
Key Points
-
Identifies factors affecting performance and survival of resin-bonded bridges provided for hypodontia patients.
-
Outlines appropriate statistical analysis for a retrospective study of this nature.
-
Highlights the interdisciplinary management of hypodontia patients.
Abstract
Objective To analyse the clinical performance and factors influencing the survival of resin-bonded bridgework provided for hypodontia patients with missing maxillary lateral incisors, following orthodontic treatment to open, maintain or redistribute the missing tooth space.
Design A retrospective analysis of patients treated at a single centre using case notes with all patients invited for review to corroborate findings.
Setting Departments of Orthodontics, Child Dental Health and Restorative Dentistry, Newcastle upon Tyne Dental Hospital and School.
Subjects and methods Between 1989-2000, 59 suitable hypodontia patients were identified of whom 45 had complete records. For these patients 73 resin-bonded bridges (RBBs) were provided. Following invitation, 24 patients attended for a review appointment. The survival of the RBBs, grade of operator providing treatment, duration of post-orthodontic retention, the influence of design, presence of pontic contact in static and dynamic excursions, and the effect of habits were assessed. Life table, Kaplan-Meier and Cox regression analysis were carried out for the 73 RBBs with complete records. A separate analysis of the RBBs provided for patients who attended for the invited review did not show a higher failure rate than those patients who did not attend. Therefore both sets of data were combined.
Results Of the 73 RBBs provided, 30 had debonded on at least one occasion (41.1%), six of these debonds were due to trauma (20%). The mean survival time of all the restorations was 59.3 months, with a median survival time of 59 months. Senior members of staff (Consultant, Senior Lecturer or Specialist Trainee) provided most restorations (n = 39) and achieved the highest mean survival of 72.6 months and median survival time of 100+ months. RBBs provided by junior staff and students had significantly lower survival times (p <0.05) compared with senior staff. Risk of failure was 3.9 times greater with junior staff and 2.5 times greater with students (p = 0.01 and p = 0.02, respectively). Analysis of all the other factors investigated showed no statistical difference in survival times or in hazard ratios. Analysis of fixed/fixed versus cantilevered bridges was limited by the number of fixed/fixed bridges (n = 11), and only two cantilevered bridges with multiple abutments were provided; both failed within one month.
Conclusion RBBs provided for post-orthodontic hypodontia patients with missing maxillary lateral incisors can for many patients be an acceptable and definitive restoration. Experienced staff achieved the best results, but why this should be was not explained by the individual factors analysed in this study.
Similar content being viewed by others

Introduction
Hypodontia is a condition where one or more teeth are developmentally absent (normally excluding third molars) and may present with varying degrees of severity.1 The prevalence in those of Northwest European origin has been shown to be in the order of 0.1-0.9% for the primary dentition and 3.5-10% for the permanent dentition.2,3,4,5 Approximately 20% of all congenitally missing teeth are maxillary lateral incisors, being the second most common missing tooth after mandibular second premolars.4,6
There are several treatment options for managing missing lateral incisors. These can vary from no treatment at all and accepting a space,7,8 to orthodontically closing a space,9,10,11,12,13 or orthodontically opening, maintaining or redistributing a tooth space in preparation for its prosthetic replacement.14,15,16,17 The treatment that is provided can involve multiple dental specialties and is dependent on a number of issues. Patient related factors include age, attitude and expectations; orthodontic factors include the severity of the hypodontia, type, and degree of malocclusion; further consideration also has to be given to the occlusion and the aesthetics.7,18,19,20,21
There have been numerous studies investigating resin-bonded bridges (RBBs) since their introduction almost 30 years ago.22,23 It has been shown that they can provide long term service,24,25,26,27,28 patients are highly satisfied with the results,29 and they are an acceptable alternative to conventional bridgework.28,30 Maxillary RBBs have significantly lower failure rates when compared to mandibular RBBs,31,32,33 and anterior RBB performance is more superior than posterior RBB performance.26,34,35 Further studies have found failure rates to be reduced when cantilever designs are used in preference to fixed/fixed designs.36,37
Although all this evidence suggests that the RBB is an acceptable form of treatment, there is little evidence about the survival and clinical performance of RBBs when provided specifically for post-orthodontic hypodontia patients, and in particular the survival of RBBs replacing the commonly missing maxillary lateral incisor. There has been contradicting evidence, with one study showing that if orthodontic treatment has been carried out immediately before RBB placement, the median survival time may be significantly reduced.38 Whereas a further study has shown that orthodontic tooth movement of abutment teeth does not result in an increased risk of failure.28 It is still unclear what duration of post-orthodontic retention is required, if any, to secure the longevity of the restoration.
