Article Text

Abstract
Laparoscopic pancreatoduodenectomy (LPD) is increasingly performed worldwide as an alternative to the open conventional method, with the aim of advancing recovery. Because of its recent introduction, little is known about late surgical complications from this procedure. Here, we describe a case of a 76-year-old woman who underwent LPD with end-to-side gastrojejunostomy and presented with pain in the right upper quadrant of the abdomen 6 months thereafter. CT showed signs of an internal herniation. Elective diagnostic laparoscopy demonstrated a hernia of the efferent loop in Petersen’s space. The loop was repositioned and Petersen’s space was closed. The patient was discharged on the same day. Apart from a short readmission for nausea and vomiting, which were managed conservatively, the patient recovered without any further complications. Internal herniation should be considered in patients with abdominal complaints following LPD.
- gastrointestinal surgery
- pancreas and biliary tract
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Laparoscopic pancreatoduodenectomy (LPD) is increasingly conducted over the last decade and is, when performed in expert centres, possibly associated with a decreased length of stay and reduced intraoperative blood loss.1 Research on this novel procedure is mostly focused on safety and complications early in the postoperative period, but data on long-term surgical outcome is limited. The current report describes a patient with pain in the right upper abdomen caused by a Petersen’s internal herniation following LPD.
Case presentation
A 76-year-old woman with a history of rheumatoid arthritis, left hip replacement, laparoscopic cholecystectomy and hysterectomy presented with jaundice, abdominal pain and weight loss at our hospital. Endoscopic retrograde cholangiopancreatography revealed a stenosis in the common bile duct and subsequent biopsies ascertained adenocarcinoma. CT did not show any signs of metastases, after which the patient underwent an LPD with end-to-side gastrojejunostomy. No perioperative complications occurred and the patient was discharged 9 days after surgery. After 6 months during a regular check-up, the patient was experiencing recurrent abdominal pain without nausea and dysphagia.
Investigations
An abdominal contrast CT (video 1) showed swirl of superior mesenteric artery and vein (figure 1), torsion of small bowel and venous congestion (figure 2).

CT abdomen showing swirl of the superior mesenteric artery and vein.

CT abdomen showing congestion of the superior mesenteric vein (arrow).
Treatment
An elective laparoscopy was planned 2 weeks following the CT scan since no acute symptoms were present. During laparoscopy, a herniation of the efferent loop in Petersen’s space was observed (figure 3). No bowel ischaemia was present. The hernia was repaired and the mesenteric defect was closed with sutures afterwards (figure 4).

