History of breast feeding and risk of incident endometriosis: prospective cohort study
BMJ 2017; 358 doi: https://doi.org/10.1136/bmj.j3778 (Published 29 August 2017) Cite this as: BMJ 2017;358:j3778
- Leslie V Farland, research scientist1 2,
- A Heather Eliassen, associate professor1 3,
- Rulla M Tamimi, associate professor1 3,
- Donna Spiegelman, professor1 3,
- Karin B Michels, professor and chair1 4,
- Stacey A Missmer, professor1 5 6
- 1Department of Epidemiology, Harvard T.H. Chan School of Public Health, Boston, MA 02115, USA
- 2Center for Infertility and Reproductive Surgery, Department of Obstetrics, Gynecology, and Reproductive Biology, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA 02115, USA
- 3Channing Division of Network Medicine, Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, MA 02115, USA
- 4Department of Epidemiology, Fielding School of Public Health, University of California, Los Angeles, CA, USA
- 5Division of Adolescent and Young Adult Medicine, Department of Medicine, Boston Children’s Hospital and Harvard Medical School, Boston, MA 02115, USA
- 6Department of Obstetrics, Gynecology, and Reproductive Biology, College of Human Medicine, Michigan State University, Grand Rapids Michigan, MI 49503, USA
- Correspondence to: L V Farland lfarland{at}mail.harvard.edu
- Accepted 4 August 2017
Abstract
Objective To investigate the association between lifetime breast feeding, exclusive breast feeding, postpartum amenorrhea, and incidence of endometriosis among parous women.
Design Prospective cohort study.
Setting Nurses’ Health Study II, 1989-2011.
Participants 72 394women who reported having one or more pregnancies that lasted at least six months, 3296 of whom had laparoscopically confirmed endometriosis. For each pregnancy, women reported duration of total breast feeding, exclusive breast feeding, and postpartum amenorrhea.
Main outcome measures Incident self reported laparoscopically confirmed endometriosis (96% concordance with medical record) in parous women. Multivariable Cox proportional hazard models were used to calculate hazard ratios and 95% confidence intervals for diagnosis of endometriosis.
Results Duration of total and exclusive breast feeding was significantly associated with decreased risk of endometriosis. Among women who reported a lifetime total length of breast feeding of less than one month, there were 453 endometriosis cases/100 000 person years compared with 184 cases/100 000 person years in women who reported a lifetime total of ≥36 months of breast feeding. For every additional three months of total breast feeding per pregnancy, women experienced an 8% lower risk of endometriosis (hazard ratio 0.92, 95% confidence interval 0.90 to 0.94; P<0.001 for trend) and a 14% lower risk for every additional three months of exclusive breast feeding per pregnancy (0.86, 0.81 to 0.90; P<0.001 for trend). Women who breastfed for ≥36 months in total across their reproductive lifetime had a 40% reduced risk of endometriosis compared with women who never breast fed (0.60, 0.50 to 0.72). The protective association with breast feeding was strongest among women who gave birth within the past five years (P=0.04 for interaction). The association with total breast feeding and exclusive breast feeding on endometriosis was partially influenced by postpartum amenorrhea (% mediated was 34% (95% confidence interval 15% to 59%) for total breast feeding and 57% (27% to 82%) for exclusive breast feeding).
Conclusion Among women who experienced at least one pregnancy that lasted at least six months, breast feeding was inversely associated with risk of incident endometriosis. This association was partially, but not fully, influenced by postpartum amenorrhea, suggesting that breast feeding could influence the risk of endometriosis both through amenorrhea and other mechanisms. Given the chronic and incurable nature of endometriosis, breast feeding should be further investigated as an important modifiable behavior to mitigate risk for pregnant women.
