
Key Points
-
Establishes that there is considerable variation between different guideline recommendations, indicating differences in interpretation of the evidence.
-
Encourages more discussion about the frequency and timing of bitewing radiographs with a view to obtaining a consensus of opinion throughout the profession.
-
Provides an objective appraisal of guideline quality.
Abstract
Objectives To identify guidelines on when and how frequently bitewing radiographs should be used in dentistry for the diagnosis of caries, and to provide an objective appraisal of their quality.
Data sources MEDLINE (OVID), US National Guideline Clearinghouse (www.guideline.gov) and the Royal College of Surgeons of England (https://www.rcseng.ac.uk/fds/publications-clinical-guidelines/clinical_guidelines) websites were searched using a variety of relevant search terms (2 August 2016).
Data selection Publications were included if they made recommendations on the issue of when and how frequently radiographs should be used in any dentally-related specialty pertaining to the diagnosis of caries; and/or if they were aimed at the individual practitioner (any health professional working within dentistry) and/or patients.
Data analysis Thirteen published guidelines were included and assessed using the AGREE II instrument.
Conclusions There was a significant variation amongst the guidelines in the recommendations at what age radiography should be undertaken. There was also disagreement on the frequency of repeat radiographs and how this is influenced by the age of the patient and their caries risk.
Similar content being viewed by others


Introduction
The task of diagnosing caries is central to the work of a dentist. Diagnosis depends on a combination of thorough clinical examination and the use of special tests, the most common of which is bitewing radiography. The availability of radiographs can allow the observer to see demineralisation of enamel and dentine by identification of relative radiolucency, although sensitivity (true positive diagnosis) and specificity (true negative diagnosis) are far from perfect, particularly in terms of sensitivity for early lesions.1,2 Furthermore, inter-observer variability in diagnosis is a significant challenge, influenced by image quality, viewing conditions and the observers' experience.3,4,5
Radiography is associated with a radiation dose and this means that its use must be justified on an individual basis rather than used indiscriminately. Justification involves weighing the potential benefit against the radiation risk, but a more practical aid is to consider whether a radiographic examination has a reasonable chance of changing management of the patient. In the UK, the IRMER regulations require justification and that the employer makes selection (or referral) criteria available to assist in choosing X-ray examinations.6 Selection criteria are clinical guidelines, ideally devised using an evidence-based process. The Department of Health recommended in 2001 that dentists might choose to use the FGDP (UK) guideline document 'Selection Criteria for Dental Radiography' as their guideline document.7 This publication made recommendations on frequency of bitewing radiographs for children and adults based on caries risk assessment and was recently revised as a third edition.8 There are, however, guidelines available from other authors and organisations within and outside the UK which differ in their recommendations regarding bitewing radiography. Furthermore, there is evidence that dentists in the UK do not follow the FGDP (UK) guidelines on the use of radiography for caries diagnosis.9,10
The aim of this review was to identify guidelines on when and how frequently bitewing radiographs should be used in dentistry for the diagnosis of caries, to provide an objective appraisal of their quality and to compare the recommendations made in them.
Material and methods
The reporting of this review follows, wherever possible, the format recommended in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.11 A literature search was undertaken to identify published material classifiable as 'guidelines' pertaining to the use of bitewing radiography for dental caries diagnosis.
Eligibility criteria
The identified publications had to meet three criteria for inclusion. A publication must:
-
Have made recommendations on the issue of when and how frequently radiographs should be used in any dentally related specialty pertaining to the diagnosis of caries
-
Be aimed at the individual practitioner (any health professional working within dentistry) and/or patients
-
Be published in, or after, the year 1948.
A publication was excluded when it:
-
Reproduced, without amendment, a current or previous guideline
-
Had been superseded by a more up-to-date version.
No a priori language restrictions were set, as it was anticipated that some non-English publications might be amenable to translation by the authors or by colleagues if needed.
Information sources and search strategy
A MEDLINE (OVID) search was performed prospectively from 1 January 1948, with a final search date of 1 August 2016 (Table 1).
