
Abstract
BHD, TP53, and HNF1β on chromosome 17 were studied in 92 cases of renal cell carcinoma (46 chromophobe, 19 clear cell, 18 oncocytoma, and nine papillary). Six, thirteen, and zero cases had, respectively BHD, TP53, and HNF1β mutations, (84% mutations involved chromophobe), suggesting a role for BHD and TP53 in chromophobe subtype.
Similar content being viewed by others


Main
Renal cell carcinoma (RCC) is mainly comprised of clear cell, papillary, and chromophobe subtypes. The study of hereditary kidney cancer syndromes has led to the identification of kidney cancer-related genes that are also involved in sporadic RCC. Recently, germline BHD mutations were found in patients with Birt–Hogg–Dubé (BHD) syndrome (Nickerson et al, 2002), and a diverse spectrum of renal tumours have been described with somatic inactivation of BHD reported in BHD-related renal tumours (Khoo et al, 2002; Schmidt et al, 2005; Vocke et al, 2005). BHD promoter methylation has been reported in a subset of sporadic clear cell and chromophobe RCC, but somatic mutation of BHD in sporadic cases is rare (da Silva et al, 2003; Khoo et al, 2003). BHD is located at 17p11.2, and LOH has been detected in all RCC subtypes (Khoo et al, 2003; Vocke et al, 2005). The TP53 gene is located at 17p13.1 near BHD. A study has reported 30% of somatic missense mutations of TP53 in chromophobe with LOH of chromosome 17p, suggesting that TP53 plays a role in this subtype (Contractor et al, 1997). The HNF1β gene (hepatocyte nuclear factor), which was found mutated in patients with maturity-onset diabetes of the young (MODY5), is located at 17q12 (Horikawa et al, 1997). Biallelic inactivation of this gene has been reported in two of 12 patients with chromophobe RCC; both patients have germline HNF1β mutations, and their tumours showed LOH, suggesting inactivation through the classic two-hit hypothesis (Rebouissou et al, 2005).
Multiple losses of whole chromosomes were frequently found in chromophobe RCC, especially in chromosome 17 (Speicher et al, 1994). We hypothesised that the lost chromosomal regions may harbour chromophobe RCC-specific tumour suppressor genes, and their inactivation contributes to the tumorigenesis. Here, we focused on three cancer-related genes located at chromosome 17, BHD, TP53, and HNF1β, and examined their involvement in chromophobe RCC by studying 46 cases and compared with 19 clear cell, 18 oncocytoma, and nine papillary subtypes. We screened these tumours for mutations, evaluated the BHD promoter methylation status, and estimated the allelic frequencies of polymorphisms in these genes.
Materials and methods
Tissue samples and DNA extraction
Ninety-two frozen sporadic renal tumour samples were collected from various hospitals in France and USA (French Kidney Tumour Consortium and Cooperative Human Tissue Network). All patients are of Caucasian origin. This included two patients with bilateral chromophobe RCC but without evidence of genetic predisposition. This study was performed after approval from our local Ethics Committee. Informed consent was obtained from each patient. Genomic DNA was extracted using the QIAamp DNA Mini Kit (Qiagen, Courtaboeuf, France) according to the manufacturer's instructions.
Sequencing analysis
The entire coding region of BHD, TP53, and HNF1β was screened for mutations by direct sequencing (Nickerson et al, 2002; B. Bressac-de Paillerets, unpublished data; Rebouissou et al, 2005; see Supplementary Information).
SNP analysis
Intronic and exonic SNPs (iSNPs and eSNPs) were obtained from the sequencing results. Rare homozygous genotypes have the lowest allelic frequencies according to the Hardy–Weinberg's law. We used the allelic frequencies of HapMap–CEU (http://www.hapmap.org).
Methylation analysis of the BHD promoter region
Genomic DNA were incubated with or without HpaII (Invitrogen, Cergy-Pontoise, France). Polymerase chain reaction (PCR) was then performed with specific primers (available on request) and products were analysed on standard agarose gels. The presence of methylated cytosines was determined by comparing the same sample under the digested or nondigested conditions, that is, if cytosines were methylated, HpaII would not be cleaved at the restriction enzyme sites, and PCR amplification would be successful.
