
Abstract
This paper considers the problem of inducing low-risk individuals of all ages to buy private health insurance in Australia. Our proposed subsidy scheme improves upon the age-based penalty scheme under the current “Australian Lifetime Cover” (LTC) scheme. We generate an alternative subsidy profile that obviates adverse selection in private health insurance markets with mandated, age-based, community rating. Our proposal is novel in that we generate subsidies that are both risk- and age-specific, based upon actual risk probabilities. The approach we take may prove useful in other jurisdictions where the extant law mandates community rating in private health insurance markets. Furthermore, our approach is useful in jurisdictions that seek to maintain private insurance to complement existing universal public systems.
Similar content being viewed by others


Introduction
In Australia, community rating by private health insurers is mandatory. By extension, adverse selection, where persons who are less healthy are more likely to be privately insured, is a persistent problem in the Australian private health insurance market. Under adverse selection, many healthy persons, who would benefit from private insurance, choose to remain uninsured in private markets because private insurance premiums are too expensive for their risk profile. To address this problem, the Australian Government recently introduced an age-based penalty scheme called “Lifetime Cover” (LTC). The stated goals of the LTC scheme are to (i) discourage “hit and run” behaviour by insured consumers (e.g., buying a policy prior to pregnancy and dropping it after the birth of a healthy child) and (ii) stabilize private health insurance coverage.Footnote 1 Basically, the intention of the LTC scheme is to encourage the low-risk young to take out and maintain private health insurance, thereby improving the risk composition of the insurance pool and lowering the attendant community-rated premiums. Arguably, the LTC initiative was the cheapest and the most effective of the recent policies that the Australian Government has pursued.Footnote 2 Elsewhere, ButlerFootnote 3 and Brown III and ConnellyFootnote 4 have shown that private coverage increased with the introduction of the LTC scheme.
The Australian scheme is novel in that it involves subsidies, which, unlike the subsidies due to the theoretical work of Crocker and SnowFootnote 5 and, in the private health insurance context,Footnote 6 are age-based. The extant literature suggests that subsidies are a second-best solution, which corrects the information asymmetry problems that prevent a Pareto optimal distribution in the health insurance market.Footnote 7 The subsidies under LTC are simply intended to provide incentives for young adults, being healthier on average relative to older adults, to buy and maintain private health insurance, with no claim of providing second-best optimality. As it is currently configured, though, this system will not produce and sustain the apparently intended outcome of higher and more stable levels of private coverage, partly due to the fact that the Australian age-based penalties do not distinguish between low-risk and high-risk persons of the same age.Footnote 8 The innovation of this paper is to produce an age-based subsidy profile that arrests and halts adverse selection in private health insurance markets with mandated community rating in the presence of a universal and mandatory public insurance system. Our contribution is to use the Rothschild–Stiglitz (RS) framework to demonstrate how the efficiency of the Australian scheme could be improved even if the second-best solutions due to Crocker and Snow,Footnote 9 or variations on them,Footnote 10 are not considered viable due to other (e.g., political) constraints.
To derive the subsidy profile, we use an age-varying, two-risk-types model in which the minority of private health insurance purchasers are initially assumed to be low-risks and the majority of private health insurance purchasers are assumed to be high-risks. Thereafter, low-risks face the prospect of becoming high-risk or remaining low-risk in each subsequent period, or year of life. To model the chance of becoming a high-risk type, we use the age-based incidence of 12 chronic conditions derived from the U.S. Medical Expenditure Panel Survey and the U.S. National Center for Health Statistics.Footnote 11 Essentially, we assume that the age-based incidence of chronic conditions corresponds with the incidence of “high-risk” status by age. Our lifetime risk model is based on the guaranteed renewability literature.Footnote 12 We combine these data with private health insurance coverage data from Australia in order to generate a community-rated base premium. We then generate a subsidy profile that is just sufficient to encourage risk-averse low-risks in every age group to take out private health insurance, thus obviating adverse selection in the presence of the community-rated LTC scheme.