In addition, the US National Guideline Clearinghouse (www.guideline.gov) and the Royal College of Surgeons of England (https://www.rcseng.ac.uk/fds/publications-clinical-guidelines/clinical_guidelines) websites were searched on the same date, and an ad hoc search of Google using a variety of relevant search terms undertaken in anticipation of identifying grey literature (for example, governmental agency reports, specialist society documents).
Where guidelines had been updated or published more than once, the most recent version was used for the assessment, taking into consideration any methods published in previous publications.
Selection of publications
Endnote X4 was used to manage the search results. An initial screening of the results was undertaken by a single assessor (TG) to remove any documents that were clearly not relevant. A second, more focused screening was undertaken by a second assessor (KH) to determine whether the identified documents truly met the inclusion criteria.
Data collection process
Each identified guideline document which met the inclusion criteria was reviewed and the recommendations for timing and frequency of bitewing radiography, along with the related patient clinical characteristics (for example, age, dental development, caries risk), were recorded.
Each guideline was then assessed independently for quality by four appraisers. Assessment of guideline quality was performed using the AGREE II instrument, which assesses the methodological rigour and transparency of guideline development.12 Each appraiser made a judgement on each of the 23 items in six domains allocating a quality score of between 1 and 7. A score of 1 was given when there was no information relevant to the AGREE II item or if the concept was very poorly reported. A score of 7 was given if the quality of reporting was exceptional and where the full criteria and considerations articulated in the AGREE II User's Manual were met. Domain scores were then calculated by summing up all the scores of the individual items in a domain and by scaling the total as a percentage of the maximum possible score for that domain. AGREE II gives no threshold of adequacy for domain scores, but advises that such decisions should be made by the user and guided by the context in which the instrument is being used. In order to establish consistency in the scoring process a pilot exercise was run by the assessors to calibrate the AGREE II instrument and to further specify scoring criteria for certain individual items within the six domains.
Guideline statements relating to when and how frequently bitewing radiographs should be used in any dentally-related specialty pertaining to the diagnosis of caries were extracted. Agreement and disagreement between guidelines was noted.
Results
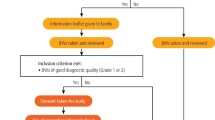
The flow of publications identified by the searches is shown in Figure 1. Full text screening and removal of duplicates left 13 publications remaining for quality assessment.8,13,14,15,16,17,19,20,21,22,23,24

PRISMA flow diagram
Quality assessment
Table 2 shows the results of the quality assessment using the AGREE II instrument. Looking at the six domains considered by the AGREE II tool, some patterns could be seen. Generally positive scores were seen for Domain 1 (scope and purpose). Guideline focus and context were usually very clear, but lower scores were seen for three publications.15,19,21 This was due to the lack of detailed definition of the population sub-groups.
Stakeholder involvement in guideline development scored poorly for all except one guideline.24 This reflected the absence of any patient or public involvement in guideline development, but also the lack of a multidisciplinary team.
Domain 3 (Rigour of development) scored poorly, with extremely low scores recorded for ten of the reviewed publications and with only one achieving a score above 50%.8 The reasons for this included incomplete or completely absent methodological detail, but frequently all of the key items in this domain were missing.
Clarity of presentation (Domain 4) was generally excellent, with only two publications having a prominently lower score.13,21 Nonetheless, even these two scored positively (>50%). The generally high scores were usually due to recommendations being highlighted in Tables rather than being contained within text.
The ratings for Domain 5 (applicability) were generally very poor, demonstrating an almost uniform failure to consider the implications of guideline implementation. Only one publication approached a reasonable quality level (46%) in this domain; this was due to the inclusion of a section on tools for clinical audit in practice.
Editorial independence (Domain 5) almost uniformly scored extremely low with the absence of explicit statements describing the independence and any competing interests of the guideline development group.
Guideline content
A summary of the extracted guidelines is presented in Tables 3,4,5,6,7,8,9,10.
Risk categories
The majority of authors make a distinction between low-risk and high-risk patients. Some introduced a moderate risk category,16,19,20,24 while Jenson et al.20 introduced an 'extreme risk' category.