Introduction
Endometriosis is a chronic gynecologic disorder diagnosed in about 10% of women in the US.123 Most affected women experience chronic pelvic pain, dysmenorrhea (painful periods), and dyspareunia (painful intercourse),45 and it has no known cure. Endometriosis lesions depend on circulating estrogen for growth and maintenance, and it is hypothesized that endometriosis etiology involves retrograde menstruation.46 While we are beginning to understand the risk profile for incidence of endometriosis, there are few known modifiable risk factors. Among parous women, breast feeding could have important implications as a modifiable risk factor for endometriosis.
The nutritional benefits of breast feeding for infants and the metabolic benefits for the mother are well known.78 The World Health Organization, the American College of Obstetricians and Gynecologist (ACOG), and the American Academy of Pediatrics (AAP) recommend that women breastfeed each child for at least 12 months with six months of exclusive breast feeding (breast feeding without the introduction of solid food or formula).8910 Emerging research has found lasting benefits of breast feeding for long term maternal health, including help in weight loss and reduction in risk of chronic disease, including breast cancer and ovarian cancer.71112 Breast feeding could alter risk of maternal disease by prolonging amenorrhea, promoting circulating levels of oxytocin and prolactin, and inhibiting circulating gonadotropins.13
Despite the plausible mechanism for an association between breast feeding and endometriosis, to our knowledge research on this topic is restricted to two studies, one previously conducted by our team in this cohort. Previous research has been limited by crude, cross sectional measures of duration of breast feeding, small sample size, and short follow-up.1415 Our current analysis followed women for over 20 years, 14 additional years from the previous study, and leverages detailed lifetime history of breast feeding applied to each pregnancy to investigate more thoroughly the relation between the duration of total breast feeding, as well as exclusive breast feeding and postpartum amenorrhea, and risk of endometriosis. We hypothesized that among women who have experienced pregnancy, duration of breast feeding would protect against risk for endometriosis, with duration of exclusive breast feeding and postpartum amenorrhea conferring the strongest protective effect.
Methods
The Nurses’ Health Study II (NHSII) is a prospective cohort study that began in 1989, when 116 430 registered nurses aged 25-42 returned a mailed questionnaire on their health and lifestyle. Follow-up questionnaires that collect information on environmental, dietary, and lifestyle risk factors have been sent every two years, with cumulative follow-up rates ≥90%.
Definition of exposure
Since 1989, participants have reported all pregnancies (lasting at least six months) every two years. In 1993, women were asked about lifetime history of breast feeding. In 1997, women were asked detailed information on their history of breast feeding and duration for each of their first four children, as described elsewhere.16 Women with more than four children were asked to report combined breast feeding information for each additional child. A supplementary questionnaire was sent to women reporting pregnancies subsequent to 1997 so that information on duration of breast feeding could be collected to 2003 (at which point the youngest participant was 39). The combination of detailed child specific information on duration of breast feeding with the annual information on pregnancy history allows us to update history of breast feeding over time.
To estimate total duration of breast feeding, women were asked, “If you breastfed, at what month did you stop breast feeding altogether?” and were given the following categories: “1-2 months, 3-5 months, 6-8 months, 9-11 months, 12-18 months, ≥19 months.” To approximate duration of exclusive breast feeding, women were asked “At what month did you start giving formula or purchased milk at least once daily?” and “At what month did you start giving solid food at least once daily (baby food, cereal, table food, etc)?” and could respond “0-2 months, 3 months, 4-5 months, 6-7 months, 8-11 months, ≥12 months.” We defined duration of exclusive breast feeding as the earlier of these two time points. Lastly, to quantify postpartum amenorrhea, women were asked “At what month after delivery did your menstrual periods return?” and were given the following categories: “1-2 months, 3-5 months, 6-9 months, ≥10 months, pregnant again, or never.” Our derived exposures of breast feeding and amenorrhea were updated every two years and were summed across reproductive history. To create a continuous variable of duration of breast feeding, women were assigned the mid-point of the reported category. Women in the highest category of total breast feeding were assigned 45 monthsand women in the highest category of exclusive breast feeding were assigned 20.5 months.