Our illustration of improvements to an age-based insurance scheme takes the Australian LTC construct as given. In their oft-cited paper, Crocker and SnowFootnote 13 demonstrated that a system of taxes and subsidies can be used to address the equilibrium existence problem established by Rothschild and Stiglitz (RS).Footnote 14 In practice, though, taxes and subsidies are often invoked in settings that involve a public–private mix and in which most of the welfare-improving properties of risk reduction and equity have already been addressed by a public system with universal access rights. In this context, the principal concerns of policy-makers may be joint and several, but could include goals to ensure the availability of alternative insurance arrangements, to relieve pressure on the public system, to encourage innovation and diffusion of innovations in medical care, to improve the quality of care, to lower time costs and so on. Thus, as in the case of vouchers in the U.S. education system – where a universal public system already exists – the purpose of government intervention is primarily to ensure the existence of viable alternatives and choices in the education market.
The illustration of an age-based, risk-based subsidy scheme is also topical. The recent health economics literatureFootnote 15 has challenged the conventional wisdom of increasing health expenditures as a function of the age distribution of the population.Footnote 16 Similarly, epidemiologists have expounded several alternative theories about the relationship between the burden of illness and disease longevity. The latter are well-discussed by Michel and Robine.Footnote 17 Thus, it seems that insurance penalties for not maintaining insurance that are based purely on age, like LTC, and not modified by risk, may exacerbate adverse selection by dissuading purchases by the low-risk old. Our work presents a tractable alternative that is likely to improve the risk composition of the pool by attracting older low-risks to the pool. A key advantage of our model is that it separates risks for the healthy from the unhealthy, by age.
In order to generate an improved lifetime subsidy stream that stabilizes insurance coverage, we invoke the RS framework. We have previously used the RS framework to demonstrate the shortfalls of the age-based penalties that apply under the Australian “Lifetime Cover” (LTC) scheme.Footnote 18 In this paper, we present a solution to the current problems of the LTC scheme, taking its basic structure as given. The resulting scheme stabilizes membership by age and risk type and remedies the adverse selection problem.
The structure of the paper is as follows. In the next section, we outline the main features of Australian private health insurance markets and provide an institutional context for our theoretical and empirical work. In the subsequent section, we describe the main features of our model and methods, and describe our lifetime risk profile based on the guaranteed renewability literature.Footnote 19 In that section, we also formulate the basis for a subsidy profile that obviates adverse selection under the LTC scheme. The penultimate section presents the results, and the final section concludes with a discussion of our results and their implications for possible reforms to Australia's private health insurance markets.
The Australian private health insurance market
The Australian Medicare scheme is a tax-financed scheme that provides (i) zero-price care to individuals who are treated as public patients in public hospitals (as discussed below, one can be a private patient in a public hospital), (ii) subsidies for services provided by private, fee-for-service (FFS) medical practitioners, both in- and out-of-hospital, and (iii) subsidies for a wide range of pharmaceuticals, pathology, diagnostic imaging and other health care (e.g., optometry) services.
The introduction of the Medicare scheme substantially increased public sector direct expenditures on health care in Australia. Prior to the introduction of Medicare (or its predecessor program Medibank), the public sector's role in health care financing was mostly indirect and in the form of income tax concessions for private health insurance and health expenditures.Footnote 20 Indeed, in the decades prior to the introduction of Medicare, most Australians held private insurance.
At the zenith of private health insurance coverage in 1970, 80 per cent of the Australian population held private health insurance.Footnote 21 After the introduction of the Medicare scheme, however, private health insurance coverage fell; by 1984, 50 per cent of the population had private health insuranceFootnote 22 and, by December 1998, coverage had fallen to a nadir of 30.1 per cent.Footnote 23
Health insurance coverage was subject to a gradual and prolonged decline, for reasons that are readily apparent when the confluence of institutional arrangements in the Medicare era is considered. Australia's private health insurers have long been required to community-rate their policies. This mandate, which was desired to achieve the usual (equity, renewability, etc.) ends may perhaps be regarded as an institutional hangover from the pre-Medicare period, during which self-insurance was the only substitute for private insurance. Predictably, given ubiquitous public coverage with the introduction of Medicare, the retention of the community-rating provision accelerated an adverse selection process.