Whilst not discussed in every guideline, there is a variance in the criteria for distinguishing between risk categories. Some argue that the presence or absence of caries should be used to distinguish between high- and low-risk patients,15,20 whereas others use a multifactorial approach to risk classification. The National Centre for Health Care Technology13 stipulated that risk assessment should encompass a number of criteria, namely: pattern of oral hygiene; exposure to fluoride; amount of retentive carbohydrates in the diet; family dental health; developmental abnormalities; tooth eruption pattern, frequency of dental visits; as well as the clinically observed condition of existing tooth surfaces and restorations. A similar approach requiring a determination of the caries risk was taken by all guidelines.
Age at which first radiograph should be taken
As detailed in Table 11, for some authors, the recommendation is that radiographs should be taken at specific ages – as young as two20 or three years old in some cases,16,21 but not until the child is four,14 five,17,18 or seven years old in others.19,22 Some authors recommend using the child's dental development as an appropriate marker and stipulate that the first radiographs should be taken during the primary dentition stage23 or, if contacts are closed, prior to the eruption of the first permanent tooth.15 Other authors, however, do not suggest a specific age at which the first radiograph should be taken.8,13,24
Age grouping categories
With respect to the categories for children and adolescents, some authors are content to make guideline recommendations that apply to all children,13,15,19 whereas others are much more specific about delineating different age groups and making specific recommendations for each of them.17,18 A number of authors distinguish between children with primary, transitional and permanent dentition, again offering specific recommendations for each category.16,23,24 Some authors also make recommendations against specific age brackets.16,17,18 Although Jenson et al.20 define four different risk categories, they only use one age category – age six and older.
With respect to categories for adults, there is less variation, with the majority making recommendations for just one adult category. Pitts and Kidd16 draw a distinction between four different age categories for adults, making specific recommendations for each. The Swiss Dental Association19 distinguishes between categories of 26–65-year-olds and 65 plus, making slightly different recommendations in each case.
Frequency of radiographs
There is a lot of contention amongst the authors as to what the appropriate interval should be between radiographs, particularly with respect to low-risk children and adolescents. The range extends from somewhere between 12 and 18 months up to 96 months,22 with the majority of authors recommending an interval of somewhere between 12 and 36 months. The divergence of options is compounded, however, by the fact that there is a variance from author to author as to the points in time at which radiographs should be taken as well as the intervals between them. For example, the American Dental Association23 recommends an interval of 12–18 months for low caries risk children in the primary dentition stage and 24 months for both children with mixed dentition and adolescents. Pitts & Kidd16 recommend an interval of 24 months for children aged 3–6 years with deciduous dentition and an interval of 12–24 months for children aged 7–13 years with mixed dentition. Mejàre18 recommends an interval of 36–48 months for 5-year-old children and for children aged 8–9 years. In addition, she recommends an interval of 24 months for 12–13-year-old children and 36 months for 15–16-year-old children. However, in an earlier paper, of which she is a co-author,17 the recommendation is a more specific interval of 36 months for 5-year-old children. The Scottish Dental Clinical Effectiveness Programme recommends24 an interval of 12–18 months for children with primary and mixed dentition and 24 months for children with permanent dentition. Unlike other authors, the National Child Oral Health Service Clinical Guideline21 does not suggest intervals in terms of months, instead they suggest that radiographs should be taken at more specific points – following the eruption of a child's first molars, at 8–9 years old, and again at 11–12 years old. This strategy of linking timing to tooth eruption is also followed by Espelid, Mejare & Weerheijm.17
For those authors who introduce a moderate risk category for children, there is more of a consensus with the majority suggesting an interval of 12 months.16,19,24 Jenson et al.,20 however, recommend an interval of 18–24 months.
For high-risk children, again the divergence of opinion is less, with somewhere between 6–12 months being the most common recommendation.
With respect to intervals for adults, there is more agreement between authors. For adults in the low risk category, the majority advocate that an interval of between 24–36 months is appropriate. For adults aged 56 and over, however, Pitts & Kidd16 recommend an interval of 12–48 months.
For adults with a moderate risk of caries, the recommendations are the same as those for children, with the majority suggesting an interval of 12 months.16,24 The Swiss Dental Association19 advocates an interval of 12-24 months, whereas Jenson et al.20 recommends that the interval should be 18-24 months.
