
Abstract
Study design:
Cross-sectional.
Objectives:
To evaluate exercise equipment preferences and compare cardiometabolic demand for passive hybrid and arm-only exercise among adults with paraplegia (PP) and those with tetraplegia (TP).
Setting:
Four community exercise programmes.
Methods:
Thirty-six adults (mean age: 41.1±12.1 years) with chronic (11.4±10.7 years post injury) TP (C3—C8; n=17) or PP (T3–T12; n=19) were recruited. Participants completed 20 min of submaximal aerobic exercise at moderate to vigorous intensity on four types of aerobic exercise equipment: arm cycle ergometer (ACE), arm glider (AG), arm–leg recumbent stepper (ALRS), and arm–leg cycle ergometer (ALCE). Participants also completed 3 sets of 10 repetitions of resistance exercise using wall pulleys (WP) and weight stack (WS) equipment. A questionnaire was administered to evaluate equipment preference. Heart rate (HR) and oxygen uptake (VO2) were measured in a subset of participants (n=9) during submaximal aerobic exercise.
Results:
Arm-only exercise modes were perceived as being safer than passive hybrid exercise modes. There were no differences in perceived enjoyment between equipment types and groups. There were significant group but not equipment differences in HR (TP: 101.4 bpm; PP: 124.9 bpm) and VO2 (TP: 6.5 ml•kg−1•min−1; PP: 10.5 mL•kg−1•min−1) during submaximal aerobic exercise.
Conclusion:
In this cross-community assessment of exercise equipment preferences after spinal cord injury (SCI), arm-only exercise modes were perceived as safer than hybrid exercise modes and there were no differences between equipment types in physiological responses.
Similar content being viewed by others


Introduction
Despite a growing body of literature supporting the benefits of exercise for persons with spinal cord injury (SCI), there are many aspects of exercise prescription and promotion that remain elusive. The numerous reports of low exercise adherence rates in this population combined with the abundant barriers point to a need for not only effective interventions but also knowledge for directing resource allocation in community exercise programmes.1, 2 Some of the most commonly reported and influential barriers to exercise participation after SCI are intrinsic in nature (lack of motivation, lack of interest, not liking exercise).2, 3 In the able-bodied population, exercise equipment preference has been tied to motivation and adherence; individuals are more likely to adhere to a programme that produces positive affective attitudes.4, 5 Thus, the identification of the preferred mode of exercise among consumers with SCI could be a valuable and strategic contribution to future exercise interventions.
There is limited information available on consumer preference of exercise equipment; one study has shown that people with SCI prefer equipment with the lowest energy cost,6 although this study involved a comparison of only two pieces of equipment. In the able-bodied literature, the results of one investigation suggest that hybrid exercise modes are preferred to leg-only exercise modes;7 however, we are unaware of any comparison of equipment preference using arm-only versus hybrid exercise modes.
Another critical point of comparison between adapted exercise modes is based on physiological outcomes; the most relevant are metabolic demand (oxygen uptake (VO2)) and cardiovascular response (heart rate (HR)). There have been several studies that have attempted to compare exercise modes using these variables; the majority have utilised functional electrical stimulated (FES) exercise and have reported greater oxygen requirements for hybrid FES rowing compared with arm-only rowing8 and for FES hybrid cycling versus arm cycling.9 Further, a study by Hasnan et al.10 revealed that both arm-only exercise and hybrid FES arm–leg exercise elicited a higher VO2 and HR response compared with FES leg exercise alone. Accordingly, electrically stimulating paralysed muscle may provide some metabolic advantage during exercise, although this equipment is relatively expensive and resource intensive compared with basic aerobic and resistance equipment.
The purpose of this study was to evaluate exercise equipment preferences among four types of aerobic and two types of commercially available resistance training equipment based on level of injury. It was predicted that hybrid aerobic exercise would be preferred by the consumer, and there would be no difference in preference between resistance exercise equipment types or level of injury. A secondary objective was to compare exercise equipment in terms of cardiovascular and metabolic demand. It was hypothesised that individuals with tetraplegia (TP) would have a lower VO2 and HR response compared with those with paraplegia (PP) and that hybrid exercise equipment would produce a greater HR and VO2 in response to a submaximal aerobic exercise bout.