The empirical evidence of the adverse selection problem is clear. Between 1986 and 1998, private health insurance coverage fell from 44.2Footnote 24 to 30.1 per cent of the population;Footnote 25 during the same period, coverage of the 70+ years old population increased from 31.5 to 36.4 per cent, while coverage of the 25–34 years old population fell from 46.5 to 22.1 per cent.Footnote 26 Even if time-to-death, as opposed to age per se, were the primary driver of health expenditures,Footnote 27 these data speak unambiguously of an adverse selection problem. The historical depth of the adverse selection problem is also apparent from Butler'sFootnote 28 analysis of the expected benefit of health insurance for various age groups. In an analysis by state, he estimated that the ratio of the highest to the lowest benefits per capita for individuals of age 20 years and more was at least 6.8:1 for females and 14.6:1 for males by the late 1990s. These data also confirm the depth of the adverse selection problem, by illustrating, starkly, its source.
Several other aspects of Australian private health insurance markets are salient for the purposes of our subsequent analysis. First, in Australia, insurance is not generally employment-based as it is in the United States. Relatively few employers provide private health insurance as part of a remuneration package. Although health insurers often have corporate plan offers for various (usually large) employers, employees typically take up such offers as individuals and incur payroll deductions to pay for the cover. Second, treatment as a private patient in a public hospital typically provides one or more of the following kinds of incremental benefits: (i) lower time costs, especially for “elective” surgery; (ii) treatment by medical practitioners of the patient's choosing; (iii) private accommodation (or, in shared accommodation, smaller numbers sharing); and (iv) accommodation-related amenities (e.g., greater choice at meal times). Third, privately insured individuals can choose to forego the privileges of private patient status and receive treatment as a public patient, in a public hospital, at the zero-price. Fourth, there is no opt-out provision in the public Medicare scheme (i.e., purchasing private health insurance does not exempt one from payment of the Medicare Levy). Fifth, the costs associated with exercising one's private health insurance status for hospital treatment are not always trivial, even if the deductible on the policy is low. This has been a recurrent source of discontent among the privately insured. Sixth, private health insurance policies in Australia offer service benefits (with various co-payment provisions) to claimants, as opposed to lump sum transfers for insured events of illness.
The policy initiatives that have been employed to arrest adverse selection in Australia's community-rated insurance markets have been documented and discussed extensively elsewhere.Footnote 29 Briefly, though, the policies that preceded the introduction of the LTC scheme were tax-and-subsidy measures that were also designed to increase and stabilize private health insurance coverage. These initiatives by the government followed an inquiry by the (then) Industry Commission into private health insurance in Australia.Footnote 30 In response to the Industry Commission's findings, the government introduced the Private Health Insurance Incentives Scheme (PHIIS). The first initiatives took effect on 1 July, 1997 and involved subsidies for ancillary and/or hospital coverage for low-income individuals and families; and taxes upon high-income individuals and families who did not take out private health insurance. Middle-income individuals were neither taxed nor subsidized under these arrangements. The maximum subsidy paid under this scheme was $450 per annum for a family with both hospital and ancillary private insurance cover. The tax penalties for high-income earners in the high income band were 1 per cent of taxable income. Although the counter-factual situation cannot be known, this iteration of the PHIIS had little or no apparent effect on the secular decline in private health insurance coverage. Thus, on 31 December 1998, the government amended the subsidy arrangements and extended the 30 per cent subsidy to all individuals who took out private health insurance, irrespective of income. Unlike the previous iteration of the PHIIS, this time private health insurance coverage increased, albeit modestly, from 30.1 per cent of the population in the December quarter of 1998 to 32.2 per cent of the population in the March quarter of 2000. However, as ButlerFootnote 31 notes, the government's intention to introduce the LTC scheme was also announced late in this period (29 September 1999) and this may have contributed to the small observed increase in coverage at the time.