The aims of this study were to retrospectively assess the range of RBB designs provided by an interdisciplinary hypodontia clinic for patients with missing maxillary lateral incisors, analyse the clinical performance of RBBs, and determine what factors may influence the survival. An important feature of the study was the systematic review of patients to supplement case note information.
Method
Sample
For the period 1989-2000, orthodontic and prosthodontic laboratory databases were used to identify 59 hypodontia patients who had received either unilateral or bilateral RBBs to replace a missing maxillary lateral incisor(s). They had received orthodontic treatment to open, redistribute or maintain the missing tooth space.
From this group, 45 patients (76.3%) were selected for whom 73 RBBs were provided, all of which had good quality pre- and post-orthodontic study casts and well-documented case records. The case records included pre-orthodontic assessment details, orthodontic treatment and review details, and restorative treatment and review details. Both the orthodontic and restorative treatment was provided at Newcastle upon Tyne Dental Hospital and School, and all of the patients had completed active treatment.
Data collection
From the case records the following information was recorded:
-
1
patient details – age, gender, and number of upper lateral incisors missing
-
2
orthodontic details – skeletal and incisor relationships, type of appliance used and treatment time
-
3
post-orthodontic retention details – type of appliance and duration of retention
-
4
RBB details – date and patient age at fitting, design, tooth retainers, presence of tooth preparation, cement used, and use of rubber dam
-
5
RBB bond history – number of debonds, rebonds and remakes, and reasons for failure
-
6
grade of clinician providing RBB – supervised student, junior member of staff (General Professional Trainee or Senior House Officer), or senior member of staff (Consultant, Senior Lecturer, Specialist Trainee).
The selected 45 patients were invited to be reviewed by one of the authors (MJG) and the following information was verified for the 24 who attended:
-
1
RBB bond history – it was possible to confirm with the patient the findings from the clinical records for number of debonds, rebonds and remakes
-
2
habit details – history of nail biting, clenching and grinding, pen chewing or any other dental related habit was recorded.
A full clinical examination was carried out and the following assessments were made:
-
1
clinical assessment – for retainer lute debond, caries and porcelain fractures
-
2
occlusal assessment – the presence of pontic contact in the intercuspal position, pontic contact in excursive lateral movements and protrusive movements, was confirmed using 12 μm occlusion foil (Roekko, Langenau, Germany).
Statistical analysis
Life tables and the survival estimation method of Kaplan and Meier39 were used to characterise the service that might be expected from the RBBs. The Cox regression model40 was then used to evaluate the influence of the different parameters on the RBB survival. Data was analysed using the software Statistical Programme for Social Sciences (SPSS) for Windows V10.0™. Each RBB was categorised as either 'failed' or 'censored' and a survival time was calculated for each:
Failed – a RBB 'failed' if there had been debond of one or more retainers on at least one occasion, with the bridge subsequently needing to be rebonded or remade. The debond failure was either due to non-traumatic, or traumatic adhesive/cohesive failure of the lute. The survival time for a failed bridge was calculated (in months) as the interval between the fit date and the date of failure.
Censored – a censored RBB was still in place and had not failed at the time of the review assessment (censor date). For the patients who failed to attend for a review, their censor date was the last known documented entry in the clinical notes. Following a censor date any further survival would be unknown and the restoration may still be in place or may have failed. A censored restoration's survival time was calculated as the interval between the fit date and the last known activity of the restoration, either as a routine review or as a review assessment as part of the study.
Life table – (Table 1) is a method to analyse the cumulative survival (column F) of restorations at specific time intervals (column A). It takes into account the number of restorations entering the specific time intervals (column B), the number failing (column C) and the number censored (column D). From these figures, the number of restorations exposed to risk can be calculated (column E); this is the number of cases that have entered the respective time interval still in situ, minus half of the number of cases lost or censored in the respective interval. The proportion of restorations failing and surviving can then be calculated along with a probability density; which is the estimated probability of failure in the respective time intervals.
The resultant figure for the cumulative proportion surviving (also called survival function) is computed by multiplying out the probabilities of survival across all the previous intervals. The median survival time is the time at which the cumulative survival function is equal to 0.5, in other words the time at which the probability of failure is 0.5. If data shows a median survival time of 100+ months, there had been too few failures for the cumulative survival to drop below 0.5 at 100 months. Comparisons of survival between selected variables were made from the life tables using the Wilcoxon (Gehan) statistic; where p <0.05 the variable was assumed to significantly influence survival.