Statistical analysis
χ2 test was used to compare the mutation frequencies as well as the frequencies of rare homozygous genotypes of each polymorphism in each tumour subtype. When the conditions of application of χ2 could not be obtained, a Yates's correction was applied, or the Fisher's exact test was used. Statistical significance was indicated by P<0.05.
Results and discussion
Alterations in BHD
Two nonsense, three frameshift, and three predicted splice mutations were identified in six samples, five of 46 chromophobe RCC (10.9%) and one of 18 oncocytomas (5.6%) (Table 1). This is the first report of somatic BHD mutations in sporadic chromophobe RCC and renal oncocytoma. T16 and T35 exhibited their respective mutations in both tumour and corresponding matched normal tissue, showing possible germline mutations, although contamination of tumour cells in the normal tissue could not be ruled out completely. Unfortunately, the blood DNA of these patients could not be obtained to verify their germline mutation status. T16 also showed loss of the wild-type allele but retained mutant strand in its tumour tissue (LOH) (Figure 1A). Two chromophobe RCC (T68 and T87b) showed a double mutation in each of the tumours. In patient A (T87a and T87b), we detected two novel somatic mutations and a previously described germline alteration (Schmidt et al, 2005), which was confirmed with the patient's blood DNA. Although patient A did not show any evidence of genetic predisposition, he has bilateral chromophobe RCC, and a germline mutation makes him a potential hereditary case and was referred to genetic counsellors. T68 showed two distinct somatic mutations not found in the matched normal tissues. The second somatic mutation is a possible second hit, instead of LOH, further supporting the tumour suppressive role of BHD. We did not detect any mutation at the hot spot within exon 11 as reported in BHD patients. The BHD mutation frequency in chromophobe is statistically not significant compared to the other subtypes (P>0.20, with Yates's correction). Methylation status of the BHD promoter was analysed on 61 of 92 samples (39 chromophobe, seven clear cell, and 15 oncocytoma), which had sufficient DNA quantity to perform the enzymatic digestion. No evidence of BHD promoter methylation was found.

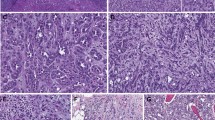
Sequence chromatograms for BHD, TP53, and HNF1β. R, N, and T are DNA from a commercially available reference, the normal tissue and its matched tumour tissue, respectively. (A) Corresponds to BHD with a somatic mutation (T68, c.1433(IVS12)-2A>T) (left) and a possible germline mutation (T16, c.103_125(558_580)del23) (right). (B) Corresponds to TP53 with a somatic mutation (T72, c.393_395delCAA) (left) and a possible germline mutation (T9, c.467G>A) (right). (C) Corresponds to HNF1β with a cytosine insertion in intron 8 (left) and a SNP in the non-coding region of exon 9 (c.*99C>) (right).
Mutations in TP53
Eight missense, three frameshift, one in-frame, and one predicted splice mutations were identified in 13 tumours, 11 of 46 chromophobe (23.9%), one of 19 clear cell (5.3%), and one of nine papillary RCC (11.1%). The mutation in T75 is located at the last base of exon 4 that can induce a splicing effect (Holmila et al, 2003). A known hot spot mutation in sarcomatoid RCC (Oda et al, 1995) has been detected in one papillary (T26) and one chromophobe (T63). A sarcomatoid component can occur in all subtypes, and its presence indicates poor outcome (Cheville et al, 2004). The matched normal tissue of T9, a clear cell subtype, has the same mutation as its tumour tissue, suggesting a possible germline mutation (Figure 1B). However, no blood DNA was available to confirm its germline status. All TP53 mutations detected here have been described in the TP53 database (www-p53.iarc.fr/P53aim.html). The TP53 mutation frequency in chromophobe is statistically significant compared to the other subtypes (P<0.01). Therefore, TP53 mutations occur preferentially in chromophobe as reported (Contractor et al, 1997). The high percentage of TP53 mutations in chromophobe could reflect the different pathways in its tumorigenesis, compared to other subtypes.