Finally, the LTC scheme itself involves age-based penalties for late joiners, with the penalties commencing at age 31. Under the LTC scheme, the ad valorem penalties are calculated by subtracting 30 from the joining age and multiplying by 2. That is, the penalty is 2 per cent of the base community-rated premium for every year, after 30 years of age, that private health insurance membership is delayed. Thus, a 40-year-old joining for the first time pays a 20 per cent premium loading for the duration of his/her membership. Also note that the maximum loading under the scheme is 70 per cent and that individuals aged 65 years or older as at 1 July 2000 were exempt from the LTC provisions.
In his work, Butler shows that there was both an announcement effect and an implementation effect associated with the LTC scheme, the latter being the largest in magnitude. Over the period from the announcement to the implementation of the LTC scheme on 15 July 2000, coverage increased from 31.0 per cent to 43.0 per cent of the population (i.e., a 39 per cent increase in coverage).Footnote 32 However, while the LTC scheme unambiguously increased membership and improved the composition of the pool, it did not solve the adverse selection problem. Elsewhere, we have shown that there is already evidence – based on the age-composition of the insurance pool – of the re-commencement of an adverse selection death spiral in the post-LTC period.Footnote 33
We now direct our attention to remedying the adverse selection problem that still exists under the LTC scheme. Our rationale is that marginal rather than radical changes to the existing scheme are likely to be considered by the Australian Government. To this end, our proposal for an age- and risk-based subsidy profile offers a tractable solution to the current problems in the extant, community-rated, LTC scheme and avoids making the perfect the enemy of the good.
The model and methods
While the length of the policy we propose is a lifetime, the RS frameworkFootnote 34 is a static model. Therefore, we apply the lifetime chronic illness risk profile from the guaranteed renewability literature, due to Pauly et al.,Footnote 35 to the RS framework at each age. The following subsection describes the lifetime chronic illness risk profile in the guaranteed renewability literature, and the subsection under this uses the lifetime chronic illness risk profile to estimate the community-rated premium. The second subsection applies the lifetime chronic illness risk profile to our RS characterization by age.
A lifetime risk profile
In the tradition of the guaranteed renewability literature due to Pauly et al.,Footnote 36 our risk profile construction is based on an assumption that two types of consumers – low-risks and high-risks – exist. Our profiles recognize the existence of both risk types at each age. We assume that, unlike acute illness, chronic illnesses increase future risks of illness permanently. Therefore, for low-risk types, the probability of the onset of a chronic illness is also the probability of permanently becoming a high-risk type. In other words, once a person becomes high-risk (suffers a chronic illness), he or she remains so for all subsequent periods.
In our model, low-risks face the probability of (chronic) illness of p Lt , conditional on not being ill, where the subscript t=30…65 indicates the time period, or age. If one suffers an illness in any period, he or she is henceforth permanently high-risk, facing an illness probability of p H =0.3, by assumption, for the remaining periods. Note that the loss probabilities we assume for high-risks is somewhat arbitrary: we do not possess actual high-risk probabilities by risk type. (Of course, information upon which empirical estimates of these high-risk probabilities – measured with error – would typically be available to insurers in practice.) Also, for illustrative convenience only, let us assume that year 65 is the last age period. In this model – which could be thought of as a cohort-type model of insurance – we assume that the majority of individuals start out as 30-year-old low-risk types. Then, using empirical data on the incidence of chronic illnesses, we use the age-specific risk of becoming chronically ill.
