Article Text

Abstract
Chronic pain is an important clinical problem affecting significant numbers of children and their families. The severity and impact of chronic pain on everyday function is shaped by the complex interaction of biological, psychological and social factors that determine the experience of pain for each individual, rather than a straightforward reflection of the severity of disease or extent of tissue damage. In this article we present the research findings that strongly support a biopsychosocial concept of chronic pain, describe the current best evidence for management strategies and suggest a common general pathway for all types of chronic pain. The principles of management of some of the most important or frequently encountered chronic pain problems in paediatric practice; neuropathic pain, complex regional pain syndrome (CRPS), musculoskeletal pain, abdominal pain and headache are also described.
- Paediatric Practice
- Pain
Statistics from Altmetric.com
Introduction
Chronic pain is generally defined as any continuous or recurrent pain lasting more than 12 weeks, or pain that persists beyond the normal expected time for tissue healing; causes may be postinjury, disease-related or idiopathic. Prevalence rates for idiopathic pain range substantially in community surveys (eg, headache: 8–83%; abdominal pain: 4–53%; back pain: 14–24%; musculoskeletal pain: 4–40%), they are generally higher in girls and increase with age.1 Similar high rates are reported for disease related pain; for example, in children with polyarticular arthritis 76% reported pain on >60% of days despite treatment with methotrexate, tumour necrosis factor-α inhibitors or both.2 Identification and management of chronic pain of any aetiology is important because of its striking association with characteristic behaviours and negative effects on everyday functioning that are not only harmful and distressing in themselves, but may also delay or prevent recovery and contribute to poor long-term prognosis. These behaviours and effects are sometimes described as ‘chronic pain syndrome’ although the term does not clarify diagnosis.
The management of chronic pain in children is frequently challenging, not least because the complex relationships between chronic pain, illness and health are often poorly appreciated and understood by patients and clinicians. Below we describe the pathophysiology, presentation, principles of assessment and management of chronic pain and suggest a general pathway for care. Additional references and recommendations for further reading are provided as online supporting materials.
Pathophysiology of chronic pain: the biopsychosocial model
The mechanisms underlying the presentation of chronic pain in childhood can best be explained using a developmentally appropriate biopsychosocial model, similar to that previously described by Gatchel.3 The complex nature of pain is illustrated by the fact that the severity and time course of chronic pain are frequently not directly or clearly related to underlying pathology or recovery from illness. Obvious examples of this disconnection include the childhood ‘functional’ pain syndromes, where it is sometimes concluded that pain is not due to a physical cause. However, it is also known that daily pain and pain-associated impairment of functioning also correlate poorly with disease control in children with better understood chronic illnesses involving tissue injury by mechanisms such as inflammation and/or hypoxia, including Juvenile Idiopathic Arthritis (JIA) and Sickle Cell Disease. In fact, scientifically supported biopsychosocial concepts of pain physiology do explain these observations without the need to attempt to inaccurately (and often arbitrarily) dichotomise the causes of chronic pain into ‘physical’ or ‘psychological’.
Briefly, tissue injury leads to ‘nociceptive’ pain due to the activation of nociceptors and signal transmission by nociceptive pathways, it may be somatic or visceral. Nociceptors are sensitised, and therefore more easily activated, by inflammatory mediators and other substances generated by physical tissue damage or injurious chronic disease processes. This in turn can lead to central nervous system (CNS) sensitisation (central sensitisation) causing augmented, persistent and more widespread ‘inflammatory’ pain, although redness and local tissue swelling—the other components of the classic triad of inflammation—are not necessarily present.
