Article Text

Statistics from Altmetric.com
Description
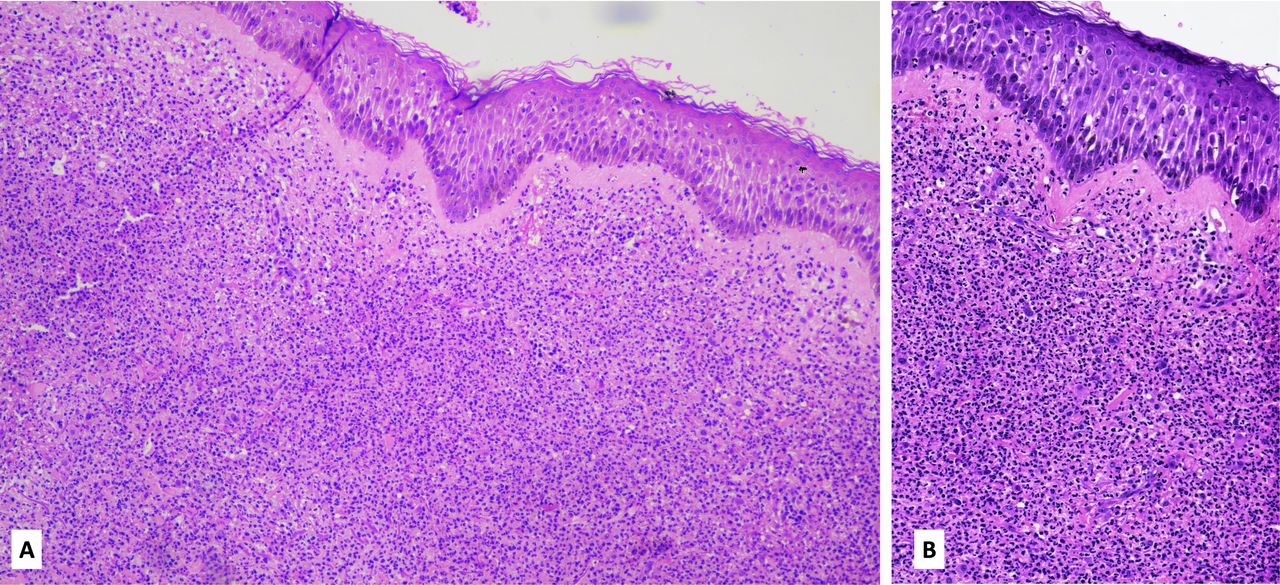
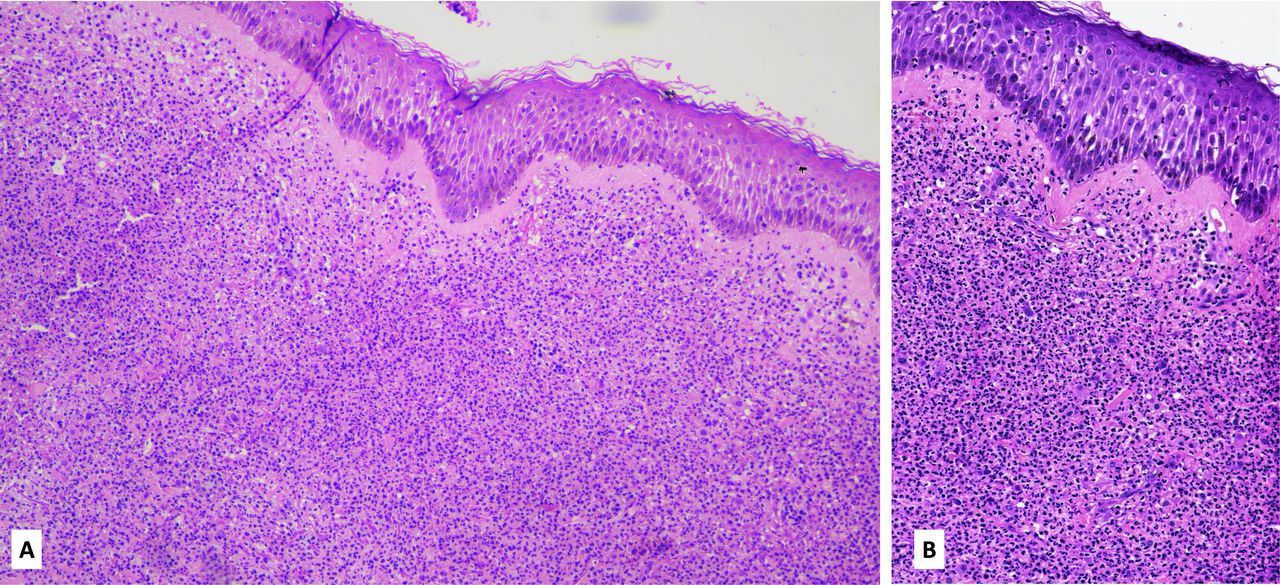
A woman in her 70s presented to the dermatology outpatient department with painful plaques over the trunk and a fever for the past 5 days. She was diagnosed with acute myeloid leukaemia (AML) in view of cytopenia (haemoglobin (Hb) 57 g/L; total leucocyte count 0.99 x 109/L; differential leucocyte counts of neutrophils 13.2%, lymphocytes 84.8% and monocytes 2%; platelet count 330 000/mm3) and confirmed by bone marrow biopsy 5 months ago. She was on tab. azacytidine 300 mg two times per day until then. After 4 months her clinical symptoms and haematological parameters improved (Hb 9.4 g/dL; total leucocyte count 4910/mm3; platelet count 350 000/mm3), but she started to develop skin lesions. There were well-defined, round to oval (5 cm × 5 cm), erythematous, oedematous, tender plaques with central crusting over the right upper back (figure 1A) and abdomen (figure 1B). Histopathology of the trunk lesion revealed a zone of oedema in the upper dermis, beneath which dense neutrophilic infiltrate was admixed with histiocytes and karyorrhexis (figure 2). A final diagnosis of Sweet’s syndrome (SS) was suspected. It was unusual despite improvement in haematological parameters of AML which led to the possibility of an azacytidine-induced SS. Later, azacytidine was replaced by six mercaptopurine (50 mg three times a week) after consultation with medical oncology services. Oral prednisolone (0.5 mg/kg) was prescribed to treat the neutrophilic dermatosis. She had resolution of the lesions in 2 weeks’ time; the prednisolone dose was tapered gradually and stopped in the next 2 weeks. There was no recurrence of the lesions at 3 months of follow-up.

Erythematous, oedematous plaque over upper back (A) and abdomen (B) with central bullae formation.
{kind=link}
{kind=link}
Upper dermal oedema and dense neutrophilic infiltrate throughout the dermis (A) H&E 100×, higher magnification image showing dense neutrophilic infiltrate and karyorrhexis (B) H&E 200×.