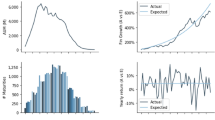
Following Herring and Pauly,Footnote 37 we include the following chronic illnesses: Cancer, diabetes, emphysema, high cholesterol, hyper-tension, heart disease, stroke, arthritis, asthma, gall bladder disease, stomach ulcer, and back problems. We use the probabilities constructed by Herring and Pauly.Footnote 38 These are the age-specific probabilities of chronic illness for low-risks. However, recall that persons suffering chronic illness in a given period are assumed permanently to be high-risk henceforth, so these probabilities also serve as the probabilities of becoming high-risk, or chronically ill. Herring and Pauly estimated the age-based probabilities of illness for low-risks from both the Medical Expenditure Panel Survey and the U.S. National Center for Health Statistics.Footnote 39 The probabilities are displayed in Figure 1 by the lowest line, labelled p Lt . Note that the older low-risks face approximately six times the probability of suffering a chronic illness in a period than do young-age low-risks. This also indicates that older low-risks have a six-fold chance of becoming high-risk in comparison to young low-risks.

LTC and chronic illness probabilities.
Community rating under the lifetime risk profile
In order to determine the community-rated premia, we use June 2000 to March 2003 Australian data on private health insurance coverage.Footnote 40 The Australian data provide the number of people insured by 5-year age groups, which we use to estimate the proportion insured in each age category.
p̄ represents the average expected risk of illness in the period for the pool of insurance buyers. Note that, due to adverse selection, the pooled risk for insurance purchasers is greater than the pooled risk for non-purchasers. The very low levels of coverage referred to above, a consequence of the advanced adverse selection problem associated with community rating, indicates that the risk pool in Australia has suffered. Therefore, we assume that a high proportion (somewhat arbitrarily, three-quarters) of all insurance buyers in each age class were high-risk in June 1999 when LTC began.Footnote 41 Of course, by definition, for adverse selection to occur in a two risk-types model, more than 50 per cent of the pool must be high-risk. Given the secular trends in the Australian market, our assumption is not unrealistic. Furthermore, we assume initially that all new joiners between June 2000, when LTC began, and March 2003 were low-risk types.Footnote 42
The community-rated base premium in our model varies, as it does in practice, with the age and risk composition of those who purchase health insurance. We calculate it as follows. For low-risk probabilities, we use a weighted average of low-risks by PHIAC 5-year age interval, as described above. The weights are the proportions of all individuals insured within each age interval.Footnote 43 Thus, if 5 per cent of the insurance buyers were in the age category 30–35 years, the probabilities for this age category were weighted 5 per cent. Thus, our stylized model captures the endogeneity of p̄. Note that because the loss is assumed for simplicity to be one, the community-rated premium is p̄ × 1 (we assume no loading). The probabilities, both high- and low-risk, are as defined in the prior section. We now turn to our representation of the LTC scheme and our proposed amendment to it, within the classic RS framework.
The RS framework
Australian health insurance markets can usefully be analysed via an application of the RSFootnote 44 framework at each age for each cohort. Recall that, in the RS model, (i) consumers are risk-averse expected utility-maximizers with state-independent and strictly concave and increasing von Neumann–Morgenstern utility functions, (ii) insurance firms are risk-neutral, (iii) insurance markets are competitive (with free entry), (iv) firms are expected profit maximizers (or are likely to behave as such in a well-organized competitive market), (v) consumers buy only one insurance contract, and (vi) risk status is known to consumers but not to producers of insurance. Along with the implicit assumption that contract provisions are unregulated, these assumptions imply inter alia that (vii) firms will offer only those contracts for which expected profits are nonnegative. Given that Australian firms are compelled to offer community-rated premia, assumption (vii) is assured. Furthermore, even though firm entry is difficult in Australian insurance markets, we assume zero profits. Since most Australian health insurance carriers are mutual firms, this is not a particularly objectionable assumption. We also assume that there is information asymmetry in these markets.
Following RS, uninsured low-risks and high-risks are assumed to be endowed with the state-contingent wealth E=(W, W−d), where W is wealth and d is the loss due to illness. The probabilities of illness are p lt if one is not chronically ill, or p H if one is chronically ill. As in RS, we assume a quasi-concave utility function of the following form:

where subscript i=lt, H, as described in the section “A lifetime risk profile”. We assume U(W s )=(W s )1/2, where s=1, 2.
Let us assume that W1=1.5 in the healthy state and W2=0.5 in the unhealthy state.