Definition of outcome
We defined our outcome as laparoscopically confirmed endometriosis. On the 1993 questionnaire, women were first asked if they had ever had “physician diagnosed endometriosis.” If they answered “yes,” they were asked to report when the diagnosis had occurred and if their disease had been confirmed by laparoscopy. Diagnosis has been assessed on every subsequent questionnaire since 1993.
We previously used medical records to validate self reported endometriosis among 200 participants who reported diagnoses of endometriosis in 1993.314 Among women who reported laparoscopic diagnosis of endometriosis, this was confirmed in 96% of medical records. Conversely, among those women without laparoscopic confirmation, evidence of clinical diagnosis was found in only 54% of medical records. Thus, to reduce the magnitude of misclassification, we restricted cases of endometriosis to those women with laparoscopic confirmation. Women who reported a diagnosis without laparoscopic confirmation and who then later had confirmation by laparoscopy were assigned to the endometriosis case group at the time of the initial clinical diagnosis. Those who reported a diagnosis of endometriosis but never received laparoscopic confirmation were censored at the report of clinical diagnosis.
Study population
Cohort participants were included in this analysis population from first report of pregnancy through the 2011 questionnaire cycle (n=72 394) (fig 1⇓). We excluded women who reported a diagnosis of endometriosis or cancer (other than non-melanoma skin cancer) before June 1989 (n=5389). We calculated person months at risk from report of first pregnancy lasting at least six months until confirmed death, cancer (other than non-melanoma skin cancer), postmenopausal status, hysterectomy, laparoscopically confirmed endometriosis, or loss to follow-up. Women who remained nulliparous until the end of follow-up did not contribute person time to the analyses. Because history of breast feeding was last collected in 2003, we did not include the 108 women who reported a first pregnancy after 2003, when participants were aged 39-56.

Fig 1 Population under study from Nurses’ Health Study II cohort
{kind=link}
Statistical analyses
We used Cox proportional hazard models, stratified by calendar time with age (months) as the time metameter, to calculate the hazard ratios and 95% confidence intervals for endometriosis. We tested the proportional hazard assumption using a likelihood ratio test for the created interaction term between our exposure (breast feeding) and the time metameter, age (months),17 and this assumption was found not to be violated. A priori hypothesized risk factors for endometriosis were adjusted for, and time varying covariates were updated biennially at every questionnaire cycle: current BMI (<18.5, 18.5-22.4, 22.5-24.9, 25-29.9, ≥30, time varying), BMI at age 18 (<18.5, 1.5-22.4, 22.5-24.9, 25-29.9, ≥30), history of smoking (never, former, current, time varying), use of oral contraceptives (never, former, current, time varying), pregnancies lasting at least six months (1, 2, ≥3 pregnancies, time varying), age at menarche (<12, 12, 13, 14, >14), history of infertility (unable to get pregnant for ≥12 months, time varying), and time since last birth (<5, 5-10, >10 years, time varying). For variables with missing data, we created missing indicator variables.
Our main analysis categorized duration of total breast feeding (<1 (reference), 1-<3, 3-<6, 6-<12, 12-<18, 24-<36, ≥36 months) and exclusive breast feeding (<1 (reference), 1-<3, 3-<6, 6-<12, 12-<18, ≥18 months). We used missing indicator variables for women with missing information on duration of breast feeding (1.3% of women with endometriosis had information missing on total breast feeding; 7.1% of women with endometriosis had information missing on exclusive breast feeding). We examined the possibly non-linear relation between total breast feeding and exclusive breast feeding and the relative risk of endometriosis non-parametrically with restricted cubic splines.18 Tests for non-linearity used the likelihood ratio test, comparing the model with only the linear term with the model with the linear and the cubic spline terms. The differences represent extremes in duration of breast feeding. Analyses were performed with SAS version 9.3 (SAS Institute, Cary, NC).