Materials and methods
Participants
Participants were recruited from four community exercise programmes for adults with SCI. Inclusion criteria were adults with a chronic SCI (> 1 year post injury) who were 18–65 years old and relied on a wheelchair for mobility. Participants were classified according to level of injury: TP (C1–C8) and PP (T1–T12). Written, informed consent was obtained from each participant, and ethics approval was obtained from the relevant Research Ethics Board at each study site.
Submaximal aerobic exercise
Participants were asked to complete 20 min of submaximal aerobic exercise at moderate to vigorous intensity, corresponding to 3–6 on the 10-point rating of perceived exertion (RPE) scale.11 HR was continually monitored throughout the 30-minute protocol (5 min of baseline, 20 min of exercise, 5 min of recovery) with a chest monitor (Polar Electro Canada, Lachine, QC, Canada), and RPEs were recorded every 5 min.12 Each testing session was completed on separate non-sequential days, and the order of testing was randomised. Four categories of aerobic exercise equipment were compared and are depicted in Figure 1: arm cycle ergometer (ACE; Monark Arm Ergometer Rehab Trainer, Patterson Medical Supply, Mississauga, ON, Canada); arm glider (AG; Vitaglide Pro Glider, RMT Fitness, Miami, FL, USA); hybrid arm and leg recumbent stepper (ALRS; NuStep T5XR Recumbent Cross Trainer, NuStep Inc., Ann Arbor, MI, USA; SCI Fit 7000 Total Body Recumbent Stepper, SCI Fit Ltd., Tulsa, OK, USA) and hybrid arm–leg cycle ergometer (ALCE; SCI Fit Pro 2 Total Body with Adjustable Cranks, SCI Fit Inc., Tulsa, OK, USA). Each study site had a different combination of exercise equipment available; however, all study sites followed a mutually agreed upon protocol.

Aerobic exercise equipment types.
Resistance exercise
Two pieces of resistance exercise equipment were evaluated: wall pulleys (WP; Endorphin Pulleys, Patterson Medical Canada, Mississauga, ON, Canada) and traditional wheelchair-accessible weight stack equipment (WS; Equalizer Multi-Station, Equalizer Exercise Machines, Red Deer, AB, Canada; Cybex VR3 Total Access, Fitness Town Commercial, Vancouver, BC, Canada). Participants were asked to complete 3 sets of 10 repetitions of one exercise using each major muscle group (chest, back, biceps, triceps).11 Wrist cuffs and clips were used when necessary.
Equipment preference questionnaire
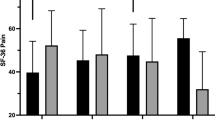
Participants completed a questionnaire to assess their opinions about each piece of exercise equipment immediately following use. Pain was measured using three scales modified from the brief pain inventory and were rated on a 7-point scale (1=none at all, 7=a lot).13, 14 Participants were asked to rate how much shoulder pain, bodily pain and physical discomfort they typically experience and how much they experienced using the specific piece of exercise equipment. The perceived safety of using each piece of equipment was also assessed with two items asking participants to rate how confident they were (1=not at all confident, 7=completely confident) in their ability to use each piece of exercise equipment (a) without assistance and (b) safely without causing injury. The perceived enjoyment of each type of equipment was measured using one scale ‘How much did you like using this specific piece of exercise equipment?’ and answers were rated from 1=not at all to 7=a lot.
Finally, the questionnaire assessed whether participants felt they could use each piece of exercise equipment to meet the physical activity guidelines for adults with SCI. Resistance and aerobic exercise equipment questionnaires included the item ‘Assuming that you are very motivated and fit, how many times per week could you imagine yourself using this specific piece of exercise equipment?’ Participants were asked to select (a) 1, (b) 2, (c) 3, (d) 4, or (e) >4. For aerobic exercise, participants were asked to select how many minutes they could imagine using each piece of equipment: (a) < 5 min, (b) 5 min, (c) 10 min, (d) 15 min, (e) 20 min, (f) 25 min, (g) 30 min, or (h) other. Resistance equipment was evaluated by two items: ‘Assuming you are very motivated, how many sets could you imagine doing while using this specific piece of exercise equipment’, with options of (a) <1, (b) 1, (c) 2, (d) 3, and (e) <3, and ‘Assuming you are very motivated, in one exercise session, how many repetitions could you imagine doing in each set using this specific piece of exercise equipment?’, with options of (a) <5, (b) 5–8, (c) 8–10, (d) 10–12, (e) 12–15, and (f) >15.