All odds ratios and indifference curves pass through point A in Figure 2 at point (1.5, 0.5). Indifference curves for low-risk types and high-risk types both intersect this point. These indifference curves illustrate utility corresponding to a world without insurance. Note that the steep, nearly straight, indifference curve labelled U lt corresponds to that of low-risk 30-year-olds. The flatter indifference curve labelled U H corresponds to high-risk consumers of any age. The solid line labelled (1−p̄)/p̄ is the community-rated odds ratio. Note that the low-risk 30-year-old will not buy insurance unless he or she is offered the contract given by the odds ratio with the dotted line. Figure 3 shows the high-risk indifference curve shifting out due to the purchase of the community-rated premium. The higher indifference curve for the high-risk types is now dashed and labelled U′ h . Of course, all high-risks buy: the figure confirms that adverse selection exists.

RS plot.

RS plot.
As in RS, we assume that firms do not know the risk status of a consumer but that the government does know the risk status. Note that this apparently strong assumption actually has the same effect as the existing regulatory environment for private health insurance in Australia. Specifically, to the extent that firms can observe individual risk, they are not permitted to act upon it in health insurance markets due to community-rating regulations. Furthermore, since the government regulates the policy inclusions and exclusions, it can (and does) curtail firms' attempts to cherry - pick or cream-skim.
The subsidy
Let s lt be the age-specific, ad valorem subsidy or tax at time t. With a loss of one, the premium is p̄ × 1, ignoring administrative loadings for simplicity. Therefore with the subsidy, the premium is (1−s lt ) × p̄.
One can solve for the subsidy by equating the marginal rate of substitution of wealth (MRS) in the good state and the bad state with the odds ratio offered by insurance. As shown in the previous section, only bad risks will buy insurance at the community-rated odds ratio. However, if the MRS is less than or equal to the odds ratio with the subsidy,

the person will fully insure. In order to minimize the necessary subsidy, it is necessary to set the MRS exactly equal to the odds ratio,

Solving for slt yields

Note that by adjusting subsidies so that the odds ratio is exactly equal to the MRS at full insurance, we ensure that low-risks will buy full insurance. On the other hand, if we lowered the subsidy at each age low-risks would either not fully insure, or not insure at all. Furthermore, if we increased the subsidy at each age, this would not increase insurance purchase by low-risks, who are already at full insurance with the subsidy given in equation (4). However, it would effectively lead to inefficient transfer payments to the low-risks.
Results
The age-based subsidy is given by the solid line in Figure 4. As one might expect, the required subsidy declines with age, because the probability of being low-risk itself declines with age. The saw-tooth nature of the plot arises due to measurement errors that are exacerbated by the use of the 5-year age groupings that were available to us. Econometric techniques exist which can be used to produce a linear or other approximation of the subsidy schedule. For the data presented in Figure 4, for example, we were able to fit a simple linear OLS model that explained more than 80 per cent of variation of the subsidy as a function of age. With the addition of moving average (MA) terms, we were able to explain more than 90 per cent of the plotted subsidy variance as a function of age. (The regression results are omitted in the interests of parsimony, but are available from the authors upon request.)

Subsidies to low-risk types by age
Although standard insurance theory suggests that welfare is maximized when all risk-averse agents buy insurance, the goal of the our proposal, like that of LTC, is not necessarily to ensure universal private insurance coverage. However, recall the endogeneity issue at work here: the risk composition of those with private insurance affects the community rated premium, which in turn affects the subsidy paid to low-risks. We now illustrate two polar scenarios: one where 33 per cent of the low-risks join and the other extreme where 100 per cent join. A consequence of our assumptions based on adverse selection is that the more who join under our subsidy scheme, the lower the community-rated premium. Let us suppose that everyone joins so that the risk pool improves.
p̄ is estimated based on the age distribution of the Australian population. As seen in Figure 5, the community-rated premium is lower. Thus, the slope of the community-rated odds ratio is steeper. Note that, not surprisingly, the low-risks do not buy insurance even though the community-rated premium is cheaper with everyone joining.