When nervous tissue is damaged, pain is described as ‘neuropathic’; nociceptor and CNS sensitisation also occur but the mechanisms, clinical characteristics, time course and pharmacological management are different.4 Pain perception in nociceptive, inflammatory and neuropathic states is strongly influenced by descending modulatory circuits from cortical, limbic and other brain areas, and by developmental, genetic and environmental factors that can blur the relationship between any initiating stimulus and subsequent pain.5–7 Pain symptoms, pain-related disability and prognosis in disease-related and idiopathic chronic pain, also show demonstrable associations with psychological distress, emotional functioning, parental attitudes, family illness models, cultural values and previous negative life events. Associated CNS changes and mechanisms linking these factors are clearly emerging, for example brain imaging studies in a number of chronic pain conditions have found significant changes in structure and functional connectivity compared with controls. The role of CNS plasticity in long-term pain, the regulation of pain during development and neuropathic pain in children have all been reviewed recently.4 ,7 ,8
Sleep disturbance, anxiety and mood disorders are common comorbid problems in children with chronic pain. Compared to controls, children and adolescents with pain due to JIA, sickle cell disease, migraine/headache, functional abdominal pain, juvenile fibromyalgia syndrome, chronic musculoskeletal pain and mixed causes, all suffered from clinically damaging sleep impairment.9 Disordered sleep and pain sensitivity are closely inter-related, and studies show that treatment of sleep problems may improve pain symptoms, analgesic effectiveness, mood and quality of life. Clinically elevated levels of anxiety were reported in children with non-cardiac chest pain (56–81%), juvenile fibromyalgia (58%) and abdominal pain (45–79%).10 Chronic pain is also a risk factor for suicidal ideation in adolescents.11 Significant pain-related impairment of daily functioning, particularly school attendance, shows clear relationships with pain intensity, psychological and emotional functioning.12–15
Given the importance of pain as a mechanism for survival, it is perhaps unsurprising that pain perception is clearly influenced by conscious and unconscious memory, cognitive and emotional functioning and contextual factors that are explicitly included in a biopsychosocial formulation of pain. It follows therefore that as chronic pain is the result of a complex interaction of biological, psychological and socially determined mechanisms, it should be assessed and managed within the framework of these three domains. In addition, it is essential to appreciate that suppression or treatment of underlying disease may not lead to resolution of pain and therefore pain should be managed independently and concurrently.