Kaplan and Meier – is a univariate observation analysis method that resembles life table analysis except that the fixed time intervals are replaced with intervals determined by failure events themselves. It calculates the survival probability for each time between placement and the maximum observation time. The data is usually expressed in the form of a stepwise graph that has time on the horizontal axis and cumulative survival on the vertical axis. Mean survival rate was calculated from the area under the plot. The cumulative survival expresses the probability that any restoration in the sample will have a life span exceeding the corresponding time on the plot. Univariate analysis was carried out and log rank statistics compared survival curves for each category of each main variable. Where the log rank score produced p <0.05, the variable was assumed to significantly influence survival.
Cox regression – provided estimates of the effect of the different factors on bridge survival (Table 2). It could adjust results to take into account the influence of significant factors. The data is represented by the hazard ratio (HR) which is the chance of debond in one group of observations divided by the chance of debond in another group. An HR of 1 means the risk is 1 times that of the second group, ie the same. An HR of 2 implies twice the risk. Where p <0.05, the variable was assumed to significantly influence survival.
Results
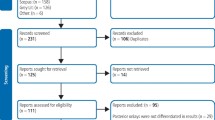
Forty-five patients were identified having a full set of orthodontic study casts and well documented case notes. Fourteen were male and 31 female. The age range of the patients at the time of RBB placement was 13-44 years, with a mode of 16 and a mean of 17.6 years. Seventeen patients had a unilateral missing upper lateral incisor and 28 had bilaterally missing upper lateral incisors. A total of 73 RBBs were under investigation (Fig. 1).

Designs and performance of all 73 RBBs provided
Orthodontic details
Pre-orthodontic incisor and skeletal relationships showed 28 patients to have a class-1 incisor relationship (62.2%), 13 patients (28.9%) had a class-2 incisor relationship (10 patients class-2 division 1, three patients class-2 division 2), and four patients (8.9%) had a class-3 incisor relationship. All the patients were diagnosed with hypodontia, having received orthodontic treatment to open, maintain or redistribute the space of one or both missing maxillary lateral incisors. The age range of the patients at the start of orthodontic treatment was 11-43 years, with a mode of 14 years. Six patients were 18 years or older, giving a mean of 16.6 years. The orthodontic treatment time ranged from seven to 40 months with a mean treatment time of 15.7 months.
Post-orthodontic retention details
Forty-three patients (95.5%) had three or more months of post-orthodontic retention before bridgework was provided. In all but one of these cases an upper removable appliance with prosthetic lateral incisors was the appliance of choice. For the one exception a functional appliance with prosthetic lateral incisors was provided.
Two patients had bridgework fitted immediately after completion of orthodontic treatment and were provided post-orthodontic retention through the use of an upper removable appliance after cementation of the RBBs. One of these patients received six months retention, whilst the other received nine months.
The range of retention time was three to 41 months, with a mean duration of 11.1 months. Eight patients (17.8%) received retention for three to five months, and 37 patients (82.2%) received retention for six months or more.
RRB details
In total, 73 RBBs were provided for the 45 patients during the time period November 1989 to January 2000. Seventeen patients had a unilateral RBB and 28 had bilateral RBBs. Figure 1 shows 62 RBBs were of a cantilever design (38 cantilevered from a canine and 24 from a central incisor), nine were of a fixed/fixed design (from the canine and central incisor), and two were double abutted cantilevers (from the canine and first premolar). During this time period, RBB construction predominantly consisted of the use of a non-perforated nickel-chromium retainer sandblasted with 50-250 μm alumina and luted with a chemically adhesive resin. However, one 'Maryland' retainer was documented along with a traditional 'Rochette' retainer. Fifty-six of the RBBs were cemented with Panavia (Kuraray Co. Ltd. Kita-ku, Osaka, Japan), which during this time period changed from Panavia Ex to Panavia 21. Only six of the bridges (8.2%) were cemented under rubber dam, for which there had been no debonds.
RBB survival
Table 1 shows the life table for all the RBBs provided. The debond failure results for patients attending and not attending for review are also presented in Table 3. In total, 30 RBBs (41.1%) debonded on at least one occasion, of which six (20%) were due to trauma. Forty-three RBBs (58.9%) did not debond.
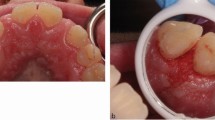
Clinical assessment of the RBBs for the patients who attended for review revealed that there had been only one partial debond for a fixed/fixed design, which had not been accounted for at previous recall. No caries was detected under the debonded retainer. Only one pontic had a porcelain fracture.
Survival curves comparing failure rate of the patients who attended and did not attend for review are shown in Figure 2. As the corroborated data of the patients who attended did not show a higher failure rate than those who did not attend, the data were combined.

