
Abstract
Data sources
The Cochrane Oral Health Group's Trials Register, Cochrane Central Register of Controlled Trials (CENTRAL), Medline and Embase databases were searched with no language or date restrictions.
Study selection
Two reviewers independently selected studies. Randomised controlled trials (RCTs) of different techniques and materials for augmenting the maxillary sinus for rehabilitation with dental implants that reported the outcome of implant success or failure at least four months after initial loading were considered.
Data extraction and synthesis
Data were extracted independently by two reviewers and study risk of bias assessed. Results were expressed using fixed-effect models as there were either fewer than four studies or we used Peto odds ratios (ORs) for dichotomous data when there were zero cells in either the treatment or control or both arms and the number of trials was small.
Results
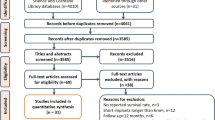
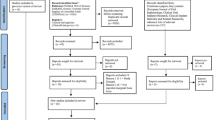
Eighteen trials involving 650 patients were included. Five studies were considered to be at low risk of bias, 11 at high risk and two of unclear risk. Four trials (102 patients) evaluated short implants (5 to 8.5 mm long) as an alternative to sinus lift in bone with residual height between 4 and 9 mm. One year after loading there was insufficient evidence to claim differences between the two procedures for prosthesis failure (OR (Peto) 0.37, 95% confidence interval (CI) 0.05 to 2.68; three trials) or implant failure (OR (Peto) 0.44, 95% CI 0.10 to 1.99; four trials). There was however an increase in complications at treated sites when undertaking the sinus lift (OR (Peto) 4.77, 95% CI 1.79 to 12.71, P value = 0.002; four trials).
Fourteen trials (548 patients) compared different sinus lift techniques. Only three comparisons included more than one trial. These were bone graft versus no bone graft, autogenous bone versus bone substitute, bone graft with or without platelet-rich plasma (PRP). There was insufficient evidence to claim a benefit for any of these techniques for the primary outcomes of prosthesis and implant failure.
The other comparisons with single studies were rotary versus piezosurgery to open a lateral sinus window, two different bone substitutes, use or not of a membrane to seal the lateral window, one- versus two-stage lateral sinus lift, two-stage granular bone versus one-stage autogenous bone blocks and crestal versus lateral sinus lift; two trials compared three different crestal sinus lifting techniques: rotatory versus hand malleting (patients preferred rotatory instruments over hand malleting) and hand versus electric malleting. There was no evidence of a benefit for any sinus lift procedure compared to any other for the primary outcomes prosthesis or implant failure.
Conclusions
There is moderate quality evidence which is insufficient to determine whether sinus lift procedures in bone with residual height between 4 and 9 mm are more or less successful than placing short implants (5 to 8.5 mm) in reducing prosthesis or implant failure up to one year after loading. However, there are more complications at sites treated with sinus lift procedures. Many trials compared different sinus lift procedures and none of these indicated that one procedure reduced prosthetic or implant failures when compared to the other. Based on low quality evidence, patients may prefer rotary instruments over hand malleting for crestal sinus lift.
Similar content being viewed by others
Commentary
Implant therapy has improved the treatment outcomes for restoring missing teeth in the past decades. The key factors for long-term implant survival are bone quantity and quality. Furthermore, the rehabilitation with implant-supported prostheses of the edentulous in the posterior maxillary regions often presents a challenge due to reduced residual alveolar bone and increased pneumatisation of the maxillary sinus. In many of these patients, sinus augmentation procedure has been used to overcome this problem by using bone grafting. Over the last ten years, maxillary sinus augmentation procedure has become a routine indication to increase the available bone height for implant placement and subsequent prosthetic reconstruction.
Evidence-based reviews reported and compared implant survival rates in augmented sinuses utilising various surgical techniques, implant surfaces and grafting materials.1,2 These reviews concluded that maxillary sinus augmentation can be a predictable grafting procedure for placing dental implants in the severely atrophic posterior maxilla. However, the possibility of surgical complications exists and should be considered.