Sensitivity analyses
We were interested in testing whether the relation between breast feeding and endometriosis differed between subgroups that were selected a priori. As previous analyses in this cohort reported a stronger magnitude of association between breast feeding and endometriosis within five years of pregnancy,14 we stratified our analysis by time since last reported birth (≤5 or >5 years). Additionally, we assessed whether the association between breast feeding and risk of endometriosis differed by age at first birth (<30, 30-35, >35), history of infertility (ever attempting to conceive for ≥12 months without success), number of pregnancies lasting at least six months (1, 2, ≥3), and BMI (<18.5, 1.5-22.4, 22.5-24.9, 25-29.9, ≥30). In previous studies of endometriosis, there has been concern about a lengthy delay between onset of symptoms and surgical diagnosis. In the Nurses’ Health Study, the average delay was about four years,14 while international multicenter studies have observed an average delay of seven years, attributable to a delay in specialist referral by primary care physicians.19 Thus, this interval from symptom onset to diagnosis could vary based on physician referral patterns or recognition in primary care of disease in adolescence. To investigate the effect of this temporal misclassification of exposure, we set the diagnostic date of endometriosis earlier by two, four, and six years. To investigate the influence of medications to suppress lactation, we restricted analyses to women who never reported use of medications (pills and injections) to suppress lactation.
Amenorrhea is inversely associated with risk of endometriosis,1420 and amenorrhea postpartum can be influenced by duration and intensity of breast feeding.721 To further elucidate how the components of breast feeding influence risk of endometriosis, we considered postpartum amenorrhea as a potential mediator of breast feeding and risk. Using the difference method, we calculated the percentage and 95% confidence interval of the effect estimates of total lifetime breast feeding and exclusive lifetime breast feeding that were mediated by postpartum amenorrhea.22 We did this by comparing models adjusted and not adjusted for amenorrhea using mediation tools described by Lin and colleagues.232425
Patient involvement
No patients were involved in setting the research question or the outcome measures, nor were they involved in developing plans for recruitment, design, or implementation of the study. No patients were asked to advise on interpretation or writing up of results. Results of the study will be disseminated to patients’ organizations and through the webpage of the Nurses’ Health Study (http://www.nurseshealthstudy.org).
Results
At baseline in 1989, women who reported a longer duration of total breast feeding tended to be older, multiparous, and have never smoked or used oral contraceptives (table 1⇓). Such women were also less likely to be currently overweight or obese, overweight or obese at age 18, and to report earlier age at menarche. From 1989 until return of the 2011 questionnaire, women who reported having pregnancies lasting at least six months were followed, and there were 3296 laparoscopically confirmed cases of endometriosis (fig 1⇑).
Characteristics of women in Nurses’ Health Study II at baseline (1989) by breast feeding status. Figures are percentages* unless stated otherwise
Compared with women who breastfed for less than a month in total (453 endometriosis cases/100 000 person years), women who breastfed ≥36 months in total across her reproductive life (184 endometriosis cases/100 000 person years) had a 40% reduced risk of a diagnosis of endometriosis (hazard ratio 0.60, 95% confidence interval 0.50 to 0.72). Attenuation between age adjusted and multivariable adjusted models was driven primarily by adjustment for the number of pregnancies that lasted at least six months. We observed a significant inverse linear relation between duration of lifetime total breast feeding and risk of endometriosis (P<0.001 for linear trend). For every additional three months of lifetime total breast feeding among women (up to 45 months), we observed a 3% reduction in risk of endometriosis (3 month increase hazard ratio 0.97, 0.96 to 0.97) (table 2⇓, fig 2⇓).
