find no gender-related differences in the frequency of experiences of violence. In contrast, Estryn-Behar et al37 report in their study that women run a lower risk of experiencing violence than men. In our study, female nurses ran no higher risk of violence, but if they did experience violence, they felt more stressed by it than their male colleagues. It has been noted in this connection that women run a higher vulnerability risk after traumatising events.38
Age
In line with other studies,26 ,32 ,35 ,39 we found that younger employees run a higher risk of being affected by physical violence than older colleagues (OR 1.8, 95% CI 1.3 to 2.5). In contrast to these findings, Hegney et al18 found no significant differences in reported workplace violence with age. In the study by Zamperion et al,30 they also found no association between age and the risk of aggression.
Consequences of experienced violence
Several studies have demonstrated the negative influence of violence and aggression on the psychological and physical well-being of the affected person16 ,23 ,24, as well as on job motivation and quality of care.40 The consequences are emotions such as anger and anxiety, as well as psychological disorders such as burnout.41 ,42 In line with Richter, we also found that the majority of the physical injuries are generally slight and that no medical care is required.43 However, our data indicate that many employees felt emotions such as anger, disappointment, self-doubt, helplessness and anxiety after such incidents. As a consequence, the employees reacted more tensely and more carefully.
Feelings of stress due to violence
Nurses, doctors and social workers are all high on the list of occupations with serious stress levels and while violence constitutes almost a quarter of all violence at work (24%).5 Di Martino stated when stress and violence interact at workplace their negative effects cumulate in an exponential way.5 In our study the feeling of stress due to physically or verbally aggressive behaviour was mostly classified as intermediate.
This feeling of stress is most marked among workers in workshops for people with disabilities and in outpatient care (36.9% and 37%, respectively). Employees in outpatient healthcare may be less affected by violence and aggression, but they more frequently feel stressed by it. In spite of the higher frequency of verbal and physical violence in inpatient care of the elderly, employees in inpatient geriatric care run a lower risk of feeling seriously stressed by the experience of violence than employees in inpatient nursing care. With the increase in incidents and poor social support, the perceived stress increased. Franz et al25 found the highest feeling of stress among employees in nursing homes. In all, 35% of the staff in nursing homes felt highly stressed due to aggression compared to workers in psychiatric clinics (27%) and workshops for people with disabilities (19%). Richter et al23 investigated patient assaults among staff members in a psychiatric hospital. In 14% symptoms of a post-traumatic stress were diagnosed. In a systematic review from Needham and colleagues non-somatic effects of patient aggression on nurses were investigated. The predominant responses were feelings of anger, fear or anxiety, post-traumatic stress disorder symptoms guilt, self-blame and shame.24
Social support and training
Asked about the social support they had received after experiencing violence, respondents most often said that colleagues had given them social support. Hahn et al 1 found that when dealing with workplace violence and aggression, social support from colleagues, family and friends seems to be more helpful than that provided by the institutions. Our findings indicate, however, that good support provided by colleagues after an assault has no influence upon how upset the victims feel. A comparable finding in the Kaluza study shows that only a weak link was found to exist between social support and psychosocial disorders.44
Violence management
In many countries, occupational health and safety legislation, along with policies which emphasise a requirement for training in violence management, were adopted.13 ,14 ,39 In our study, training by the employer for possible experiences of violence was found to have a positive correlation on both the sense of stress and the risk of experiencing verbal or physical violence. But only one in three respondents said that they had been trained by their employer to deal with aggressive or violent disputes. No consideration was given to the extent and content of employee training and support. Studies and reviews are now available that deal with the effectiveness of training programmes in different healthcare sectors.38 ,45 ,46 It is not entirely clear as to whether training programmes can reduce the number of instances of violence, but cognitive knowledge and subjective confidence tend to have a positive effect on how staff cope with the experience of violence. However, due to a lack of high-quality studies there is huge scope for future research in this area. A recent study from Hahn et al39 investigated the management of patient and visitor violence in a general hospital. If the workplace had an official, organisational antiviolence strategy, healthcare staff felt more confident. But training in aggression management did not significantly influence the healthcare staff's feeling of confidence in dealing with patient violence. The authors stated that this could reflect the lack of appropriate training for the specific situations for healthcare workers in general hospitals. In line with these findings, 42% of healthcare workers in general hospitals had not received instructions and training compared with employees in residential homes for people with disabilities (11%) in our study.
Therefore, these findings support the importance of an adequate organisational strategy and appropriate training measures for specific working groups.
Limitations
With respect to the cross-sectional study design, no causal conclusion could be drawn. Another limitation is that a self-assessment of a 12-month period cannot rule out recall bias. That may have led to an overestimation of frequency, the severity of physical violence and its emotional and physical consequences. Mild violence may lead to underestimation. However, because of the self-reported data, there was no possibility of verifying the accuracy of the data. The low response rate is also a limitation of this study and reduces the ability to generalise the results. This is especially true for the general hospitals. Of the 230 facilities which the questionnaire was sent to, only 39 took part in the survey. Of the facilities that took part in the survey, the response rate was especially low in participating hospitals, at 25.5%. Presumably, only hospitals that were already particularly aware of the issue took part in the survey. That may have led, especially in hospitals, to the overrating of both the frequency of violence and the stress that it caused. In other studies, similar response rates were found, for example 31%47 and 38%.7 However, the topic of violence towards healthcare staff is a challenging research issue. Maguire et al47 stated that underreporting can be related to the professional socialisation of healthcare workers into an ethos of compliance and acceptance that their job is accompanied by bad but inevitable facets such as violence and aggression. In the study by Gates and colleagues, 65% of the emergency staff said that they never reported the incidents to the hospital authorities.48
For Germany, there has hitherto been little meaningful data on violence towards nursing and care staff except in psychiatric clinics. This study is intended first to generate some idea of how high the burden of violence experienced by nursing and healthcare staff and by employees in facilities for the disabled in Germany. Individual sectors are then to be examined in detail with a view to implementing interventions appropriate to the work area in question. It must, however, be borne in mind that the individual work areas differ widely in the burden of violence experienced, the factors that trigger it and the work situation, and cannot therefore be compared with each other.
Conclusion
Violence and aggression towards nursing and healthcare personnel occur frequently. Every third of the participant respondent feels severely stressed by violence and aggression. Occupational support provisions to prevent and provide aftercare for cases of violence and aggression reduce the risk of incidents and of perceived stress. However, only about a third of the respondents appear to receive adequate provision of support. Research is needed on occupational support provisions that reduce the risk of staff experiencing verbal or physical violence and the stress that is associated with it for the different settings. Our data also suggest the need for improved, target-group-specific prevention measures, as well as the effective implementation of aftercare to deal with the violence experienced by employees in the German healthcare and welfare systems.
References
Footnotes
-
Contributors AS, AZ, DW and AN designed the study, analysed and interpreted the data and drafted the manuscript. CW, MH and CP contributed to the study design, analysis and interpretation of the data. All authors had full access to all data in the study and take responsibility for the integrity of the data. AS, DW and AN are guarantors.
-
Funding This study was supported by the Institute for Statutory Accident Insurance and Prevention in the Health and Welfare Services, Hamburg, Germany. The funding source was not involved in the design, conduct or interpretation of the study or writing of the submitted work.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Hamburg.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.