Metabolic demand
At one study site, VO2 (VO2000 Metabolic Measurement System, MGC Diagnostics Corp., St. Paul, MN, USA) was measured throughout the exercise protocol on each of three pieces of aerobic exercise equipment (ACE, AG, ALRS) to obtain an assessment of metabolic demand. Steady-state HR and VO2 were defined as the mean value during 20 min of submaximal exercise. Prior to this assessment, participants completed an incremental peak exercise test on an ACE (Lode B.V., Groningen, The Netherlands; Moxus Metabolic System, AEI Technologies Inc., Bastrop, TX, USA).15, 16
Data analysis
Data are presented as mean±s.d. and were analysed using IBM SPSS (IBM SPSS Statistics, Version 20.0). Prior to the analysis, data were evaluated for normality using the Shapiro–Wilk test and equal variances using Levene’s test. Mann–Whitney U-tests were used to compare results between groups (TP vs PP) and Wilcoxon signed-rank tests were used when comparing items from the consumer preference questionnaire based on equipment types (ACE, AG, ALRS, ALCE). Group differences in peak exercise test results were compared using an independent samples t-test. Steady-state HR and VO2 were analysed with a two-way (group × equipment) analysis of variance (ANOVA).
Results
Participants
Thirty-six adults (age: 41.1±12.2 years) with chronic SCI (11.4±10.7 years post injury, C3–T11) were recruited to participate. Nine participants completed the assessment of metabolic demand (age: 40.1±10.8 years, C3–T10, 10.2±11.5 years post injury). Participant characteristics are presented in Table 1.
Equipment preference questionnaire
Results of the consumer preference questionnaire are presented in Table 2. There were no group or equipment differences in perceived enjoyment. Perceived safety was lower when comparing ALRS with ACE (P<0.01), ALCE with ACE (P=0.03) and ALRS with AG (P=0.01). Perceived safety also varied based on level of injury; participants with TP reported lower scores than PP after using ALRS (P=0.04), ACE (P<0.00) and AG (P<0.00).
In the resistance exercise equipment, perceived safety was lower in TP than in PP for both wall pulleys (P<0.01) and weight stack (P=0.02). There were no differences in perceived enjoyment across equipment types or between groups.
Mean scores indicate that participants feel confident in their ability to use the aerobic and resistance exercise equipment to meet or exceed the frequency and time components of the physical activity guidelines for adults with SCI.
Cardiovascular and metabolic responses to submaximal aerobic exercise
Results of the peak exercise test revealed a significant difference in POpeak (P=0.02) and relative VO2peak (P=0.03) between TP and PP groups (Table 3). Physiological responses to submaximal exercise bouts (from the subset of study participants) are presented in Table 4 and Figures 2 and 3. There was a significant main effect for group for steady-state HR (P<0.01), absolute VO2 (P<0.01), relative VO2 (P<0.01) and %HRpeak (P=0.03) across equipment types, where TP had lower values than PP for all variables. There was no significant effect of equipment on steady-state HR or VO2.

Heart rate during 20 min of steady-state submaximal exercise in participants with tetraplegia (TP) and paraplegia (PP).

Oxygen consumption during 20 min of steady-state submaximal exercise in participants with tetraplegia (TP) and paraplegia (PP).
Discussion
The primary objective of this study was to identify aerobic and resistance exercise equipment preferences in the SCI population. A unique aspect of this study was the combination of an equipment preference questionnaire with physiological responses to a submaximal exercise bout. Contrary to our hypothesis, there were no group or equipment differences in overall enjoyment of various types of aerobic or resistance exercise equipment; however, there were significant group and equipment differences in perceived safety. Similarly, there were no differences in HR or VO2 responses to steady-state submaximal exercise between equipment types, but there were differences when comparing individuals with TP and PP.