For high risk adults, there is again more variation with some authors suggesting an interval of six months.16,24 Two authors suggest an interval of 6-18 months.20,23 The National Centre for Health Care Technology13 and the Swiss Dental Association19 propose 12 months whereas Stephens and Kogon15 recommend between 12–24 months.
Discussion
The quality of guidelines has been defined as 'the confidence that the potential biases of guideline development have been addressed adequately and that the recommendations are both internally and externally valid, and are feasible for practice'.12
Our aim was to identify when and how frequently bitewing radiographs should be used in dentistry for the diagnosis of dental caries and to assess the quality of guidelines. There is considerable variation between different guideline recommendations, indicating differences in interpretation of evidence. However, most of the guidelines recommend bitewing frequency in the population according to age and the risk of further caries.
The criteria for distinguishing between caries risk categories varies between authors. Validated tools are available to assess caries risk; for example, Caries-Risk Assessment Tool25 the Cariogram26 and the CAMBRA system.27 However, studies of contemporary clinical dental practice have shown that a substantial proportion of dentists do not perform rigorous caries risk assessment or relate the future risk of caries to treatment decisions.28 This may be due to a belief that they are unable to predict caries, economic drivers, and perceived deficiencies in the guidelines themselves or other factors. Past and present caries activity is a simple method of assessing caries risk but has only moderately accurate power of predicting future caries activity.29
Caries risk
Effective monitoring of early carious lesions must involve an assessment of the patient's risk of disease progression and the likelihood of further caries. This is reflected in all the guidelines, where frequency of radiography is based on risk assessment. However, there is disagreement amongst the guidelines about how frequently radiographic assessment should take place. Using the AGREE instrument for all guidelines, we found that there were low percentage scores in the domains of stakeholder involvement, rigour of development, applicability and editorial independence. Organisations that develop practice guidelines should use the AGREE Reporting Checklist, produced by consensus agreement amongst international teams of practice guideline stakeholders, to ensure the full reporting of all relevant information.
Greater consensus between guidelines would be desirable and expected if guidelines are based on adequate evidence, but there are a multiplicity of factors governing the risk of further caries and caries progression. The caries activity of an individual will affect its rate of progression through enamel.30 Many of the earlier classical studies on caries progression were carried out in an era where there was limited access to fluoridated toothpaste and therefore the prophylactic effect of fluoride on enamel remineralisation was not available. Other factors to be considered in the guideline recommendations include the ability of the dentist to detect early caries on bitewing radiography and the consequences of a failure to detect it. Systematic reviews have shown that dentists have a poor sensitivity in detecting even dentine lesions on radiograph; for example, Schwendicke et al.31 found that the sensitivity for detecting dentine proximal caries on radiograph was only 36%.
Impact on treatment choices
A basic element of justification of X-ray imaging is asking the question as to whether the information it provides is likely to alter management. If it is not, then the radiograph is unlikely to be justified. If the initial radiograph shows only very early proximal enamel lesions, and we know that caries progresses through enamel over a period of 4 years,32,33 then it can be argued that radiograph monitoring at intervals of six to twelve months is unnecessary. The lesion will not reach a level at which restorative intervention may be needed in this interval. The treatment required for enamel lesions (oral hygiene instruction, appropriate fluoride administration etc) does not need radiographic information. If the attempts at remineralisation fail and a lesion extends from outer to inner enamel, there would still be no change to management apart from reinforcement of the preventive measures.
Future guideline development
What evidence is needed to determine the appropriate frequency of bitewing radiography for caries diagnosis? On the assumption that larger dentinal lesions would be restored (or the tooth extracted) at the initial treatment phase, subsequent bitewing radiography is used to detect new lesions and to monitor existing lesions that were judged not to require restorative intervention at that time. Thus the fundamental need is to understand the rate at which caries lesions progress through enamel, the amelo-dentinal junction and the outer dentine. Given that caries progresses slowly through enamel and dentine,32,33 it might be concluded that a bitewing should not be repeated until several years have passed. There are, however, several complicating factors that might influence the timing of bitewing radiographs; do we play safe? If caution is preferred, should guidelines take account of poor observer performance, poor radiographic quality and uncertainties around the speed of caries progression and recognise that bitewings should therefore be taken more frequently?