Some alternative approaches have been utilised to overcome the problem of inadequate bone quantity including, but not limited to, the use of a short implant (4 to 8 mm long). The main advantage of a short implant is that it avoids the need for entering the sinus cavity and use of bone graft, although a minimum of 5-6 mm of residual bone height is still required. However, a critical clinical question is whether implants placed in a grafted sinus present a higher risk of failure than the use of short implants in posterior atrophic maxillae. This is why this is a clinically relevant topic so as to clarify the specific indications for each treatment.
In 2014, an update3 of a Cochrane review first published in 20104 from the Cochrane Oral Health Group compared the predictability of bone augmentation to no augmentation when undertaking sinus lift procedures. In addition to that, they compared different maxillary sinus augmentation techniques for implant rehabilitation. It was conducted with an appropriate methodology, with no restrictions on language or date of publication, databases were search, a thorough critical appraisal was performed. A grade of the evidence for each outcome was presented using the GRADE profiler, summarising the findings, quality of evidence and strength of the recommendations. The authors' grading for the overall risk of selection bias was moderate. It concluded that there is insufficient evidence to determine whether sinus lift procedures in bone with residual height are more or less successful than placing short implants in reducing prosthesis or implant failures. Only a few studies were included in the meta-analysis for prosthetic and implant failures. The combined statistics of similar studies (low heterogeneity) shows no statistically significant results. There is also insufficient evidence to conclude that different sinus lift procedures lead to fewer prosthesis or implant failures than the other. However, there was some statistically significant difference observed among studies of increased complications at sites involving sinus lift procedures. The overall result is statistically significant. However, a large confidence interval is noted and some statistical heterogeneity was observed in the meta-analysis. The clinical applicability of the results is inconclusive.
Given the lack of evidence, and small number included in the meta-analysis, larger, long-term, well designed controlled clinical trials are needed.
Therefore, clinicians may treat suitable patients with severely atrophic posterior maxilla when a methodical preoperative evaluation is performed, including careful case planning, surgical technique and biomaterial selection. Finally, the validity of new procedures specifically to treat these regions must be fully evaluated.
References
Del Fabbro M, Rosano G, Taschieri S . Implant survival rates after maxillary sinus augmentation. Eur J Oral Sci 2008; 116: 497–506.
Pjetursson BE, Tan WC, Zwahlen M, Lang NP . A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. J Clin Periodonto. 2008; 35: 216–240.
Esposito M, Felice P, Worthington HV . Interventions for replacing missing teeth: augmentation procedures of the maxillary sinus. Cochrane Database Syst Rev 2014; 5: CD008397. doi: 10.1002/14651858. CD 008397. pub2.
Esposito M, Grusovin MG, Rees J, et al. Interventions for replacing missing teeth: augmentation procedures of the maxillary sinus. Cochrane Database Syst Rev 2010; 3: CD008397. doi: 10.1002/14651858.CD008397. Review. Update in: Cochrane Database Syst Rev 2014; 5: CD008397.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Luisa Fernandez Mauleffinch, Review Group Co-ordinator, Cochrane Oral Health Group, School of Dentistry, The University of Manchester, Coupland III Building, Oxford Road, Manchester, M13 9PL, UK. E-mail: luisa.fernandez@manchester.ac.uk
Esposito M, Felice P, Worthington HV. Interventions for replacing missing teeth: augmentation procedures of the maxillary sinus. Cochrane Database Syst Rev 2014; 5: Art. No.CD008397. DOI: 10.1002/14651858.CD008397.pub2.
This paper is based on a Cochrane Review published in the Cochrane Library 2014, issue 5 (see www.thecochranelibrary.com for information). Cochrane Reviews are regularly updated as new evidence emerges and in response to feedback, and the Cochrane Library should be consulted for the most recent version of the review.
Rights and permissions
About this article

Cite this article
Khouly, I., Veitz-Keenan, A. Insufficient evidence for sinus lifts over short implants for dental implant rehabilitation. Evid Based Dent 16, 21–22 (2015). https://doi.org/10.1038/sj.ebd.6401081
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401081