The malignancy-associated SS accounts for 15%–20% of total cases of SS and is associated with both haematological and visceral malignancies.1 In this setting, AML constitutes the most reported cases. It occurs in about 1% of the patients with AML.2 SS induced by azacytidine is rare in literature. The time interval between initiation of azacytidine and appearance of clinical lesions of SS varies from 5 days to 9 months.3 4 Though most of the previous reports are with subcutaneous injection of azacytidine, it was following oral administration in our case.
The typical skin lesions supported by the classical histopathological picture were confirmatory for the diagnosis of SS. The temporal correlation of the appearance of those lesions following administration of azacytidine and no recurrence after discontinuation of the drug suggested a drug-induced aetiology.
Patient’s perspective
My mother was ill with haematological malignancy, but the new onset painful eruption was troublesome. It was picked early and treated accordingly. The painful lesions didn’t recur after stopping the suspected drug. Though the prognosis of the actual disease was discussed and explained to us, the relief from the painful lesions was helpful. (Patient’s daughter)
Learning points
Azacytidine is a rare cause of drug-induced Sweet’s syndrome and should be suspected in patients of acute myeloid leukaemia who are on azacytidine along with the disease itself.
The incubation period is usually 2–4 months for azacytidine-induced Sweet’s syndrome.
Short course of systemic steroid is usually enough along with substitution of the causative agent.
Ethics statements
Patient consent for publication
Footnotes
Contributors All the authors have contributed to the preparation of the manuscript. PW and SP were responsible for the dermatology portion. BT has written the pathology portion, and SB is responsible for the medical oncology part.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.