Analysis of HNF1β
No mutations were identified in all coding exons of the HNF1β gene. However, an insertion of a cytosine in the intron 8 was detected (Table 2, and Table 3 in Supplementary Information). This is a deletion/insertion polymorphism (DIP) that has been reported previously (Horikawa et al, 1997). Here the frequency of its rare genotype (insC) in chromophobe is statistically significant compared to the other subtypes (P<0.02). Furthermore, this variant was observed in a normal tissue sample, but was lost in the matched tumour through LOH (Figure 1C). We could not establish any relationship between HNF1β and sporadic RCC as we did not find any mutations, suggesting HNF1β mutation as a very rare genetic event in sporadic renal tumours.
Analysis of SNPs in BHD, TP53, and HNF1β
We detected 14 SNPs, including one possible new iSNP in BHD (Table 2 and Supplementary Table 3). All tumours that carry the BHD mutations showed homozygosity in all four iSNPs. All except two TP53-mutated tumours (T26 and T45) demonstrated homozygous alleles in all four SNPs. In addition, the proportion of samples showing homozygous SNP alleles in BHD, TP53, and HNF1β are 41/92 (44.6%), 65/92 (70.6%), and 37/92 (40.2%), respectively. Chromophobe RCC exhibited the highest percentage of rare homozygous genotypes (Table 2). Among the 92 renal tumours, 24 samples are homozygous for all SNP studied (26%). Twenty-one of them are of chromophobe subtype (45.6% of all chromophobe; P<0.001). One of them carries a BHD mutation and eight of them have TP53 mutations (72.7% of TP53-mutated chromophobe; P<0.02). The other three are of oncocytoma subtype (16.7% of all oncocytoma). Homozygous SNP alleles detected in this study may indicate chromosomal deletions. In samples with mutations, it may suggest LOH, which is consistent with the two-hit hypothesis. However, we also noticed the high frequency of homozygous SNP alleles especially in samples without TP53 mutation (70%). Although it has been shown that p53 is functional in p53 wild-type RCC cells (Warburton et al, 2005), the relationship between chromosomal 17 deletions and TP53, especially in sporadic chromophobe subtype, is worth further investigation.
In summary, BHD and TP53 may play an important role as tumour suppressors in chromophobe RCC.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Cheville JC, Lohse CM, Zincke H, Weaver AL, Leibovich BC, Frank I, Blute ML (2004) Sarcomatoid renal cell carcinoma: an examination of underlying histologic subtype and an analysis of associations with patient outcome. Am J Surg Pathol 28: 435–441
Contractor H, Zariwala M, Bugert P, Zeisler J, Kovacs G (1997) Mutation of the p53 tumour suppressor gene occurs preferentially in the chromophobe type of renal cell tumour. J Pathol 181: 136–139
da Silva NF, Gentle D, Hesson LB, Morton DG, Latif F, Maher ER (2003) Analysis of the Birt–Hogg–Dube (BHD) tumour suppressor gene in sporadic renal cell carcinoma and colorectal cancer. J Med Genet 40: 820–824
Holmila R, Fouquet C, Cadranel J, Zalcman G, Soussi T (2003) Splice mutations in the p53 gene: case report and review of the literature. Hum Mutat 21: 101–102
Horikawa Y, Iwasaki N, Hara M, Furuta H, Hinokio Y, Cockburn BN, Lindner T, Yamagata K, Ogata M, Tomonaga O, Kuroki H, Kasahara T, Iwamoto Y, Bell GI (1997) Mutation in hepatocyte nuclear factor-1 beta gene (TCF2) associated with MODY. Nat Genet 17: 384–385
Khoo SK, Giraud S, Kahnoski K, Chen J, Motorna O, Nickolov R, Binet O, Lambert D, Friedel J, Levy R, Ferlicot S, Wolkenstein P, Hammel P, Bergerheim U, Hedblad MA, Bradley M, Teh BT, Nordenskjold M, Richard S (2002) Clinical and genetic studies of Birt–Hogg–Dube syndrome. J Med Genet 39: 906–912