Our aim in this publication is not to construct further guidelines, but to encourage discussion about the more controversial aspects of this field so that general consensus can be obtained throughout the profession. The present guideline recommendations on bitewing radiograph frequency and the age at which the first radiograph should be taken are very varied and, in general, have not involved discussion and general acceptance throughout the profession. Ideally, guidelines should be transparent with regard to the methods used, particularly with regard to assessment and interpretation of the evidence used to support recommendations.
Over recent years GRADE (http://www.gradeworkinggroup.org) has developed as an internationally recognised framework for systematically evaluating the quality of evidence within both systematic reviews and guidelines. It aims to overcome the confusion that arises from having multiple systems for grading evidence and recommendations. By providing a systematic and explicit approach to making and reporting judgments, the use of GRADE in future guidelines may help in reducing the variation in recommendations on bitewing radiograph frequency.
References
Bader J D, Shugars D A, Bonito A J . Systematic reviews of selected dental caries diagnostic and management methods. J Dent Educ 2001; 65: 960–968.
Schwendicke F, Tzschoppe M, Paris S . Radiographic caries detection: A systematic review and meta-analysis. J Dent 2015; 43: 924–933.
Svenson B . The influence of image quality on radiographic diagnosis of approximal caries. Swed Dent J Suppl 1991; 74: 1–62.
Hellén-Halme K, Petersson A, Warfvinge G, Nilsson M . Effect of ambient light and monitor brightness and contrast settings on the detection of approximal caries in digital radiographs: an in vitro study. Dentomaxillofac Radiol 2008; 37: 380–284.
Hellén-Halme K, Petersson G H . Influence of education level and experience on detection of approximal caries in digital dental radiographs. An in vitro study. Swed Dent J 2010; 34: 63–69.
Legislation.gov. The Ionising Radiation (Medical Exposure) Regulations 2000. Available online at http://www.legislation.gov.uk/uksi/2000/1059/contents/made (accessed March 2017).
Department of Health. Guidance Notes for Dental Practitioners on the Safe Use of X-ray Equipment. London: Department of Health, 2001.
Horner K, Eaton K A (Eds). Selection Criteria for Dental Radiography. 3rd Edition. London: Faculty of General Dental Practice (UK), 2013.
Taylor G K, Macpherson L M . An investigation into the use of bitewing radiography in children in Greater Glasgow. Br Dent J 2004; 196: 563–568; discussion 541.
Mauthe P W, Eaton K A . An investigation into the bitewing radiographic prescribing patterns of West Kent general dental practitioners. Prim Dent Care 2011; 18: 107–114.
Moher D, Liberati A, Tetzlaff J, Altman D G, The PRISMA Group: Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg 2010; 8: 336–341.
Brouwers M, Kho M E, Browman G P et al. AGREE II: Advancing guideline development, reporting and evaluation in healthcare. CMAJ 2010; 182: E839–E842.
National Center for Health Care Technology. Dental Radiology: A Summary of Recommendations from the Technology Assessment Forum. J Am Dent Assoc 1981; 103: 423–425.
Stecksén-Blicks C, Wahlin Y B . Diagnosis of approximal caries in pre-school children. Swed Dent J 1982; 7: 179–184.
Stephens R G, Kogon S L . New US guidelines for prescribing dental radiographsa critical review. J Can Dent Assoc 1990; 56: 1019–1024.
Pitts N B, Kidd E A . The prescription and timing of bitewing radiography in the diagnosis and management of dental caries: contemporary recommendations. Br Dent J 1992; 172: 225–227.
Espelid I, Mejare I, Weerheijm K . EAPD guidelines for use of radiographs in children. Eur J Paediatr Dent 2003; 4: 40–48.
Mejàre I . Bitewing examination to detect caries in children and adolescentswhen and how often? Dent Update 2005; 32: 588–590.
Swiss Dental Association. Qualitätsleitlinien in der Zahnmedizin. Schweiz Monatsschr Zahnmed 2005; 115: 1–133.
Jenson L, Budenz A W, Featherstone J D, Ramos-Gomez F J, Spolsky V W, Young D A . Clinical protocols for caries management by risk assessment. J Calif Dent Assoc 2007; 35: 714–723.