Initial presentation, assessment and management pathway
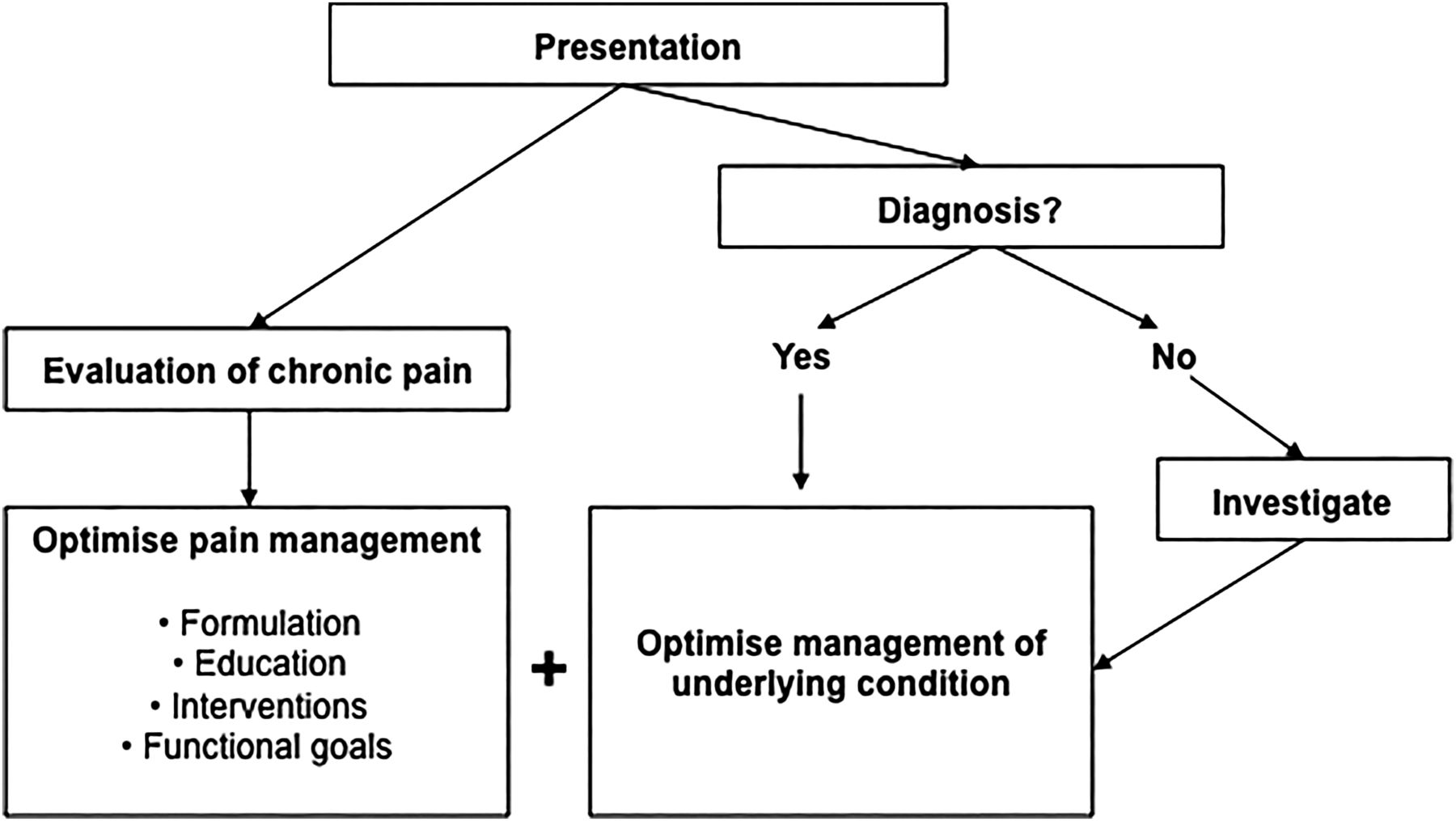
The initial approach to assessment and management is shown in figure 1. The aims are to identify and quantify important symptoms, signs and behaviours indicating possible mechanisms of pain, its impact on functioning, and to identify targets for treatment. Important areas of questioning within the three domains are given in table 1.
Domains of clinical evaluation of chronic pain at presentation

Clinical management of paediatric chronic pain on presentation.
The use of instruments such as age-appropriate diagnostic or health screening questionnaires and formal assessments of psychological and physical function are potentially helpful but may not be feasible in general clinics. Importantly, pain should be assessed and managed separately, contemporaneously and in conjunction with any investigations or diagnostic clarification.
Assessment and management are bridged by an individualised biopsychosocial formulation (see below) and a treatment plan that includes pain education, therapeutic interventions as indicated, and the setting of functional outcome goals. Figure 2 shows a common pathway for chronic pain management, regardless of aetiology. Outcome goals should be developmentally appropriate, personally meaningful and negotiated with children and their families, for example, a staged improvement in school attendance and resumption of previously enjoyed activities/social interactions. Reviews should be at predetermined intervals. If progress is unsatisfactory, further evaluation and modification of the management plan may be indicated to identify barriers and refocus interventions. Progress depends on many factors including the complexity and chronicity of the pain problem and associated degree of functional impairment, access to specialist input such as physiotherapy and psychology, and patient and family adherence to interventions. Lack of progress and failure of symptom resolution should lead to referral for specialist, multidisciplinary input (figure 2).

Paediatric chronic pain referral and management pathway.
Principles of management and interventions
Because the many co-contributing mechanisms to chronic pain are relevant across multiple patient diagnostic groups, common management strategies are often applicable such as a trial of simple analgesics, sleep management and interventions to improve pain coping and restore function, although direct evidence for specific treatments is stronger for certain pain conditions.