RS plot: everyone joins.
Of course, all high-risks buy full health insurance.
Note that due to our assumption of a loss equal to unity, the lower dashed line in Figure 4 represents the subsidies paid to low-risks when all low-risks join the insurance pool.
Discussion
Maintaining a public and private system of health insurance and health care is a goal of constituencies in many countries. With a private system, there may be advantages in terms of time cost savings, technological spread, and innovation, etc. However, the welfare-improving benefits of insuring against risk are largely addressed by the universal public health care system, the role emphasized in the extant literature. Instead, this paper addresses how to provide age- and risk-type-specific subsidies in order to maintain a viable private health insurance market and health care system.
The introduction of the Australian lifetime cover (LTC) scheme was an important step towards demonstrating that age-based penalties on older persons buying insurance, after not maintaining insurance, can be used to arrest adverse selection. However, it has been shown theoretically and empirically that the policy has not stabilized adverse selection.Footnote 45 In contrast, our scheme subsidizes private health insurance for low-risk types of all ages. By distinguishing low-risks from high-risks at all ages, our scheme does not discourage low-risk older persons who have not maintained insurance from buying insurance for the first time.
For decades, epidemiologists, and more recently, health economists, have questioned the conventional wisdom surrounding ageing and its implications for morbidity health costs in the future. The Australian LTC scheme ignores such considerations. Our subsidy scheme, in contrast, distinguishes between risk types by age, and can incorporate different assumptions about ageing, morbidity, and health expenditures. In these respects, our proposal results in a more efficient solution for Australian health care markets that accommodates the extant policy of mandated community rating while stabilizing coverage. In this respect, our work may represent a useful direction for other jurisdictions where, for whatever reason, policy-makers are committed to the pursuit of insurance policies that are not second-best efficient in the sense of Crocker and SnowFootnote 46 and Neudeck and Podczeck.Footnote 47
Notes
Ibid.
The extant literature, however, does not analyse the optimality of the subsidies within a general equilibrium context where other sectors are subject to market failure.
See e.g., Neudeck and Podczeck (1996).
Although Zweifel et al. (1999) did not reject the age-neutrality hypothesis in their pioneering work, the results of that study have subsequently been criticized on econometric grounds (Salas and Raftery (2001); Dow and Norton (2002)).
See Butler (1998a).
Ibid.
Ibid.
Ibid.
Ibid.
We note that in only one age category there was negative membership growth as a proportion of the pool during this period.
References
Anderson, R. (1998) ‘United States abridged life tables, 1996’, National Vital Statistics Reports, vol. 47, Atlanta: Centers for Disease Control and Prevention's National Center for Health Statistics, pp. 1–20.
Australian Institute of Health and Welfare (2000) Australia's Health 2000: The Seventh Biennial Health Report of the Australian Institute of Health and Welfare, Technical report, Canberra: Australian Institute of Health and Welfare.
Brown III, H.S. and Connelly, L.B. (2005) ‘Lifetime cover in private insurance markets’, International Journal of Health Care Finance and Economics 5: 75–88.
Busse, R., Krauth, C. and Schwartz, F. (2002) ‘Use of acute hospital beds does not increase as the population ages: Results from a seven year cohort study in Germany’, Journal of Community Health 56: 289–293.
Butler, J. (1998a) ‘Health expenditure’, in G. Mooney and R.B. Scotton (eds.) Economics and Australian Health Policy, Crows Nest, Australia: Allen and Unwin, pp. 40–71.
Butler, J. (1998b) ‘Policy change and private health insurance: Did the cheapest policy do the trick?’ Australian Health Review 25: 33–41.
Butler, J. (1999) Estimating elasticities of demand for private health insurance in Australia, NCEPH Working Paper No. 43, Canberra: National Centre for Epidemiology and Population Health.
Commonwealth of Australia (1999) ‘Bills digest no. 13 1999–2000 National Health Amendment (Lifetime Health Cover)’, Canberra: Department of the Parliamentary Library.