National Child Oral Health Services Clinical Guideline. Posterior bitewing (PBW) guideline for child oral health services. 2010. Available online at http://oralhealth.hiirc.org.nz/page/30129/posteriorbitewingpbwguidelinefor-child/?q=bitewing&highlight=bitewing§ion=9005 (accessed May 2015).
Steiner M, Bühlmann S, Menghini G, Imfeld C, Imfeld T . Caries risks and appropriate intervals between bitewing x-ray examinations in schoolchildren. Schweiz Monatsschr Zahnmed 2010; 121: 12–24.
American Dental Association Council on Scientific Affairs. Dental Radiographic Examinations: Recommendations for Patient Selection and Limiting Radiation Exposure. US Department of Health and Human Services, Public Health Service, Food and Drug Administration, 2012.
Scottish Dental Clinical Effectiveness Programme. Oral Health Assessment and Review Dental Clinical Guidance. 2012. Available online at http://www.sdcep.org.uk/wp-content/uploads/2015/04/SDCEP-OHAR-Version-1.0.pdf (accessed May 2015).
American Academy of Pediatric Dentistry Council on Clinical Affairs Policy on use of a caries-risk assessment tool (CAT) for infants, children, and adolescents. Pediatr Dent. 2005–2006; 27 (7 Suppl): 25–27.
Bratthall D, Hänsel Petersson G . Cariograma multifactorial risk assessment model for a multifactorial disease. Community Dent Oral Epidemiol 2005; 33: 256–264.
Doméjean-Orliaguet S, Gansky S A, Featherstone J D . Caries risk assessment in an educational environment. J Dent Educ 2006; 70: 1346–1354.
Riley J L 3rd, Gordan V V, Ajmo C T, Bockman H, Jackson M B, Gilbert GH ; Dental PBRN Collaborative Group. Dentists' use of caries risk assessment and individualized caries prevention for their adult patients: findings from The Dental Practice-Based Research Network. Community Dent Oral Epidemiol 2011; 39: 564–573.
Hänsel Petersson G, Ericson E, Isberg P E, Twetman S . Caries risk assessment in young adults: A 3year validation of clinical guidelines used in Public Dental Service. Acta Odontol Scand 2013; 71: 1645–1650.
Pitts NB . Monitoring of caries progression in permanent and primary posterior approximal enamel by bitewing radiography. Community Dent Oral Epidemiol. 1983; 11: 228–235.
Schwendicke F, Tzschoppe M, Paris S . Radiographic caries detection: A systematic review and meta-analysis. J Dent 2015; 43: 924–933.
Shwartz M, Grondahl H G, Pliskin J S, Boffa J . A longitudinal analysis from bitewing radiographs of the rate of progression of approximal carious lesions through human dental enamel. Arch Oral Biol 1984; 29: 529–536.
Pitts NG . Monitoring of caries progression in permanent and primary posterior approximal enamel by bitewing radiograph: a review. Community Dent Oral Epidemiol 1983; 11: 228–235.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
KH was involved in the development of two publications included in the review, while AMG was involved in one.
Additional information
Refereed Paper
Rights and permissions
About this article

Cite this article
Goodwin, T., Devlin, H., Glenny, A. et al. Guidelines on the timing and frequency of bitewing radiography: a systematic review. Br Dent J 222, 519–526 (2017). https://doi.org/10.1038/sj.bdj.2017.314
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2017.314
This article is cited by
-
Effects of provider incentives on dental X-raying in NHS Scotland: what happens if patients switch providers?
The European Journal of Health Economics (2022)
-
Diagnostic efficacy of and indications for intraoral radiographs in pediatric dentistry: a systematic review
European Archives of Paediatric Dentistry (2020)
-
Best clinical practice guidance for prescribing dental radiographs in children and adolescents: an EAPD policy document
European Archives of Paediatric Dentistry (2020)
-
Combined Near-Infrarred Light Transillumination and Direct Digital Radiography Increases Diagnostic In Approximal Caries
Scientific Reports (2019)
-
Dental caries prevention in children and adolescents: a systematic quality assessment of clinical practice guidelines
Clinical Oral Investigations (2018)