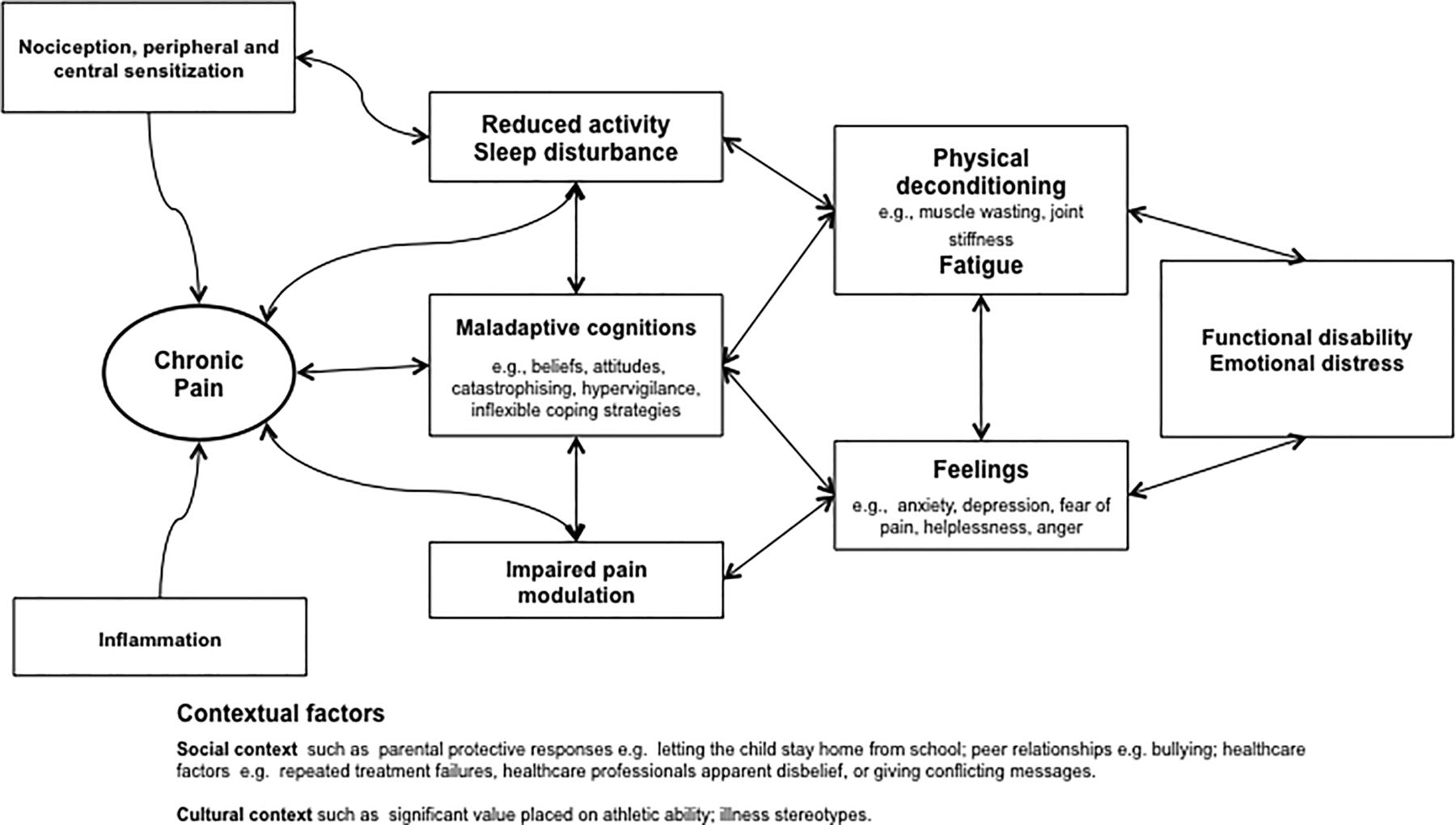
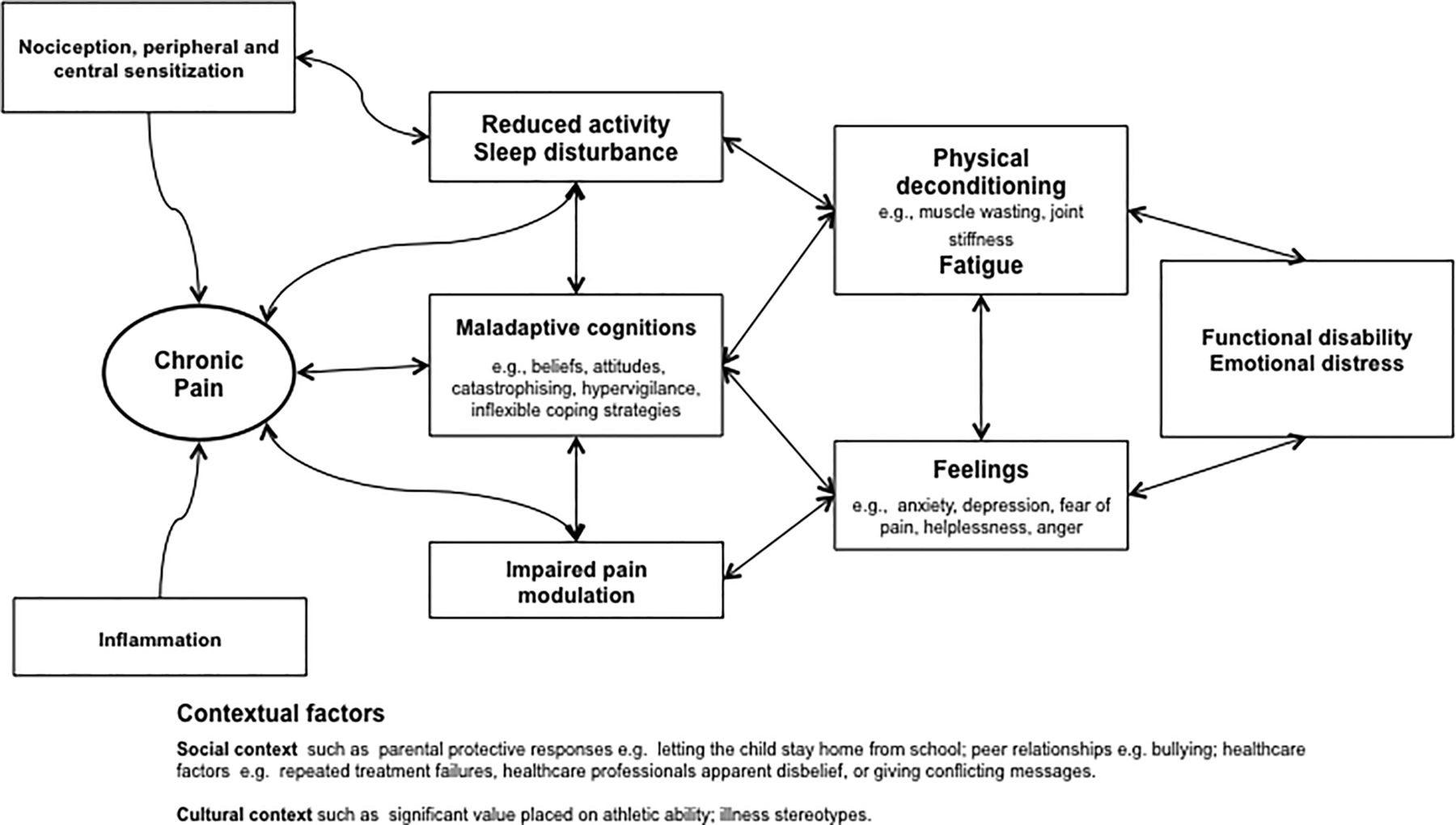
The first step is to construct an individual biopsychosocial formulation of pain that is shared with patient and family through pain education; figure 3 gives an example for a child with chronic inflammatory pain. The formulation explains contributing causes of pain and the rationale for management using pharmacological, physical and psychological interventions, it also helps to establish a constructive therapeutic relationship by acknowledgement, validation and explanation.
{kind=link}
{kind=link}
{kind=link}
Generic formulation diagram of chronic inflammatory pain. Formulation is the summation and integration of the knowledge acquired through assessment of the patient and family. It draws on current evidence and theory to provide a framework for describing the pain problem, associated impaired functioning and emotional distress. It explains how pain developed and is maintained. A formulation may comprise of a number of provisional hypotheses and targets of intervention.
Pain education: The goal of education is to find a common denominator between current scientific knowledge of the (biopsychosocial) nature of chronic pain and the subjective viewpoint of the child and their family, so that they are better able to cope with pain and engage with management strategies. This includes explanation and reassurance about the cause of pain, a brief summary of relevant pain mechanisms and the integral role of psychosocial and physical factors in precipitating and maintaining pain. The use of therapeutic stories, metaphors, leaflets, books, on-line information resources, ‘apps’ and other audiovisual media can be introduced in a supportive function to consolidate verbally transmitted information. A recent systematic review concluded that cognitive reassurance, that is, providing explanations and education, was associated with higher satisfaction, enablement, reduced concerns directly after the consultation, improvement in symptoms at follow-up and reduced health care utilisation in adults when compared with affective reassurance, that is, creating rapport and showing empathy.16 Tending to confirm intuitive support for the concept that, for parents at least, strategies that improve understanding are more likely to be effective.