Kaplan-Meier survival curve for all RBBs provided for patients who attended and failed to attend for review
Figure 3 shows the survival curve for all 73 RBBs. The age of the bridges from the time of fitting until the last entry in the clinical notes ranged from 0.5 months to 100 months. There was a mean survival time of 59.3 months, and a median time of survival of 59 months. When the RBBs that debonded due to trauma were excluded, the mean survival time increased to 65.6 months. It was not possible to calculate the median survival time as there had not been enough debond failures (ie a value of 100+ months). The remaining analyses were carried out using total number of debonds, where traumatic debond and partial debond counted as debond failure.

Kaplan-Meier survival curve for all patients for all the RBBs provided
Influence of covariates on survival
Grade of operator – was found to have a significant effect on RBB survival (Fig. 4). Senior hospital staff gave the highest results of 72.6 months mean survival time and 100+ months median survival time, with junior members of staff achieving the lowest times (Table 4). Results were statistically significant (using Wilcoxon Gehan and Log rank) when comparing both supervised students and junior hospital staff to senior members of staff (p <0.05), but not when comparing supervised students to junior hospital staff. Table 2 shows that a RBB provided by junior staff was 3.9 times more likely to debond than a RBB provided by senior staff (p = 0.01). Similarly a RBB provided by a supervised student was 2.5 times more likely to debond than a RBB provided by senior staff (p = 0.02).

Kaplan-Meier survival curve for all patients comparing grade of operator providing RBB
Post-orthodontic retention time – the mean and median survival times were 57.5 and 53 months respectively, when retained for six or more months (n = 60), with times of 62.9 and 100+ months when retained for three to five months (n = 13). There was no significant statistical difference seen in survival between the two groups (p = 0.52) and no difference in HR when un-adjusted and adjusted for grade of operator.
RBB design – of the 62 cantilevered RBBs, 25 (40.3%) had debonded; 17 failed when cantilevered from a canine (44.7%) and eight failed when cantilevered from a central incisor (33.3%). Six of the nine fixed/fixed bridges had not debonded (66.7%), however two had a complete debond within 12 months (22.2%) and one had a partial debond after 13 months (11.1%). Both of the double abutted bridges had failed by one month. There was no significant difference in survival between the two types of cantilever design (p = 0.63), or between one retainer (cantilever design) and more than one retainer (fixed/fixed or double abutted design; p = 0.77). The Cox regression data showed no significant differences for bridge design when non-adjusted and adjusted for grade of operator.
Tooth preparation and rubber dam – tooth preparation was documented to have been carried out for 69 cases, however the extent of preparation was unknown. For the four bridges that had no preparation, there had been no debonds. Similarly, rubber dam was only documented for six cases of which none of the bridges had debonded. However, there were insufficient cases in both situations for meaningful analysis.
Pontic contact and survival – of the 39 bridges seen at review, 11 had a contact with the pontic in the intercuspal position and three additional patients had contact with the pontic only in a lateral or protrusive movement. Twenty-five had no contact with the pontic whatsoever. The mean and median survival times were 62.9 and 95 months respectively when there was no contact, with times of 81.9 and 100+ months when there was contact in the intercuspal position or excursive movements. Figure 5 shows a slightly improved survival curve for the RBBs when there were contacts with the pontic, but the difference did not quite reach statistical significance (p = 0.08). The HR when adjusted for grade of operator was 0.31 in favour of contact with the pontic (p = 0.08).

Kaplan-Meier survival curves for all patients attending for review comparing the influence of a pontic contact in static and dynamic movements
Habit history and survival – eight of the 24 reviewed patients reported a positive history of a habit, either clenching or grinding, nail biting or pen chewing. For these patients, 75% of the RBBs were still in situ, and the mean and median survival times were 76.4 and 95+ months. There was no statistical significance between the presence and absence of a habit and survival (p = 0.72), or in the HR when un-adjusted and adjusted for grade of operator.
Discussion
Retrospective studies are often called into question as they rely heavily on the quality of the clinical case notes that have been recorded by multiple operators. It must be emphasised at the outset that this study took special precautions to validate patient records. Firstly, the clinical records of all 59 hypodontia patients were checked to ensure that they were contemporaneous and complete; only 14 were eliminated due to unsatisfactory or incomplete entries. Secondly, in order to ensure that the notes truly represented the clinical condition, a single operator reviewed the patients; only one additional retainer debond and one chipped porcelain pontic were noted. As a final precaution, two separate analyses were carried out for RBB survival in patients who attended for review and those who did not. If the median survival of those who attended had been worse than those who did not, it would have called into question whether all debonds had been fully recorded for non-attendees. In the event a significantly steeper survival plot (p = 0.0007) was formed for the attendees (Fig. 2), giving confidence in the quality of the records and justifying the further analysis of the two groups combined. This improved survival for the attendees may reflect the fact that these patients were more satisfied with the treatment that had been provided and were happier to attend for a review appointment. The poorer survival for the patients who failed to attend may be related to the fact that they were dissatisfied with their treatment and had received alternative treatment elsewhere.