Relative risk of laparoscopically confirmed endometriosis by cumulative history of breast feeding in Nurses’ Health Study II
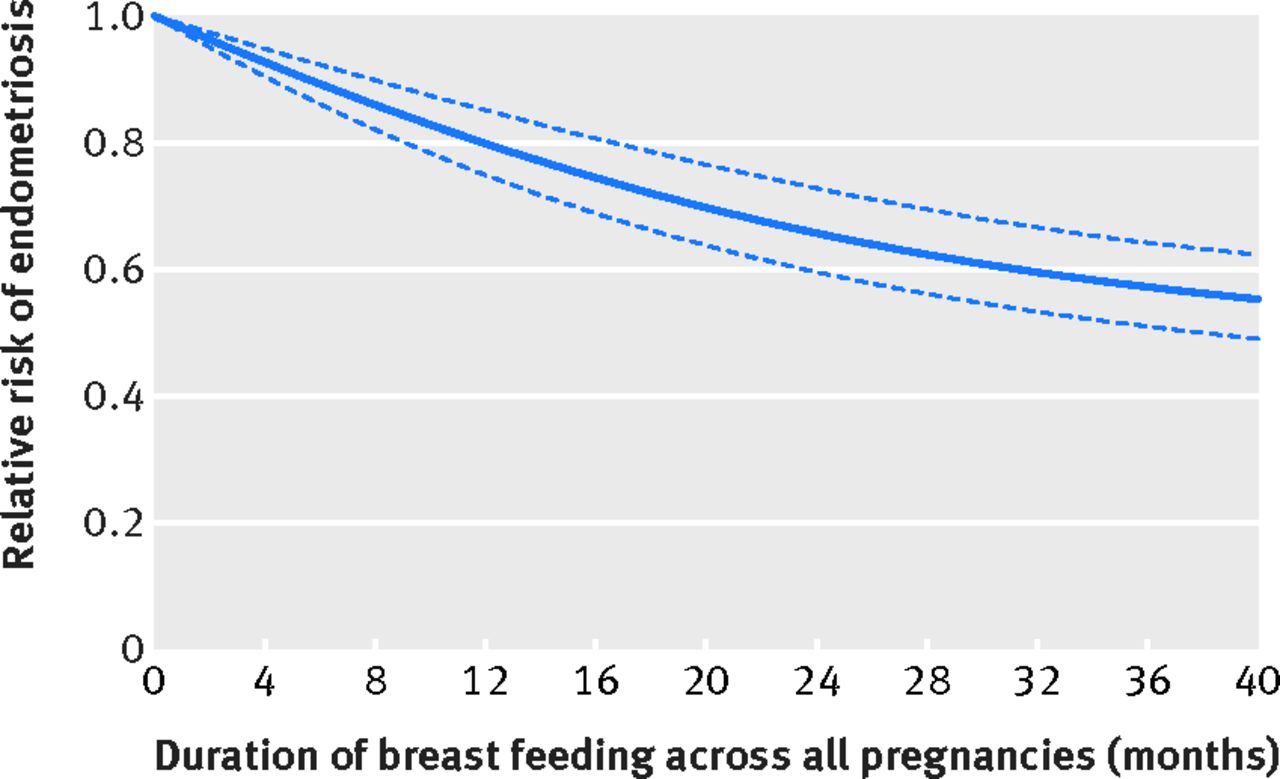
Fig 2 Relative risk of endometriosis by history of total breast feeding across woman’s lifetime, stratified by calendar time with age as time metameter (months), additionally adjusted for current BMI, BMI at age 18, history of smoking, history of use of oral contraceptive, pregnancies lasting at least six months, age at menarche, history of infertility, and time since last birth (reference value=0 months)
{kind=link}
Compared with women who did not breast feed exclusively (413 endometriosis cases/100 000 person years), women who did so for 18 months or more across their reproductive lifetime (199 endometriosis cases/100 000 person years) had nearly a 30% reduced risk for endometriosis (hazard ratio 0.73, 95% confidence interval 0.58 to 0.91). In models that used restricted cubic splines, the relation between exclusive breast feeding and endometriosis seemed non-linear (P=0.01 for non-linearity) but remained significant (P=0.001 for overall significance of curve) (fig 3⇓).