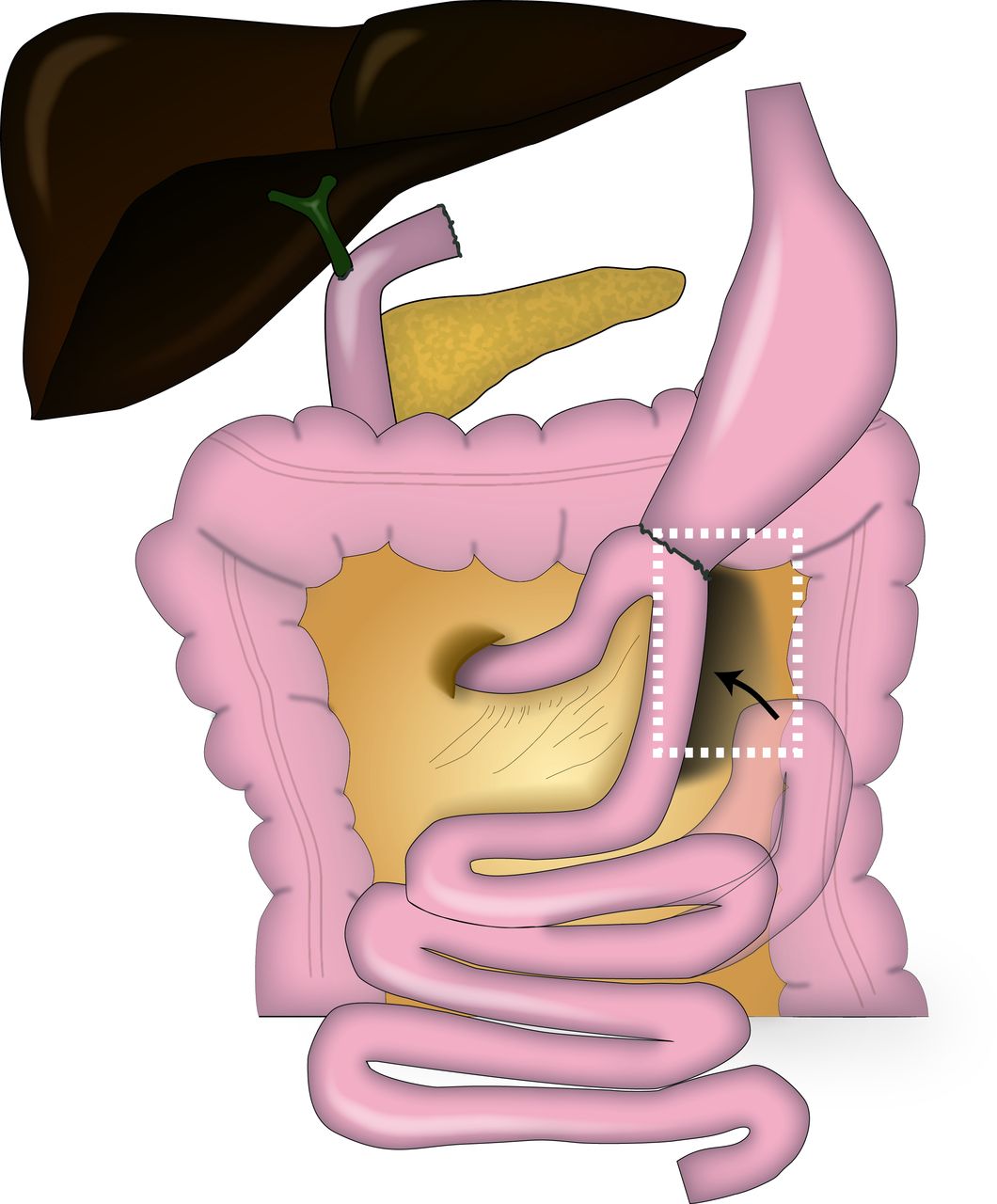
Schematic presentation of this case. Following laparoscopic pancreatoduodenectomy, with the creation of a hepaticojejunostomy, pancreaticojejunostomy and gastrojejunostomy, an intestinal loop has herniated (arrow) in the space posterior to the gastrojejunostomy (Petersen’s space, highlighted in white box). Image created by Anne Ten Hove and David Brinkman.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Closure of the mesenteric defect during laparoscopy.
Outcome and follow-up
The patient recovered quickly and was discharged on the same day as the operation. After 3 days, the patient was readmitted because of nausea and vomiting, which was most likely related to gastroparesis. Due to effective conservative treatment with a nasogastric tube and enemas, the patient recovered and could be discharged after 3 days.
Discussion
Pancreatoduodenectomy remains the only curative treatment for (pre)malignant tumours in the periampullary region. As in other types of abdominal surgery, a laparoscopic approach could improve recovery and possibly reduce length of stay.1 Due to its recent introduction, studies have focused on short-term surgical outcome, while little is known on late complications following LPD.
Internal herniation is an occasional but potentially life-threatening complication following abdominal surgery with an incidence between 1.1% and 6.1% after laparoscopic gastric bypass surgery.2–4 Although internal herniation is predominantly described in bariatric surgery, it is rarely seen following (open) pancreatoduodenectomy. In fact, only two studies have reported a case of internal herniation following open pancreatoduodenectomy.5 6 For robotic-assisted pancreatoduodenectomy, a recent study found internal herniation in 5 out of 192 cases (2.6%). Patients in this study presented with symptoms such as nausea, vomiting or merely vague abdominal pain.7 Thus far, no cases of internal herniation have been reported following LPD, but a similar incidence of internal herniation could be expected as observed after robotic surgery.
Closure of the mesenteric defect has been proposed as a method to prevent internal herniation. Indeed, a meta-analysis demonstrated that closure of the defects was associated with a decreased incidence of internal herniation following laparoscopic bypass surgery, which was confirmed in a randomised controlled trial.8 9 Closure also appears to have a preventive effect in robotic-assisted pancreatoduodenectomy.7 Using surgical videos, Qin et al found the incidence of internal herniation to be 0% after closure of the mesenteric defect (0/31) compared with 63% (5/8) when the mesenteric defect was left untreated. Although it could provoke early small bowel obstruction, closure of the mesenteric defect should be considered during LPD to prevent internal herniation.
In summary, this report describes an internal herniation following LPD, which was successfully treated laparoscopically by repositioning the hernia and closure of the defect in Petersen’s space. This diagnosis should be considered in patients with abdominal complaints following LPD.
Learning points
Internal herniation should be considered in patients presenting with abdominal complaints following laparoscopic pancreatoduodenectomy (LPD).
Patients with an internal herniation do not always present with nausea and vomiting.
Closing of mesenteric defects during the initial surgical procedure might prevent internal herniation following LPD.
Supplementary video
Footnotes
Contributors MDL has treated the patient. DJB drafted the manuscript. DJB, JVH and MDL critically revised the manuscript. All authors approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.