The limitation of both mean and median survival times for studies of this type is that the eventual outcome of the censored restorations is not known; survival time is only confirmed for failed restorations, so a study would have to run indefinitely in order to know precisely all survival times. However, the process of survival analysis takes into account estimated probabilities of failure and number of cases at risk to give the survival function. The advantage of this study is that continued survival, or failure was confirmed for those 39 restorations reviewed at invited follow-up. This information provided a baseline against which the survival of the restorations provided for the 21 patients not attending the invited review could be compared.
This being said, the five-year survival rate in this study was respectable (47% including traumatic debonds and 55% excluding traumatic debonds); however there have been no other previous studies specifically focussing on post-orthodontic hypodontia patients to compare it to. Numerous studies have investigated the general survival of RBBs.24,25,26,27,28,41 It has been reported that bridges provided for younger patients may be subject to higher debond rates, due to shorter clinical crowns with reduced area for bonding, higher incidence of trauma and possibly a higher content of fluoride content in the enamel.24,42 This may partially explain the reduced five-year survival in this study when compared to general survival data of RBBs provided for adult patients with no mention of having had orthodontic treatment, typically 75% for anterior RBBs at 7.5 years.25
The management of a hypodontia patient involves a team approach, and the full integration of the specialties at an early stage is necessary to allow for a treatment plan to be successfully carried out.7,18,19 Assessment of the demographic data in this study reflects general prevalence data, in that more females are affected by hypodontia than males,4,43 and it is more frequent for upper lateral incisors to be missing bilaterally than unilaterally.44 It was evident that the majority of patients started their orthodontic treatment when they were aged 14, with most of the bridges being placed when the patients were aged 15-17. For the majority of these patients the RBB was the definitive restoration and was successful and functioned well for the patient well into early adulthood.
This study is in agreement with previous work by Djemal et al.28 and highlights that if a RBB were to be provided in a hospital environment as part of a complex multidisciplinary treatment plan, a greater longevity may be achieved when provided by a senior member of staff. As discussed, it may not just be the greater level of experience of the treating clinician that results in the increased survival. Other factors applicable to junior members of staff may contribute to their reduced survival; such as unfavourable case allocation, less chair side support, and greater time pressures. Regardless, it does highlight the need for a careful understanding of the potential problems and closer supervision of these cases if being treated by junior members of staff, both in planning and executing of the final stages of the lengthy treatment plan.
If a RBB is not the planned definitive restoration, it can provide satisfactory service until an implant-supported prosthesis could be considered.7 The question of whether the bridge is provisional or definitive can have an impact on whether tooth preparation is carried out or not. In this study, 69 out of the 73 had some form of tooth preparation carried out, with four undocumented cases. If the bridge is considered to be provisional, one may advocate not providing any tooth preparation so as to leave an intact abutment after removal. If the bridge is considered definitive then tooth preparation can be carried out to improve the survival.45,46,47
The importance of effective moisture control and the use of rubber dam has been highlighted.30,31,48,49,50 However, it may sometimes hinder cementation, and, in young patients where minimal undercuts exist due to immature gingival architecture, its placement can be difficult. No further associations can be made from the data, but the likely importance of strict moisture control during bridge placement can be emphasised. The use of rubber dam should be judged on the merits of each case.