Fig 3 Relative risk of endometriosis by exclusive breast feeding history across a woman’s lifetime, stratified by calendar time with age as time metameter (months), additionally adjusted for current BMI, BMI at age 18, history of smoking, history of use of oral contraceptive, pregnancies lasting at least six months, age at menarche, history of infertility, and time since last birth (reference value=0 months)
{kind=link}
We then evaluated the pregnancy specific impact of breast feeding. For each pregnancy, a three month increase in average duration of total breast feeding was associated with an 8% reduction in risk of endometriosis (hazard ratio 0.92, 95% confidence interval 0.90 to 0.94; P<0.001 for linear trend; table 3⇓). For each pregnancy, a three month increase in average duration of exclusive breast feeding per pregnancy was associated with a 14% decreased risk of endometriosis (0.86, 0.81 to 0.90; P<0.001 for trend).
Relative risk of laparoscopically confirmed endometriosis by history of breast feeding per pregnancy in Nurses’ Health Study II
Postpartum amenorrhea was also inversely associated with risk of endometriosis. Compared with women who had never experienced amenorrhea postpartum, women who had postpartum amenorrhea for 6-12 months across her reproductive lifetime had a decreased risk of endometriosis (hazard ratio 0.58, 95% confidence interval 0.50 to 0.68; P<0.001 for linear trend; table 4⇓). These patterns were consistent when we investigated the influence of postpartum amenorrhea on average per pregnancy (table A in appendix). Postpartum amenorrhea was a significant contributor to the association between total lifetime breast feeding and risk of endometriosis (% mediated 34%, 95% confidence interval 15% to 59%) and of the association between exclusive lifetime breast feeding overall and risk, if we assume a linear relation between exclusive breast feeding and endometriosis (% mediated 57%, 27% to 82%). Even after we accounted for postpartum amenorrhea, however, both lifetime total breast feeding (hazard ratio per three month increase 0.98, 95% confidence interval 0.96 to 0.99) and exclusive lifetime breast feeding (0.97, 0.95 to 1.00) remained associated with a lower risk for endometriosis (consistent with results presented in table 2⇑) (table B in appendix).
Relative risk of laparoscopically confirmed endometriosis by history of amenorrhea in Nurses’ Health Study II
While the inverse association between breast feeding and risk of endometriosis was stronger in women who gave birth within the past five years (P=0.04 for interaction; hazard ratio per three month increase 0.95, 95% confidence interval 0.93 to 0.97), the association was attenuated but remained significant even after five years since last birth (0.97, 0.96 to 0.98). In multivariate adjusted models, we found no differences in models stratified by BMI, age at first birth, number of pregnancies, or infertility status. Similar patterns were seen when we restricted analysis to uniparous women (table C in appendix). In sensitivity analyses predating diagnosis of endometriosis by two, four, and six years, and restricted to women who did not use drugs to suppress lactation, the overall patterns between breast feeding and endometriosis did not vary (results not shown).
Discussion
Principal findings
Breast feeding overall, as well as exclusive breast feeding, is associated with a lower risk of endometriosis. For each pregnancy, women who did not breast feed were at a significantly increased risk of endometriosis compared with women who followed the recommendations from the American College of Obstetricians and Gynecologists and American Academy of Pediatrics of breast feeding for at least one year. While we observed heterogeneity in the strength of the association by time since last birth, breast feeding consistently was protective in all groups of women. Part of the inverse association between lifetime total breast feeding duration and risk of endometriosis could be attributed to postpartum amenorrhea.