More comprehensive pain education programmes are often a component of specialist pain management. Recent meta-analyses have demonstrated efficacy for educational and/or psychosocial (skill-based and educational) interventions on various outcomes, findings also indicated that higher ‘dose’ interventions (≥2 h in one setting or≥4 teaching sessions) were significantly more likely to work.17
Pharmacological interventions: Robust studies of pharmacological interventions in childhood chronic pain are lacking, but nevertheless the use of analgesics is widespread and based on (i) putative mechanism of pain (nociceptive, inflammatory or neuropathic) or presence of central sensitisation, (ii) evidence for efficacy extrapolated from acute pain or chronic pain in adults together with (iii) an individual risk-benefit analysis. Combinations of analgesics are frequently used in specialist settings, but new analgesics should always be introduced on a ‘trial’ basis and therefore withdrawn if not effective or side effects outweigh benefits.
Simple analgesics such as paracetamol and non-steroidal anti-inflammatory drugs may have a place singly or in combination with the long-term management of inflammatory pain, although their effects should be carefully monitored and doses frequently reviewed. Opioids and compound analgesics containing opioid are rarely indicated for chronic pain except in palliative care because of their side effects and problematic pharmacodynamic effects that can occur with long-term use such as drug tolerance, dependence and opioid-induced hyperalgesia.18 ,19 Chronic opioid use is also known to cause potentially damaging sleep disordered breathing and may lead to cognitive deficits in some patients.
Neuropathic pain may respond to treatment with drugs that act on neurotransmitters and ion channels that are involved in pain transmission in damaged nervous tissue. Amitriptyline, a tricyclic antidepressant, has a fairly well-established place in the treatment of neuropathic pain in adults where it is considered a first-line therapy in non-specialist settings. Low dose amitriptyline (5–10 mg daily) is also used in children with some types of neuropathic pain, where its sedative effect can also be helpful if there is accompanying disordered sleep.4 ,20 The use of amitriptyline for other pain conditions is controversial although it is used in adults with fibromyalgia, where it is thought to reduce pain due to effects on central sensitisation, although a recent Cochrane review concluded that a positive effect is likely only in a minority of patients.21 Studies have concluded that amitriptyline is either not effective or there is insufficient evidence to support its use in childhood migraine or functional abdominal pain.22 ,23
Gabapentin and pregabalin are calcium channel–blocking anticonvulsants with activity against neuropathic pain in adults and children.4 ,19 They have also been shown experimentally to reduce central sensitisation in adults and consequently have been used in fibromyalgia but there is currently no evidence to support such use in children. Gabapentin may be helpful in childhood refractory insomnia.24 Pregabalin has been shown to be effective in postchemotherapy neuropathic pain.25
Overall, the role of pharmacological interventions in children with chronic pain in non-specialist settings is severely limited by lack of research evidence for efficacy and potential side effects. In a number of cases, for example, when opioids administered during a previous acute pain episode have been continued, or in medication-overuse headache, gradual withdrawal (rather than the introduction of new medicines) is indicated as part of the overall treatment strategy.
Psychological interventions: A broad number of interventions underpinned by psychological theory and methods, emphasising psychological or social factors rather than biological factors, are included under the umbrella term psychological interventions. Primary interventions that are currently used include multicomponent cognitive behavioural therapy augmented by strategies such as relaxation, hypnosis, biofeedback and operant strategies aimed at parents. Other self-management interventions commonly delivered within a cognitive behavioural framework include pacing and sleep hygiene.
A recent systematic review found psychological treatments to be effective in reducing pain intensity for headache and also improved pain and disability in non-headache pain (including JIA and sickle cell disease). Evidence is limited to estimate the effects of psychological therapies on mood and also for effects on disability in children with headache.26 The inclusion of parents, significantly improves child symptoms for painful conditions immediately post-treatment.27 Studies directly comparing self-administered versus therapist-administered interventions have found similar effects on pain reduction.28
‘Pacing’ is regularly recommended and involves individuals learning to balance time spent on activity and rest in order to achieve increased function/participation in meaningful activities.29 However, the concept currently lacks consensus definition and demonstrable evidence base as a stand-alone intervention.
Sleep management primarily involves identifying poor sleep hygiene patterns and implementing strategies to improve sleep regulation.
