Article Text

Statistics from Altmetric.com
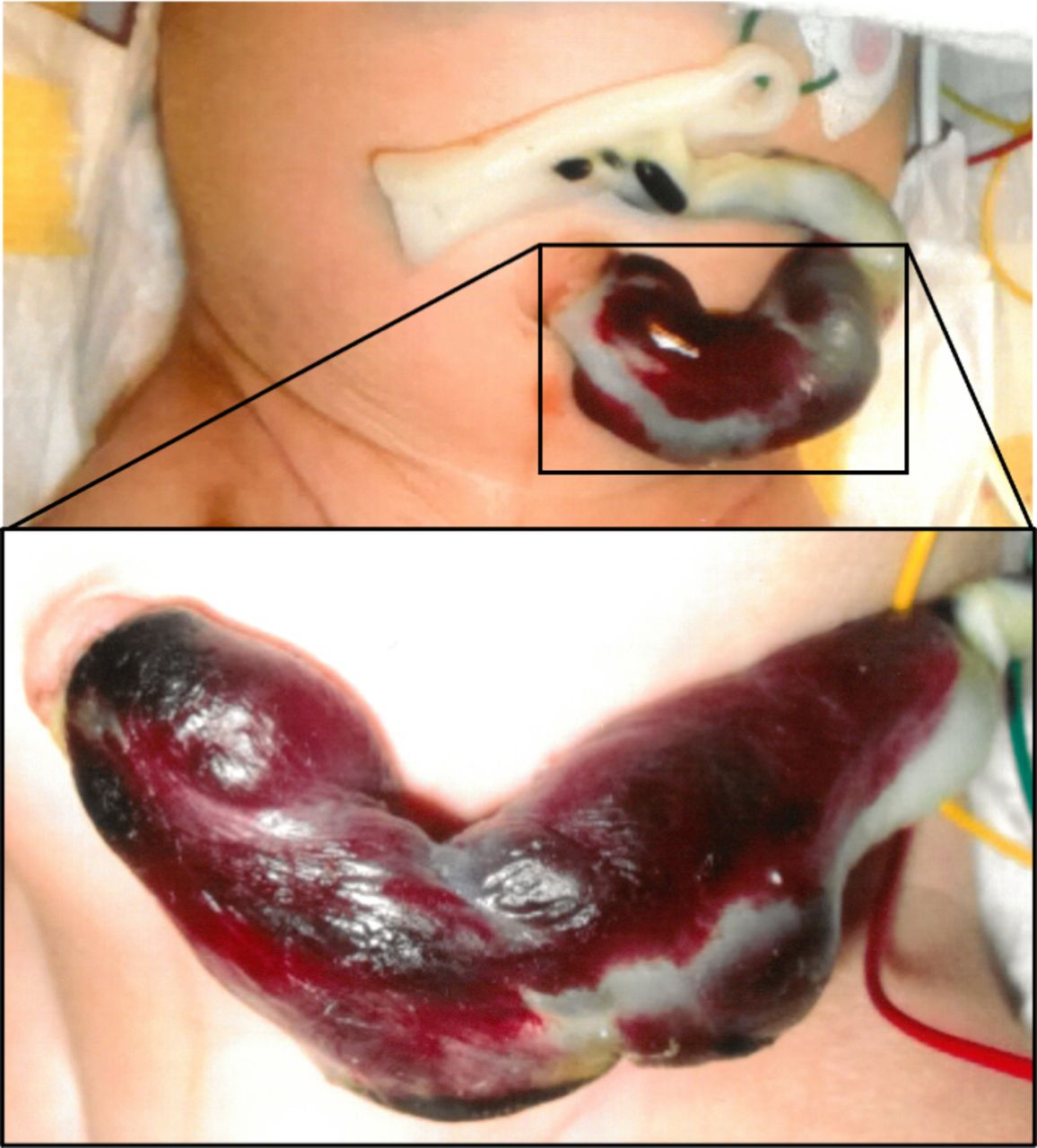
A baby boy was delivered at term by emergency caesarean section because of abnormal fetal heart rate patterns during spontaneous labour. The umbilical cord arterial blood obtained at delivery had a pH of 6.97 and a lactate concentration of 12.1 mmol/L. The Apgar scores were 3 and 7, respectively, at 1 and 5 min. The proximal umbilical cord had a thrombotic aspect at delivery (figure 1). A thrombus was also identified in the ductus venosus at 1 hour of life. The boy presented left hemicorporeal seizures at 21 hours of life, which revealed a neonatal arterial ischaemic stroke (NAIS; figure 2). Placental histology revealed acute chorioamnionitis (online supplemental file). Screening for thrombophilia was negative in the boy and his mother.1
Supplemental material

Umbilical cord at delivery.

{kind=link}
{kind=link}
Focal restriction of diffusion on cranial MRI at 24 hours of life, delineating a recent ischaemic lesion in the superficial posterior territory of the right median cerebral artery.
The pathophysiology of NAIS remains unclear but may be multifactorial.2 Two main mechanisms of NAIS are currently suspected: a cerebral embolism of a placental thrombosis and a focal cerebral arteritis secondary to chorioamnionitis.3 However, the intuitive embolic hypothesis is challenged,3 and perinatal inflammation is consistently reported as a major independent risk factor of NAIS in recent case–control studies.3 4
The baby combined a lot of NAIS risk factors: nulliparity, male sex, multiple markers of difficulty with transition—fetal heart rate abnormality, emergency caesarean section, low Apgar score, low umbilical artery pH—and perinatal inflammation.2–4 Proximal umbilical cord thrombosis is highly unusual and has never been described in NAIS.
Ethics statements
Patient consent for publication
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MD, TR-B and AG collected and analysed the data. MD and AG drafted the manuscript. SC and AG reviewed and revised the manuscript.
Funding Our work was supported by the Region Auvergne-Rhône-Alpes.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.