Khoo SK, Kahnoski K, Sugimura J, Petillo D, Chen J, Shockley K, Ludlow J, Knapp R, Giraud S, Richard S, Nordenskjold M, Teh BT (2003) Inactivation of BHD in sporadic renal tumors. Cancer Res 63: 4583–4587
Nickerson ML, Warren MB, Toro JR, Matrosova V, Glenn G, Turner ML, Duray P, Merino M, Choyke P, Pavlovich CP, Sharma N, Walther M, Munroe D, Hill R, Maher E, Greenberg C, Lerman MI, Linehan WM, Zbar B, Schmidt LS (2002) Mutations in a novel gene lead to kidney tumors, lung wall defects, and benign tumors of the hair follicle in patients with the Birt’Hogg–Dube syndrome. Cancer Cell 2: 157–164
Oda H, Nakatsuru Y, Ishikawa T (1995) Mutations of the p53 gene and p53 protein overexpression are associated with sarcomatoid transformation in renal cell carcinomas. Cancer Res 55: 658–662
Rebouissou S, Vasiliu V, Thomas C, Bellanne-Chantelot C, Bui H, Chretien Y, Timsit J, Rosty C, Laurent-Puig P, Chauveau D, Zucman-Rossi J (2005) Germline hepatocyte nuclear factor 1alpha and 1beta mutations in renal cell carcinomas. Hum Mol Genet 14: 603–614
Schmidt LS, Nickerson ML, Warren MB, Glenn GM, Toro JR, Merino MJ, Turner ML, Choyke PL, Sharma N, Peterson J, Morrison P, Maher ER, Walther MM, Zbar B, Linehan WM (2005) Germline BHD-mutation spectrum and phenotype analysis of a large cohort of families with Birt–Hogg–Dube syndrome. Am J Hum Genet 76: 1023–1033
Speicher MR, Schoell B, du Manoir S, Schrock E, Ried T, Cremer T, Storkel S, Kovacs A, Kovacs G (1994) Specific loss of chromosomes 1, 2, 6, 10, 13, 17, and 21 in chromophobe renal cell carcinomas revealed by comparative genomic hybridization. Am J Pathol 145: 356–364
Vocke CD, Yang Y, Pavlovich CP, Schmidt LS, Nickerson ML, Torres-Cabala CA, Merino MJ, Walther MM, Zbar B, Linehan WM (2005) High frequency of somatic frameshift BHD gene mutations in Birt–Hogg–Dube-associated renal tumors. J Natl Cancer Inst 97: 931–935
Warburton HE, Brady M, Vlatkovic N, Linehan WM, Parsons K, Boyd MT (2005) p53 regulation and function in renal cell carcinoma. Cancer Res 65: 6498–6503
Acknowledgements
We thank S Rebouissou and J Zucman-Rossi regarding HNF1β study, and B Gardie and J Feunteun for critical reading of the manuscript. We also thank the Service de Génétique (Institut Gustave Roussy) for their assistance in direct sequencing. This work was supported by grants from the Ligue Nationale Contre le Cancer (Comités de l'Allier, du Cher et de l'Indre) and Institut National du Cancer (the French NCI). We are grateful to the patients for their cooperation and participation in this study. Finally, we want to thank Cooperative Human Tissue Network and the following foundations: Hauenstein, Gerber, Schregardus, and Amway Japan.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supplementary Information accompanies the paper on British Journal of Cancer website (http://www.nature.com/bjc)
Supplementary information
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Gad, S., Lefèvre, S., Khoo, S. et al. Mutations in BHD and TP53 genes, but not in HNF1β gene, in a large series of sporadic chromophobe renal cell carcinoma. Br J Cancer 96, 336–340 (2007). https://doi.org/10.1038/sj.bjc.6603492
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6603492
Keywords
This article is cited by
-
The tumor suppressor folliculin inhibits lactate dehydrogenase A and regulates the Warburg effect
Nature Structural & Molecular Biology (2021)
-
Renal Cell Carcinoma: Molecular Aspects
Indian Journal of Clinical Biochemistry (2018)
-
Renal cell cancers: unveiling the hereditary ones and saving lives—a tailored diagnostic approach
International Urology and Nephrology (2017)
-
A review on hepatocyte nuclear factor-1beta and tumor
Cell & Bioscience (2015)
-
Molecular genetics and clinical features of Birt–Hogg–Dubé syndrome
Nature Reviews Urology (2015)