Physical interventions include but are not limited to physiotherapy, massage therapy and desensitisation treatments, transcutaneous electrical nerve stimulation (TENS), local heat and cold (thermal analgesia), acupuncture and mirror box therapy. The rationale for physiotherapy in chronic pain stems from evidence of the beneficial effects of exercise on tissue healing, function and mood coupled with the belief that activity avoidance and resultant deconditioning contribute to ongoing pain by encouraging a negative cycle of decreasing function and increasing pain.30 Research studies tend to report physical interventions as part of multimodal pain management, including psychological and pharmacological techniques rather than trials of clearly defined physiotherapeutic techniques such as progressive muscle strengthening, graded motor imagery, sensory-motor treatment or in vivo graded exposure alone.31 Physiotherapy has an established place as a component of multidisciplinary management of childhood chronic pain, especially in the management of musculoskeletal pain and complex regional pain syndrome (CRPS).31 ,32 Acupuncture and other forms of complementary medicine are used in some centres, and even though children and families often report that such treatments are helpful, evidence is otherwise lacking. Mirror box therapy is a relatively novel sensorimotor technique for localised pain in a single limb in which patients perform movements of the unaffected limb while watching its mirror reflection superimposed over the (unseen) affected limb, thus creating a visual illusion of affected limb movement.33 ,34 A number of small studies and case reports have found benefit in adults and adolescents with (neuropathic) phantom limb pain.35 ,36 However, mirror therapy has been shown to have positive and negative effects on the symptoms of CRPS.37
Specific chronic pain conditions
Neuropathic pain is defined as pain that is due to a lesion or disease of the somatosensory nervous system, its causes, assessment and management in childhood have been reviewed recently.4 Neuropathic pain may coexist with nociceptive/inflammatory pain; causes include traumatic injury, cancer, chemotherapy, chronic infection, neurological and metabolic disease, and inherited sensory nerve dysfunction.4 CRPS II is by definition due to nerve injury, whereas CRPS type I presents a similar clinical picture but without obvious nerve damage. The evidence base for the use of medications and interventions for neuropathic pain in children is weak.4 ,38 Specific pharmacological management potentially includes many systemic and local treatments but as the efficacy and therapeutic index are often relatively low, fairly rapid progression to specialist assistance is recommended if neuropathic pain is suspected or responds poorly to first-line treatment.4
Complex regional pain syndrome was formerly known as reflex sympathetic dystrophy or causalgia. It is characterised by localised pain with variable swelling, discolouration (vasomotor), abnormal sweating (sudomotor) and dysmorphic changes to hair and nails, usually distally in a single, usually lower, limb. It is rare below the age of 5 years and most frequently seen in girls, peak incidence 14 years.39 Most commonly there is no obvious precipitating factor. The diagnosis is often delayed having tried a variety of unhelpful interventions, including immobilisation, consequently children with CRPS can present with significant functional impairment.40 Clinical criteria for diagnosis, validated in adults, may be helpful in reducing diagnostic confusion.41 Severe CRPS can be accompanied by dystonia with strikingly abnormal posture or limb position and sometimes associated movement disorders. The prognosis of childhood CRPS is good, although relapses are common (25–40%); delay in diagnosis and inappropriate treatment may adversely affect prognosis.42
Following assessment, interventions favouring mobilisation or remobilisation of the affected limb are universally held to be important. Early referral to an appropriately experienced physiotherapist and other physical interventions such as desensitisation and TENS are indicated along with pharmacological and psychological interventions such as simple analgesics and distraction to improve the tolerability of painful exercises. Amitriptyline, gabapentin and other agents active in neuropathic pain are sometimes also used empirically for CRPS. Failure to progress or worsening of symptoms and disability are likely to be multifactorial and should trigger specialist referral for multidisciplinary assessment and management.39 Although physiotherapy is often held to be key, there have been few good studies analysing the contribution of different elements of care and most specialist treatment programmes for CRPS offer a package of physical, psychological and pharmacological strategies.31
Chronic Musculoskeletal Pain that is either generalised or localised (eg, low back pain or joint pain) can lead to significant functional impairment, it may be disease-related, persisting after treatment of joint inflammation or trauma, or there may be no clear cause.42 ,43 Adolescents with chronic widespread musculoskeletal pain, sometimes called juvenile fibromyalgia or diffuse idiopathic pain are increasingly presenting for treatment, characteristically, they have pain at multiple sites, poor physical functioning, disturbed sleep, fatigue and low mood. Again, initial assessment (figure 1) should focus on clarification of the diagnosis and confirmation that any underlying treatable inflammatory or other cause of pain is optimally managed. Partly correctable biomechanical factors may contribute such as poor posture, flat feet, leg length discrepancy, deconditioning (reduced muscle strength and endurance) and obesity, in addition joint hypermobility (the presence of increased mobility in 6 or more joints) has been associated with musculoskeletal pain in some populations.44–46 Recent reviews have emphasised biopsychosocial formulations of pain and the importance of pain education for children and their families as a part of management.42 ,43
Simple analgesics (paracetamol and NSAIDs) have usually been tried by families and found to be ineffective. Opioids can contribute to lethargy and fatigue and are not indicated. A trial of amitriptyline or gabapentin may be logical if central sensitisation is thought to be playing a role, although there are no studies to support this strategy. A rehabilitative approach using sleep management, functional targets, graded or paced aerobic exercise therapy with targeted muscle strengthening are most often used together with psychological strategies for the management of pain, anxiety or low mood (figure 2).