Before prosthetic replacement, the orthodontic history should be known, as the tooth movements carried out for hypodontia patients could be prone to relapse, which could inadvertently affect RBB survival. Movements such as space closure in the absence of crowding, de-rotations, space redistribution/creation, and overbite reduction in the absence of a stable occlusal stop, are particularly prone to relapse.17,51
Following orthodontic treatment, some retention is necessary for almost all patients and on occasions this may be life-long.52,53,54 The optimum duration of retention prior to RBB placement, to prevent both tooth positional relapse of the abutment teeth and to secure the longevity of the restoration for these cases, remains undetermined. An accepted protocol is to provide six months full time retention with a removable retainer with prosthetic lateral incisors attached; this is continued during manufacture of the RBB.17 The figure of six months has been derived to allow for periodontal and gingival reorganisation. This is due to the fact that considerable residual force can remain in the tissues of the periodontium after tooth movement, and reorganisation of the periodontal ligament occurs over a three to four month period after treatment.5,56 The gingival collagen fibre network can take four to six months to remodel, and the supra-crestal fibres over 232 days.57
It was previously documented that if orthodontic tooth movement had been carried out before the placement of a RBB, there could be more failures.58 In contrast, if the space had been retained for at least three months, the median survival time can be significantly increased.38 In the present study it was not possible to assess RBB survival times for retention of less than three months, due to insufficient sample size. It was considered appropriate to compare retention of five months or less, with six months or greater, considering current protocols advise at least six months retention.7,17 When comparing three to five months post-orthodontic retention with six or more months, no significant effect on the survival of the RBB was seen in this study.
After active orthodontic therapy and retention, the orthodontist hopes that the fixed restorative work will provide maximum stability of tooth position and prevent unwanted movements. In these situations the restorative dentist needs to know the orthodontic history as this may influence the bridge design.50 It is plausible that a fixed/fixed or multiple retainer design could offer more tooth positional stability when compared to a cantilever design. However, the restorative dentist is concerned about the risk of debond from multiple retained bridges, and catastrophic damage by way of caries if the bridge remains in situ. Also, previous studies have shown that multiple retained bridges may not survive as long as a cantilever design.28 In this study there were no significant differences in survival between the bridge designs, and although one partial debond had occurred in one of the reviewed patients, no caries was detected.
Finally, it has been highlighted that occlusal factors and parafunctional activity may be important in the success and failure of a RBB.31,50,59,60 This study showed no statistically significant adverse effect on survival in the presence of occlusal contact with the pontic, or with the presence of a habit. Indeed, an almost statistically significant improvement was seen for the RBBs that had a contact in the intercuspal position. It may have been that these had been placed by more experienced members of staff with a better understanding of occlusal harmony. Due to the presence of a holding contact in the intercuspal position and harmonious excursive movements, there could be a reduced potential for movement of the abutment tooth position. Paradoxically, as the bridges were reviewed for this study months or years after placement, it is possible that those with interferences may have moved or debonded so that they no longer made occlusal contact.
Further work is necessary to assess tooth positional stability following RBB placement after orthodontic treatment to prepare the missing tooth space, and determine the relative risk of unwanted tooth movement resulting from different orthodontic treatments. It would also be useful to investigate the impact such tooth movements may have on ultimate patient satisfaction levels. Whilst acknowledging the limitations of retrospective studies, the findings are instructive and should inform the development of any future prospective trials of RBBs in hypodontia patients. Bearing in mind the relatively small patient numbers and the time taken to recruit, there is a strong argument for multicentred trials.
Conclusions
Within the limitations of this study, it can be concluded that:
-
1
RBBs replacing missing maxillary lateral incisors are an acceptable restoration that can be provided for young, post-orthodontic hypodontia patients, giving a median survival time of 59 months
-
2
senior members of staff provided the most restorations and achieved the highest survival times
-
3
RBB design had no significant effect on the survival of the restorations
-
4
post-orthodontic retention of six months or more did not significantly improve the survival of the restorations
-
5
the presence of occlusal contact on the pontic, or a habit, had no significant adverse effect on the survival of the restorations in this study.
References
Dhanrajani P J . Hypodontia: etiology, clinical features and management. Quintessence Int 2002; 33: 294–302.
Brook A H . Dental anomalies of number, form and size: their prevalence in British school children. J Int Assoc Dent Child 1974; 5: 37–53.
Lervik T, Cowley G C . Observations of dental disease and anomalies in 9 to 11 year-old Norwegian children. Acta Odontol Scand 1983; 41: 45–51.
Bergstrom K . An orthopantomographic study of hypodontia, supernumeraries and other anomalies in school children between the ages of 8-9 years. Swed Dent J 1977; 1: 145–157.
Hunstadbraten K . Hypodontia in the permanent dentition. J Dent Child 1973; 40: 115–117.
Locht S . Panoramic radiographic examination of 704 Danish children aged 9-10 years. Community Dent Oral Epidemiol 1980; 8: 375–380.
Jepson N J, Nohl F S, Carter N E et al. The interdisciplinary management of hypodontia: restorative dentistry. Br Dent J 2003; 194: 299–304.
Millar B J, Taylor N G . Lateral thinking: the management of missing upper lateral incisors. Br Dent J 1995; 179: 99–106.
Carlson H . Suggested treatment for missing lateral incisor cases. Angle Orthod 1952; 22: 205–216.