Comparison with other studies
Our findings confirm previous reports of an inverse relation between breast feeding and risk of endometriosis.1415 In previous research within our cohort, with six years of follow-up and 448 incident cases, we reported a significant relation between a one time measure of lifetime duration of breast feeding and endometriosis (P=0.008 for linear trend).14 Women who reported breast feeding for an overall total of more than 23 months were at a significantly decreased risk of endometriosis compared with women who reported never breast feeding (hazard ratio 0.7, 95% confidence interval 0.5 to 1.0). We found, however, that the inverse relation was evident only within the five years since the last birth (P<0.001 for heterogeneity). Heilier and colleagues also found a protective association of “ever” versus “never” breast feeding in a case-control setting, though their sample size was limited (88 women with endometriosis), and they did not adjust for parity or other confounding factors.15 While these earlier investigations used crude, cross sectional measures of lifetime breast feeding, and had limited numbers of women with endometriosis, our current analysis incorporated detailed time varying information on breast feeding for each individual pregnancy and had over 20 years of follow-up for this large cohort of women (with 3296 incident cases of endometriosis). We also expanded the definition of breast feeding to investigate total and exclusive breast feeding, as well as adding an investigation of the impact of postpartum amenorrhea.
Duration of total breast feeding and exclusive breast feeding were associated with a reduced risk of endometriosis, with a significant proportion of the reduction in risk accounted for by postpartum amenorrhea (34% and 57%, respectively). The most common and supported etiologic theory for onset of endometriosis, “Sampson’s theory,” posits that endometriosis is caused or at least initiated by retrograde menstruation.6 Thus, the more menstrual periods a woman experiences, the greater her exposure to retrograde menstruation and therefore the greater the risk for developing endometriosis. Our analysis lends support to this theory. We found that longer duration of postpartum amenorrhea was associated with a significantly decreased risk of endometriosis and was an important mediator of the association of total and exclusive lifetime breast feeding.
An estimated 90% of women experience retrograde menstruation,26 which suggests that the true differences between women with and without endometriosis might be caused by factors that influence adherence, proliferation, and maintenance of the cells and lesions not only retrograde menstruation. Alternatively, there could be a component of the pathways that initiate and support the return of menses postpartum that are also implicated in the pathophysiology of endometriosis. These pathways might or might not overlap with the well established association between earlier age at menarche and increased risk of endometriosis.1427
We found that the inverse association between total and exclusive breast feeding and risk of endometriosis could not be fully explained by taking into account duration of postpartum amenorrhea. Aside from regulating amenorrhea, which could influence retrograde menstruation, breast feeding is known to increase concentrations of circulating oxytocin and inhibit circulating concentrations of estrogen, gonadotrophin releasing hormone, luteinizing hormone, and follicle stimulating hormone. Breastfeeding women in whom menstruation has not restarted have lower concentrations of circulating estradiol than women with normal cycles.28 While little is known regarding the duration of hormonal and inflammatory changes once breast feeding ceases, that breast feeding could be associated with lower risk has biologic plausibility. Moreover, breast feeding has been found to be associated with lower risk of other chronic diseases, including breast cancer,71112 ovarian cancer,7 and type two diabetes,716 through similar hypothesized mechanisms of altered circulating hormones and prolonged amenorrhea.13
Strengths and limitations of the study
Despite the strengths of our investigation, our findings also have some limitations. Misclassification of history of breast feeding is possible as women were asked retrospectively to report their experience. Previous research indicates that women can accurately report their breast feeding for up to 20 years after index birth (r=0.82 for continuous duration of recalled breast feeding compared with continuous duration reported on medical records),29 which implies that the likelihood for misclassification from recall is minimal. We would expect women with and without endometriosis to recall their duration of breast feeding similarly. Additionally, if women reported more than four pregnancies on our questionnaire, they were asked to sum duration of lactation across five or more pregnancies (2.8% of pregnancies in 2003), which could lead to misclassification. To estimate potential mediation by postpartum amenorrhea we had to assume a linear relation between exclusive breast feeding and risk of a diagnosis of endometriosis, which could be an oversimplification of the distribution of the relation. This analysis prospectively investigated the relation between duration of breast feeding and risk of endometriosis after pregnancy and, in doing so, did not include women with a diagnosis of endometriosis before their first reported pregnancy or women with endometriosis before study follow-up (n=5389). While this strengthens our findings, we cannot generalize our findings to women with endometriosis diagnosed before pregnancy as their risk could not be affected by breast feeding. We also did not differentiate singleton and multiples pregnancies; only 1.7% of women, however, reported twins or higher order multiples. Our findings might not be applicable to women with infertility who remained nulliparous. Because of a potential delay in diagnosis of endometriosis, some women in our cohort might have asymptomatic disease or disease that has not yet been diagnosed. As the prevalence of endometriosis is believed to be about 10%, the inclusion of women with undiagnosed endometriosis in the non-case group (about 62 000) would likely have a limited effect30 among the large number of women in this cohort who genuinely did not have endometriosis. We explored diagnostic delay more thoroughly through the sensitivity analyses that predated diagnosis of endometriosis by two, four, and six years. This did not materially alter our results. Women with endometriosis might also have disordered pain perception that could influence duration of breast feeding. Our study did not collect detailed information on pain sensitization, and this mechanism should be investigated more thoroughly in future work. We also did not collect detailed information on location or staging of the endometriosis lesions, which could represent disease heterogeneity, although stage has consistently been found not to be correlated with severity of pain or infertility.