Headaches are common during childhood, population prevalence estimates range from 8–83%.1 Primary headache disorders are predominantly migraine and tension-type headache. Secondary headache due to central nervous mass lesions, infection or other pathology should be excluded (figure 1). A minority of children with primary headache report daily headaches and significant disability. Migraine headaches differ from those in adults (no aura) and migraine variants are more common, for example, opthalmoplegic or complex migraine with transient neurological abnormalities.
Primary headache is usually amenable to patient and family education, removal of possible triggers and judicious use of simple analgesics. Specific therapies and prophylaxis for migraine such as triptans and β-blockers are also used but have not been subjected to rigorous evaluation in children.47 Further interventions such as sleep management, increased physical activity, school attendance and changed dietary habits, including adequate hydration, are often recommended.47 ,48 Psychological therapies are effective for primary headache. Recent meta-analyses support relaxation training for recurrent headache; a large positive effect on pain reduction at immediate post-treatment and follow-up was found, whereas there were small and non-significant effects on disability and emotional functioning.26 ,49 Long-term improvements over more than 3 years after treatment with relaxation, for tension-type as well as migraine headaches, have also been shown. Recently, applied relaxation has been presented via the Internet to children and adolescents with recurrent headache with positive effects.50
Chronic or recurrent abdominal pain (CAP) is defined as at least 3 pain episodes over at least 3 months interfering with function. The incidence of CAP peaks between ages 4 to 6 years and again in early adolescence (particularly girls >12 years). Significant ongoing pain is usually medically investigated in order to identify directly treatable causes such as inflammatory bowel disease, but the cause often remains obscure (figure 1). Clinical guidelines on the investigation and management of CAP including ‘red flag’ symptoms of organic disease and ongoing management are available.51 Functional gastrointestinal disease (FGID) is classified according to Rome III criteria. A recent study identified prognostic subgroups of FGID associated with CAP based on pain severity and psychosocial variables at first assessment: children with high levels of pain, poor pain coping, negative affect, pain catastrophising and higher levels of functional disability with evidence of central sensitisation had the worst long-term prognosis.52
As before, the principles underpinning the treatment of CAP emphasise a biopsychosocial formulation of pain together with pain education and targeted interventions. Symptoms are sometimes associated with specific foods, and eating is frequently cited as a pain trigger in FGID. Peppermint oil supplements for 2 weeks reduced symptoms in children with irritable bowel syndrome in one RCT.53 Amitriptyline was equivalent to placebo in one study, and a systematic review has concluded that there is little evidence to support the use of analgesics or other drug treatments.54 ,55 There is inconclusive evidence that a lactose-free diet decreases symptoms or that a fibre supplement decreases the frequency of pain attacks.56 Well-designed clinical trials and accumulated clinical experience support the view that hypnosis, as an integral part of biopsychosocial management, is the most efficacious treatment for CAP improving pain and disability outcomes.57 Long-term follow-up has shown that the beneficial effects remain even up to 5 years after the intervention in the majority of patients.58
Conclusion
Chronic pain in children and young people remains an entity which is often poorly recognised, evaluated and managed leading to unnecessary distress and poor health outcomes. In addition to the significant cost to a child's quality of life, the economic burden of chronic pain in young people in the UK was estimated in 2005 to be approximately £8000 per child per year.59 Progress in the development and investigation of novel treatments for childhood chronic pain remains slow in comparison with other chronic health problems.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors All three authors contributed to the conception and design of the article, performed literature searches and were involved in drafting and redrafting the article, revising it critically for important intellectual content, and approving the final version.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.