Tuverson D L . Orthodontic treatment using canines in place of missing maxillary lateral incisors. Am J Orthod 1970; 58: 109–127.
Robertsson S, Mohlin B . The congenitally missing upper lateral incisor: a retrospective study of orthodontic space closure versus restorative treatment. Eur J Orthod 2000; 22: 697–709.
McNeill R W, Joondeph D R . Congenitally absent maxillary lateral incisors: treatment planning considerations. Angle Orthod 1973; 43: 24–29.
Schroff B, Siegel S M, Feldman S, Siegel S C . Combined orthodontic and prosthetic therapy. Dent Clin N Am 1996; 40: 911–943.
Hobkirk J A, King P A, Goodman J R, Jones S P . Hypodontia: 2. The management of severe hypodontia. Dent Update 1995; 22: 8–11.
Sabri R . Management of missing lateral incisors. J Am Dent Assoc 1999; 130: 80–84.
Shaw W C . Common treatment procedure. In Orthodontics and occlusal management. pp.116–179. Oxford: Butterworth-Heinemann Ltd, 1994.
Carter N E, Gillgrass T J, Hobson R S et al. The interdisciplinary management of hypodontia: Part 3 - orthodontics. Br Dent J 2003; 194: 361–366.
Meechan J G, Carter N E, Gillgrass T J et al. The interdisciplinary management of hypodontia: Part 4 - oral surgery. Br Dent J 2003; 194: 423–427.
Nunn J H, Carter N E, Gillgrass T J et al. The interdisciplinary management of hypodontia: background and role of paediatric dentistry. Br Dent J 2003; 194: 245–251.
Hobson R S, Carter N E, Gillgrass T J et al. The interdisciplinary management of hypodontia: Part 5 - the relationship between an interdisciplinary team and the general dental practitioner. Br Dent J 2003; 194: 479–482.
Jooneph D R, Riedel R A . Orthodontics: current principals and techniques. St. Louis: Mosby-Year Book, 1994.
Rochette A L . Attachment of a splint to enamel of lower anterior teeth. J Prosthet Dent 1973; 30: 418–423.
Howe D F, Denehy G E . Anterior fixed partial dentures utilising the acid-etch technique and a cast metal framework. J Prosthet Dent 1977; 37: 28–31.
Dunne S M, Millar B J . A longitudinal study of the clinical performance of resin bonded bridges and splints. Br Dent J 1993; 174: 405–411.
Creugers N H, Kayser A F, Van't Hof M A . A seven-and-a-half year survival study of resin bonded bridges. J Dent Res 1992; 11: 1822–1825.
Boyer D B, Williams V D, Thayer K E, Denehy G E, Diaz-Arnold A M . Analysis of debond rates of resin bonded prostheses. J Dent Res 1993; 72: 1244–1248.
Wood M, Thompson V P, Morrison G V, Romberg E . Resin bonded bridge recalls: results averaging ten years [IADR abstract 1527]. J Dent Res 1993; 72: 294.
Djemal S, Setchell D, King P, Wickens J . Long-term survival characteristics of 832 resin-retained bridges and splints provided in a post-graduate teaching hospital between 1978 and 1993. J Oral Rehabil 1999; 26: 302–320.
Creugers N H, De Kanter R J A M . Patients' satisfaction in two long-term clinical studies on resin-bonded bridges. J Oral Rehabil 2000; 27: 602–607.
Chang H K, Zidan O, Lee I K, Gomez-Martin O . Resin-bonded fixed partial dentures: a recall study. J Prosthet Dent 1991; 65: 778–781.
Boening K . Clinical performance or resin-bonded fixed partial dentures. J Prosthet Dent 1996; 76: 39–44.
Olin P S, Hill E M E, Donahue J L . Clinical evaluation of resin-bonded bridges: a retrospective study. Quintessence Int 1991; 22: 873–877.
Creugers N H, De Kanter R J A M, Van't Hof M A . Long-term survival data from a clinical trial on resin-bonded bridges. J Dent 1997; 25: 239–242.
De Rijk W G, Wood M, Thompson V P . Maximum likelihood estimates for the lifetime of bonded dental prostheses. J Dent Res 1996; 75: 1700–1705.
Briggs P, Bishop K . The single unit, single retainer, cantilever resin-bonded bridge. Br Dent J 1996; 181: 373–379.
Gilmour A S M, Ali A . Clinical performance of resin-retained fixed partial dentures bonded with a chemically active luting cement. J Prosthet Dent 1995; 73: 569–573.
Hussey D L, Pagni C, Linden G J . Performance of 400 adhesive bridges fitted in a restorative dentistry department. J Dent 1991; 19: 221–225.
