





Abstract
The authors present a case of coronary sinus spasm during left ventricular lead implantation for biventricular pacing relieved by direct infusion of nitroglycerin.
Case report
A 60-year-old man with idiopathic dilated cardiomyopathy, ejection fraction (EF) < 30%, left bundle-branch block with QRS duration of 160 ms, NYHA class III, and optimal medical therapy for at least 6 months was referred to our division for cardiac resynchronization therapy (CRT) using a biventricular pacing device. Triple puncture of the subclavian vein was used to introduce separate guidewires and 9-french peel away sheaths for positioning three pacing leads according to modified Seldinger technique.1 Right ventricular lead was first implanted and placed via fluoroscopy in apical position. Atrial lead was positioned in the right atrium appendage and secured by active fixture. After cannulation of the coronary sinus (CS) ostium, using a quadripolar electrophysiological catheter (Josephson curve, Bard Corp., Billerica, MA, USA) and a pre-shaped guiding sheath (RAPIDO Cut-Away Coronary Sinus Hook, Guidant Corporation, St Paul, MN, USA), the CS venogram was performed in order to define the anatomy of the CS branches and to select the optimal target vein.
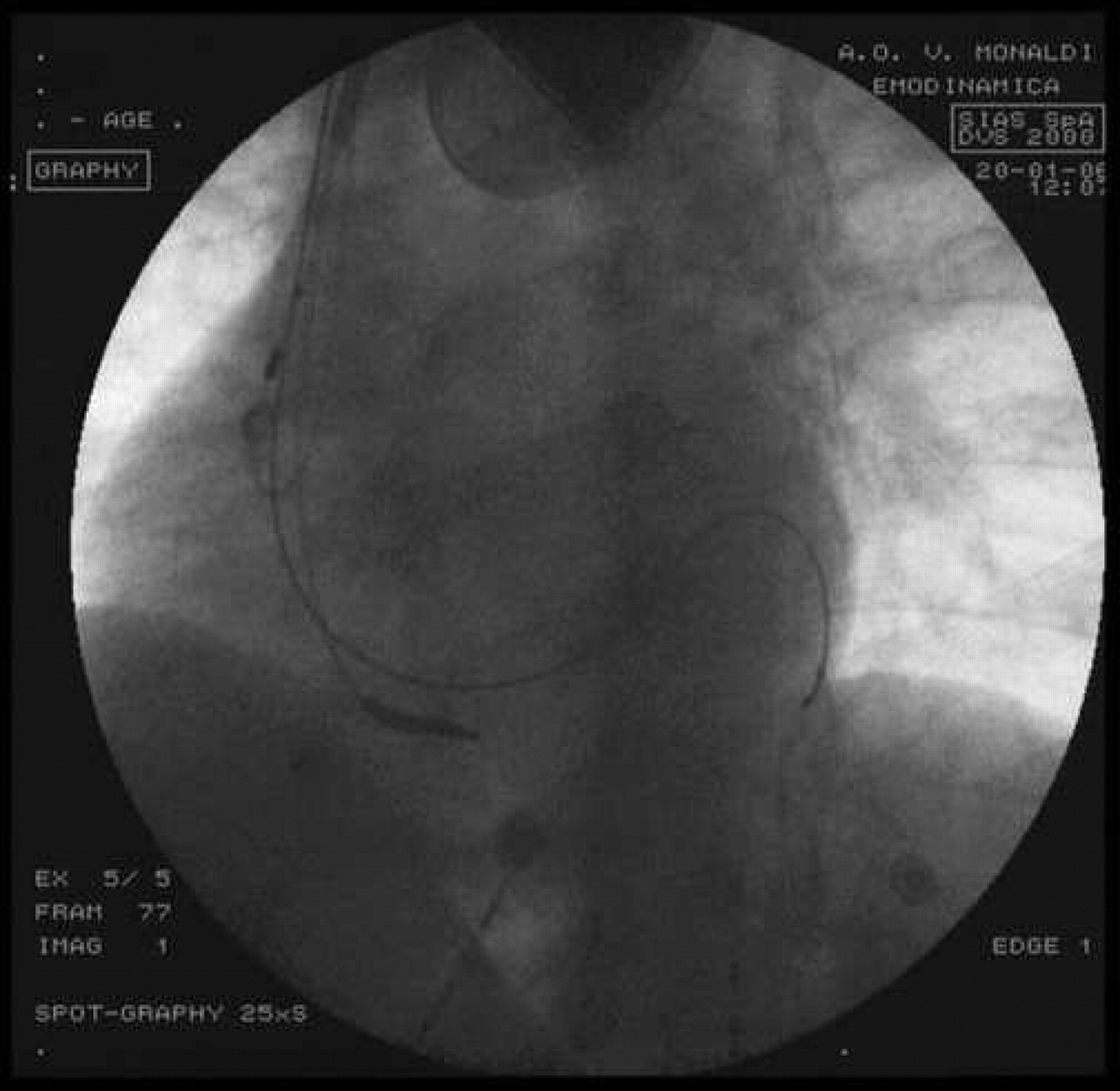
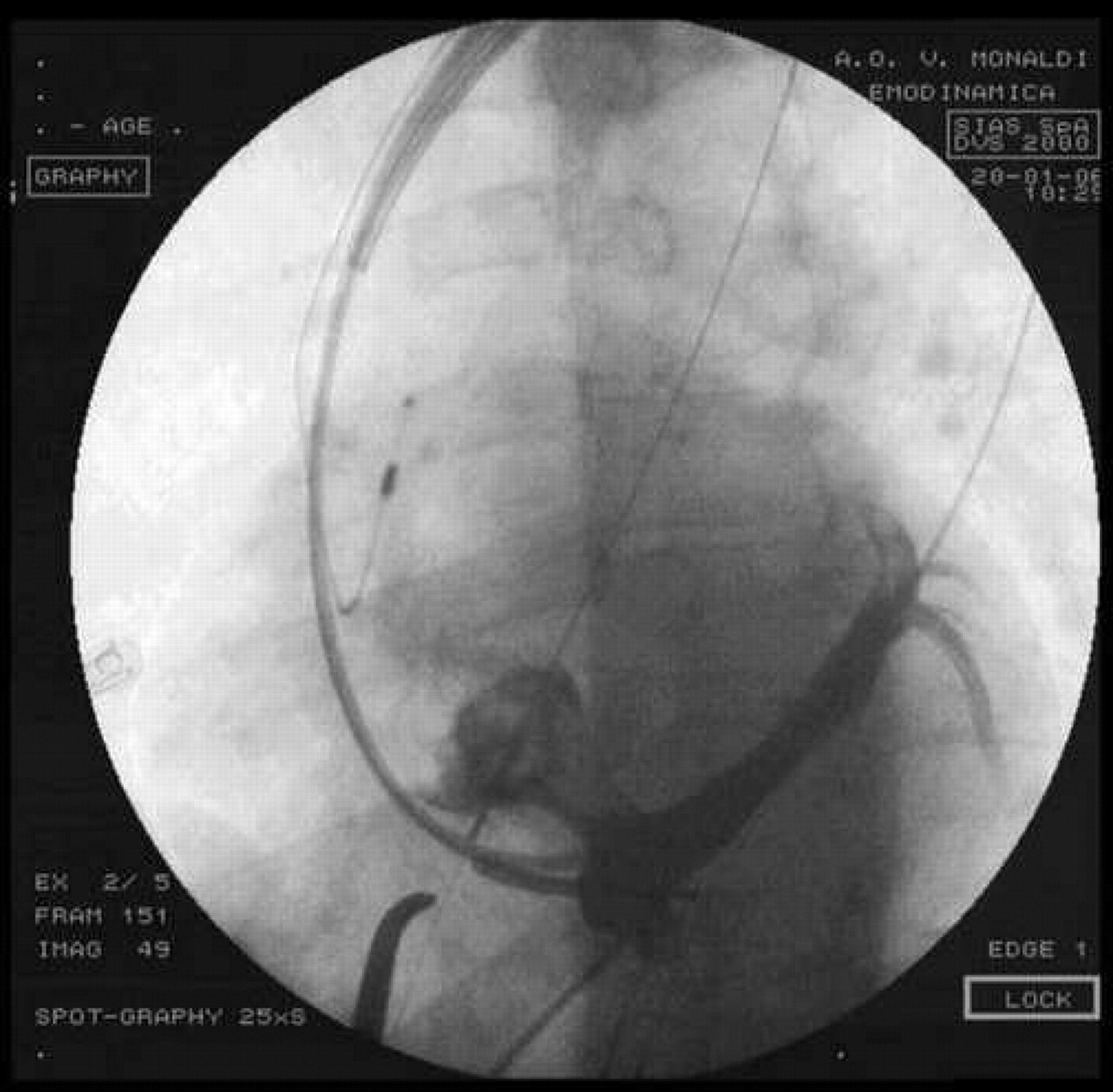
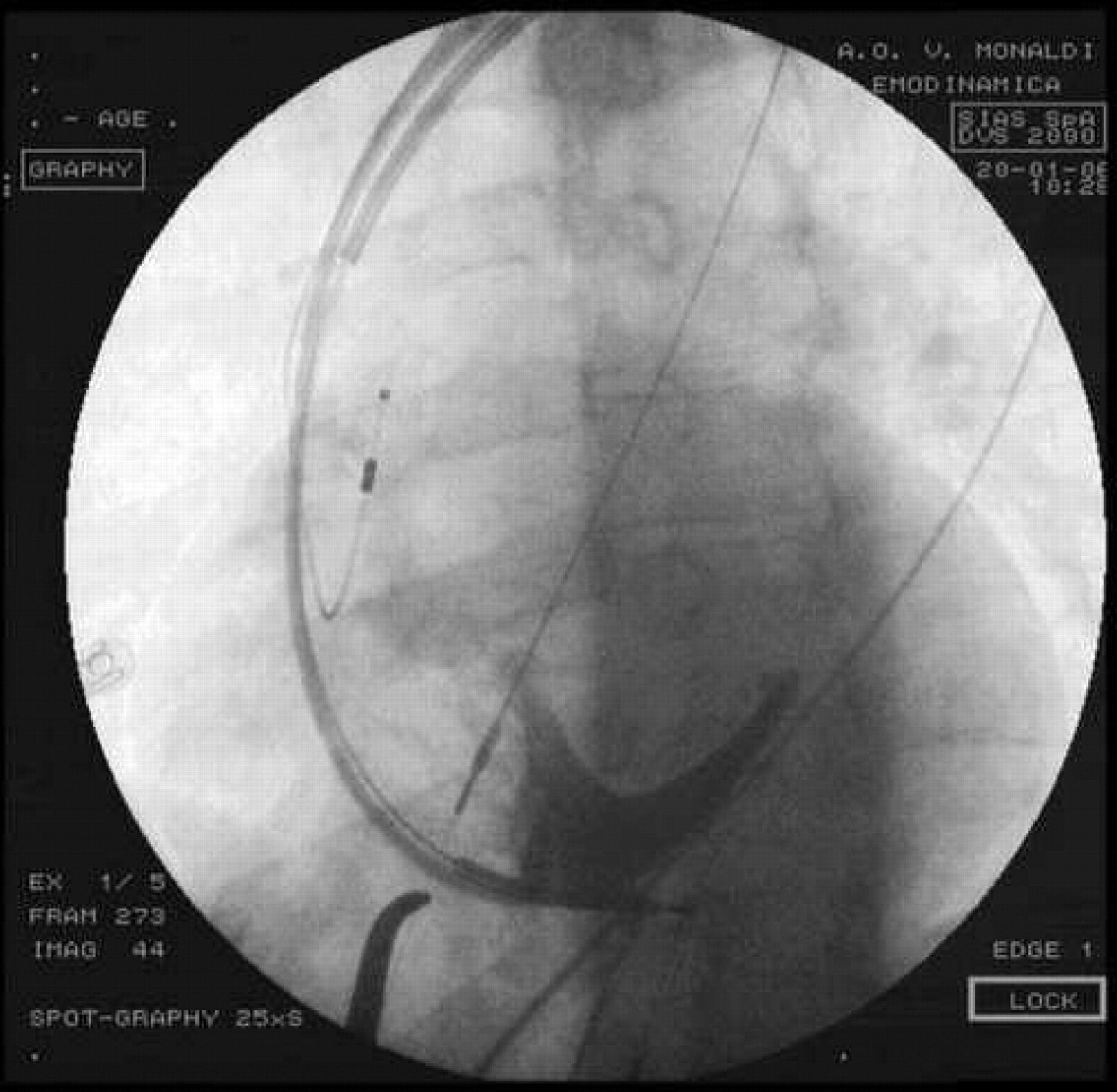
Coronary sinus contrast venography showed a complete occlusion of CS with no evidence of tributary veins, probably related to vasospasm (Figure 1). Direct infusion of nitroglycerin relieved the spasm (Figure 2) and allowed to visualize a posterior CS tributary vein, in which left ventricular (LV) epicardial lead was placed using Easytrack lead system (Guidant Corporation). Results of the implantation were assessed from the position of the leads on chest X-ray films (Figure 3) and from the changes in the QRS interval width on 12-lead surface electrocardiogram. CRT device was programmed in atrial synchronous biventricular pacing with the lower rate limit set at 40 bpm, and the upper rate limit set at 130 bpm. At 12 months' follow-up, thresholds remained intact and the patient showed an improvement in his functional capacity.
Left anterior oblique projection. Contrast venography showing complete occlusion of coronary sinus (CS) related to vasospasm, with no evidence of CS tributary veins. Right atrial and right ventricular leads position are shown.
Left anterior oblique projection. Direct infusion of nitroglycerin into coronary sinus relieved the spasm and allowed to visualize the detailed anatomy of the coronary sinus and its tributary veins.
Anterior–posterior projection. CRT system in place. The pacing leads in the right atrium and in the apex of the right ventricle are shown. Left ventricular pacing lead is placed in a posterior branch of the coronary sinus.
Conclusion
In appropriately selected patients, the leads positioning is of key importance to obtain a successful cardiac resynchronization therapy. Intravenous LV lead placement may be difficult with the presence of anatomical anomalies of the CS, cardiac veins, and ostial valves.2 Contrast venography is necessary in order to diagnose a pre-existing CS vein occlusion or other venous anomalies that might prevent successful transvenous LV lead placement. CS spasm may represent an under-recognized and reversible reason for inability to place biventricular pacing devices. If the direct infusion of nitroglycerin in CS does not relieve the spasm, it may be used as a standard venography balloon for dilating the CS region of spasm.3

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}