Crocker, K. and Snow, A. (1985) ‘A simple tax structure for competitive equilibrium and redistribution in insurance markets with asymmetric information’, Southern Economic Journal 26: 1142–1150.
Dow, W.H. and Norton, E.C. (2002) The red herring that eats cake: Heckit versus two-part model redux, Triangle Health Economics Working Paper Series, No. 1, University of North Carolina at Chapel Hill.
Felder, S., Meier, M. and Schmitt, H. (2000) ‘Health care expenditure in the last months of life’, Journal of Health Economics 19: 679–695.
Hall, J., Abreu, L.D. and Viney, R. (1999) ‘Carrots and sticks – the fall and fall of private health insurance in Australia’, Health Economics 8: 653–660.
Herring, B. and Pauly, M. (1999) ‘Premium variation in the individual health insurance market’, International Journal of Health Care Finance and Economics 1: 43–58.
Herring, B. and Pauly, M. (2003) Incentive-compatible guaranteed renewable health insurance premiums, NBER Working Paper.
Industry Commission (1997) Private Health Insurance, Technical report, Canberra: Industry Commission.
Michel, J.-P. and Robine, J.-M. (2004) ‘A “new” general theory of population ageing’, The Geneva Papers on Risk and Insurance — Issues and Practice 29(4): 667–678.
Neudeck, W. and Podczeck, K. (1996) ‘Adverse selection and regulation in health insurance markets’, Journal of Health Economics 15: 387–408.
Pauly, M., Hirth, R. and Kunreuther, H. (1995) ‘Guaranteed renewability in insurance’, Journal of Risk and Uncertainty 10: 143–156.
PHIAC (2002) Coverage of Hospital Insurance Tables Offered by Registered Health Benefits Organisations By Age Cohort, http://www.phiac.gov.au/statistics/membershipcoverage/agecohort.htm, Accessed 10 June 2003, PHIAC.
Rothschild, M. and Stiglitz, J. (1976) ‘Equilibrium in competitive insurance markets: An essay on the economics of imperfect information’, Quarterly Journal of Economics 90: 630–649.
Salas, C. and Raftery, J.P. (2001) ‘Econometric issues in testing the age neutrality of health care expenditure’, Health Economics 10: 669–671.
Seshamani, M. and Gray, A. (2004a) ‘Ageing and health-care expenditure: The red herring argument revisited’, Health Economics 13: 303–314.
Seshamani, M. and Gray, A.M. (2004b) ‘A longitudinal study of the effects of age and time to death on hospital costs’, Journal of Health Economics 23: 217–235.
Stearns, S.C. and Norton, E.C. (2004) ‘Time to include time to death? The future of health care expenditure predictions’, Health Economics 13: 315–327.
Zweifel, P., Felder, S. and Meier, M. (1999) ‘Ageing of population and health care expenditure: A red herring?’, Health Economics 8: 485–496.
Zweifel, P., Felder, S. and Meier, M. (2001) ‘Reply to: Econometric issues in testing the age neutrality of health care expenditure’, Health Economics 10: 673–674.
Zweifel, P., Felder, S. and Werblow, A. (2004) ‘Population ageing and health care expenditure: New evidence on the “red herring”’, The Geneva Papers on Risk and Insurance — Issues and Practice 29(4): 652–666.
Author information
Authors and Affiliations
Additional information
*Support for Dr. Brown came from the Hispanic Health Research Center, supported by NIH CMHD P20 MD000170-03 located at the Brownsville Regional Campus of the University of Texas School of Public Health.
Rights and permissions
About this article
Cite this article
Connelly, L., Shelton Brown, H. Lifetime Subsidies in Australian Private Health Insurance Markets with Community Rating. Geneva Pap Risk Insur Issues Pract 31, 705–719 (2006). https://doi.org/10.1057/palgrave.gpp.2510099
Published:
Issue Date:
DOI: https://doi.org/10.1057/palgrave.gpp.2510099