To our knowledge, this is the largest study to prospectively estimate the association with breast feeding and the first study to estimate the components of breast feeding on risk of endometriosis. With over 20 years of follow-up and validated measurement of endometriosis, our study is well powered to estimate risk. Additionally, the study’s time varying and detailed estimates of duration of breast feeding across the entire history of reproduction in these women, as well as detailed information on postpartum amenorrhea, gives us a clearer understanding of the public health importance of breast feeding as a modifiable risk factor for endometriosis risk among parous women.
Conclusions and policy implications
Endometriosis is a chronic disease with no known cure and debilitating symptoms. At present, few modifiable risk factors are known to prevent its occurrence. Future research should investigate breast feeding as a mechanism for mitigation of symptoms among women with a diagnosis of endometriosis. The strong inverse relation we found between duration of breast feeding and risk might have important clinical implications for advising women to modify their risk profile for endometriosis. Our findings lend support to the body of public health and policy literature that advocates for the promotion of breast feeding. All women should be counseled regarding the health benefits of breast feeding for both the mother and child, systems level policy changes should be implemented to encourage breast feeding, and future research should investigate the benefit of breast feeding among women diagnosed with endometriosis for symptom control.
What is already known on this topic
Few modifiable risk factors for endometriosis are currently known
Despite the plausible mechanism for an association between duration of breast feeding and risk of endometriosis, research on this topic is restricted to studies with crude cross sectional measures of duration of breast feeding, small sample sizes, and short duration of follow-up
What this study adds
Duration of breast feeding is inversely associated with risk of endometriosis
The findings give further support to the importance of counseling women regarding the health benefits of breast feeding for both the mother and child
Footnotes
We thank the participants and staff of the Nurses’ Health Study II for their valuable contributions. The authors assume full responsibility for analyses and interpretation of these data. An abstract of this work was presented as an oral presentation at the annual meeting of the 13th World Congress on Endometriosis in May 2017.
Contributors: LVF, SAM, RMT, AHE, and DS were responsible for study concept and design. LVF analyzed the data and wrote the manuscript, while all authors critically reviewed the manuscript and approved the final version. All authors also had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. LVF is guarantor.
Funding: This work was supported by National Institutes of Health, National Cancer Institute (UM1 CA176726, 3R25CA057711 to LVF), National Institute of Child Health and Human Development (HD57210, T32HD060454 to LVF), and the Dana Farber and Harvard Cancer Center Mazzone Award. The NIHR had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. The views expressed in this publication are those of the authors and not necessarily those of the funding agencies.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: support from the Harvard T H Chan School of Public Health, Eunice Kennedy Shriver National Institute of Child Health and Human Development, and National Cancer Institute for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: The study was approved by the institutional review board at Brigham and Women’s Hospital and Harvard medical school.
Data sharing: No additional data available.
Transparency: The lead author affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.