Edwards G D, Mitchell L, Welbury R R . An evaluation of resin-bonded bridges in adolescent patients. J Paediatr Dent 1989; 5: 107–114.
Kaplan E L, Meier P . Nonparametric estimation from incomplete observations. J Am Stat Assoc 1958; 53: 457–481.
Cox D R . Regression models and life tables. J Royal Stat Soc 1972; 34: 187–220.
Aslani E, Johansson J, Moberg L-E . Resin-bonded bridges by dental undergraduates: three year follow-up. Swed Dent J 2001; 25: 21–29.
Marinello C P, Kerschbaum T, Heinenberg B . First experiences with resin-bonded bridges and splints - a cross-sectional retrospective study, part II. J Oral Rehabil 1988; 15: 223–235.
Egermark-Eriksson I, Lind V . Congenital numerical variation in the permanent dentition: sex distribution of hypodontia and hyperdontia. Odontol Rev 1971; 22: 309–315.
Stamatiou J, Symons A L . Agenesis of the permanent lateral incisor: distribution, number and sites. J Clin Pediatr Dent 1991; 15: 244–246.
Simon J F, Gartrell R G, Grogono A . Improved retention of acid-etched fixed partial dentures. A longitudinal study. J Prosthet Dent 1992; 68: 611–615.
Rammelsberg P, Pospiech P, Gernet W . Clinical factors affecting adhesive fixed partial dentures: a 6-year study. J Prosthet Dent 1993; 70: 300–307.
Barrack G M, Bretz W A . A long-term prospective study of the etched-cast restoration. Int J Prosthodont 1993; 6: 428–434.
Mohl G, Mehra R, Ford A . Clinical evaluation of etched-metal resin-bonded fixed partial dentures. J Prosthet Dent 1988; 59: 403–404.
Leibenberg W H . Secondary retention of rubber dam: effective moisture control and access considerations. Quintessence Int 1988; 26: 243–252.
Morgan C, Djemal S, Gilmour G . Predictable resin-bonded bridges in general practice. Dent Update 2001; 28: 501–508.
Melrose C, Millett D T . Toward a perspective on orthodontic retention? Am J Orthod Dentofac 1998; 113: 507–514.
Proffit W R . Equilibrium theory revisited: factors influencing position of the teeth. Angle Orthod 1978; 48: 175–186.
Kaplan H . The logic of modern retention procedures. Am J Orthod Dentofac 1988; 93: 325–340.
Houston W J B, Stephens C D, Tulley W J . Stability and retention. In A textbook of orthodontics. 2nd ed. pp 346–356. Oxford: Wright, 1992.
Reitan K . Tissue rearrangement during retention of orthodontically rotated teeth. Angle Orthod 1959; 29: 105–113.
Moss J P . The soft tissue environment of teeth and jaws: an experimental malocclusion: parts 2 and 3. Br J Orthod 1980; 7: 205–216.
Reitan K . Clinical and histologic observations on tooth movement during and after orthodontic treatment. Am J Orthod 1967; 53: 721–745.
Barrack G M . Etched cast restorations. Quintessence Int 1985; 1: 27–34.
Creugers N H, Snoek P A, Van't Hof M A, Kayser A F . A 5-year prospective study. II. The influence of patient-dependent variables. J Oral Rehabil 1989; 16: 521–527.
Berekally T J, Smales R J . A retrospective clinical evaluation of resin-bonded bridges inserted at the Adelaide Dental Hospital. Aust Dent J 1993; 38: 85–96.
Acknowledgements
The authors would like to acknowledge the assistance of Nick Steen for his statistical advice.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Garnett, M., Wassell, R., Jepson, N. et al. Survival of resin-bonded bridgework provided for post-orthodontic hypodontia patients with missing maxillary lateral incisors. Br Dent J 201, 527–534 (2006). https://doi.org/10.1038/sj.bdj.4814160
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4814160
This article is cited by
-
Longevity of resin-bonded fixed partial dental prostheses made with metal alloys
Clinical Oral Investigations (2016)
-
Occlusal rehabilitation in patients with congenitally missing teeth—dental implants, conventional prosthetics, tooth autotransplants, and preservation of deciduous teeth—a systematic review
International Journal of Implant Dentistry (2015)
-
Survival characteristics of 771 resin-retained bridges provided at a UK dental teaching hospital
British Dental Journal (2015)
-
A review of the success and failure characteristics of resin-bonded bridges
British Dental Journal (2013)
-
Resin bonded bridges: techniques for success
British Dental Journal (2011)
