Article Text

Statistics from Altmetric.com
Description
Acute airway obstruction is a common ENT emergency with a wide range of aetiologies. The most common causes are infection, malignancy and foreign bodies, but more unusual causes should be considered.1
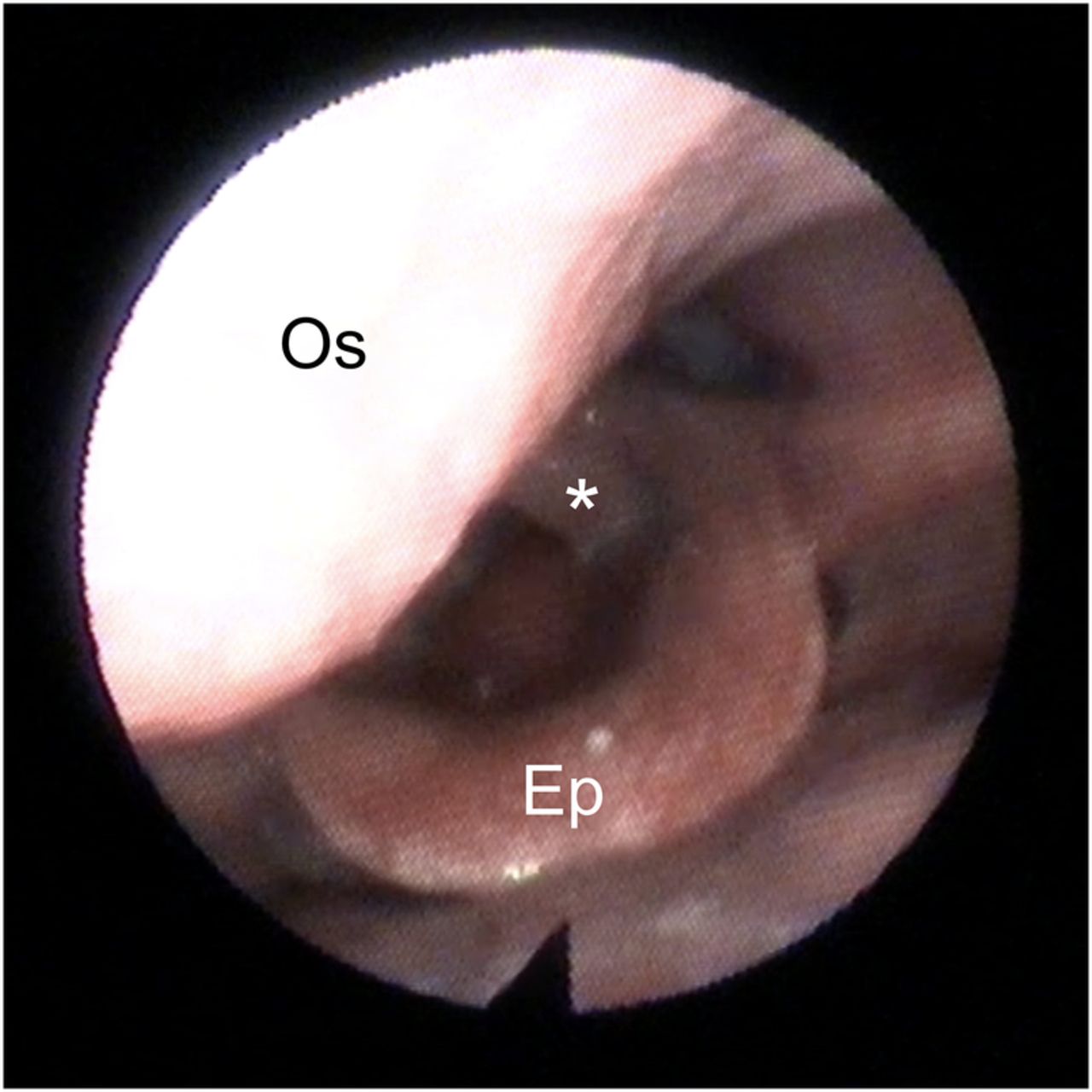
A 77-year old gentleman presented to the emergency department with worsening difficulty in breathing for 3 months since undergoing spinal surgery for multilevel cervical myelopathy. He of stertor, cough, dysphagia and intermittent apnoea. He was otherwise systemically well with no clinical signs of sepsis. Flexible nasendoscopy revealed a large posterior pharyngeal wall mass obscuring the glottis (figure 1).

Flexible nasendoscopy demonstrating a large posterior pharyngeal mass protruding into the airway resulting in narrowing of the glottic inlet as well as supraglottic oedema (Os, osteophyte compressing the posterior pharyngeal wall; Ep, epiglottis; *vocal fold demonstrating glottic oedema).
CT of the neck revealed a large confluence of osteophyte formation from C2 to C5, protruding into and distorting the posterior pharyngeal wall and larynx, resulting in narrowing of the glottic inlet (figure 2). The patient underwent an emergency tracheostomy in order to secure the airway. During the procedure, bone cutters were required to create the tracheal window due to severe calcification of the trachea. Once stabilised, he was transferred to a neurosurgical centre for surgical osteophytectomy.

{kind=link}
{kind=link}
CT scan of the neck (A, sagittal view; B, axial view) demonstrating a large cervical osteophyte compressing the posterior pharyngeal wall resulting in narrowing of the airway.
A diagnosis of diffuse idiopathic skeletal hyperostosis (DISH) was made. DISH primarily affects elderly men and results in ossification of ligaments and tendons as well as parts of the upper aerodigestive tract. Characteristically, ossification of the anterior longitudinal ligament is seen, resulting in the formation of intervertebral osteophytes.2 Although asymptomatic in most cases, patients may have symptoms such as dysphagia and dysphonia, and very rarely airway obstruction.3
Acute airway obstruction is rare in this condition, but securing a safe airway follows the same protocol and assessment as for the other causes. Early assessment and clinical observation by an experienced airway clinician will guide intervention.
Learning points
There are a wide range of aetiologies of acute airway compromise; these tend to be infection, malignancy and foreign bodies.
More unusual causes for airway compromise must always be considered when the aetiology is not immediately obvious.
Urgent assessment by an airway-trained clinician should be sought as soon as possible all cases of airway obstruction.
Footnotes
Contributors AWH reviewed the literature and prepared the manuscript. KD provided critical review and images. SG revised and supervised the manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.