Although the results of the questionnaire revealed that all pieces of aerobic exercise equipment were equally well liked, it is important to acknowledge that only two-thirds of participants with TP and PP were willing to use ALRS, whereas 100% were willing to use ACE. The reasons cited for not wanting to use the hybrid exercise equipment were the associated transfer or being unable to properly secure feet. Further, among participants willing to use the hybrid exercise equipment, perceived safety was significantly lower among participants with TP across all equipment types and was lower when comparing hybrid exercise with arm-only exercise regardless of injury level. Considering there was no cardiovascular or metabolic advantage to using hybrid exercise, it may be sufficient to promote the use of arm-only exercise, as it appears to be palatable to a broader scope of individuals with SCI.
Preferences for the resistance exercise equipment were similar, as there were no differences between equipment types in perceived enjoyment, and perceived safety was greater among participants with PP. This group difference is likely reflective of the need for assistance in completing many of the resistance exercise manoeuvres (for example attaching wrist cuffs) and changing the equipment settings. It is difficult to distinguish an ideal method for resistance training on these findings alone, although variations in the types of exercises that can be completed and the amount of weight that can be lifted on each machine suggest a specific need for both equipment types in a comprehensive exercise programme.
The lack of differences in energy expenditure between hybrid and arm-only exercise was unexpected. Given that some individuals with incomplete SCI may retain the capacity to voluntarily activate muscles in the lower limbs, we anticipated greater muscle activation with the arm–leg exercise equipment than with arm-only (which would translate into increased VO2). Whereas previous work has shown greater metabolic demand for hybrid versus arms- or legs-only exercise in this population,8, 9, 10, 17 all of these studies have utilised FES. Therefore, it appears that in order for there to be any significant metabolic advantage to hybrid exercise, the equipment must involve electrical stimulation. The use of electromyography to assess muscle activation during non-FES hybrid exercise might be an important addition to future studies to determine whether residual muscle activation in people with incomplete SCI is sufficient to contribute to metabolic demand.
It was encouraging to observe no significant differences in steady-state VO2 or %VO2peak between equipment modes, suggesting that subjects are able to self-select a consistent exercise intensity based on a prescribed RPE. In the present study, participants were instructed to exercise according to verbal anchors of ‘moderate’ and ‘very hard’ on the 10-point RPE scale (RPE of 3–6); yet, the corresponding oxygen uptakes represented only 40–50% of VO2peak. These findings might suggest that participants predominantly rely on peripheral cues of fatigue, previously suggested in the work by Cowan et al.18 Alternatively, people may naturally select the ‘easiest’ intensity when presented with a range to achieve. Thus, to attain an intensity of effort associated with fitness benefits (moderate to vigorous), an RPE of 4–7 may be more appropriate.12 It may also be prudent to provide more specific instruction and divide exertion into both central and peripheral components. The use of peripheral RPE for regulating moderate intensity wheelchair exercise has been shown to be effective in a group of able-bodied participants; however, applicability in the SCI population has yet to be established.19
An obvious limitation to this study was that all of our participants did not complete the exercise bouts using each piece of exercise equipment. We felt this would provide a more accurate reflection of the equipment used in community exercise facilities and we did not feel it was ethically appropriate to require our participants to use pieces of equipment they were not comfortable using.
The findings of this study indicate that there is no difference in perceived enjoyment between commercially available aerobic and resistance exercise equipment; however, individuals with SCI appear to perceive arm-only aerobic exercise modes as being safer than passive hybrid equipment. Promoting the use of arm-only exercise, particularly among persons with TP, may enhance exercise intervention strategies, as additional barriers associated with hybrid exercise equipment may discourage regular use.
Data Archiving
There were no data to deposit.
References
Ginis KAM, Latimer AE, Arbour-Nicitopoulos KP, Buchholz AC, Bray SE, Craven BC et al. Leisure time physical activity in a population-based sample of people with spinal cord injury part I: demographic and injury-related correlates. Arch Phys Med Rehabil 2010; 91: 722–728.
Scelza WM, Kalpakjian CZ, Zemper ED, Tate DG . Perceived barriers to exercise in people with spinal cord injury. Am J Phys Med Rehabil 2005; 84: 576–583.
Cowan RE, Nash MS, Anderson KD . Exercise participation barrier prevalence and association with exercise participation status in individuals with spinal cord injury. Spinal Cord 2013; 51: 27–32.
Rhodes RE, Warburton DER, Bredin SS . Predicting the effect of interactive video bikes on exercise adherence: an efficacy trial. Psychol Health Med 2009; 14: 631–640.
Daley AJ, Maynard IW . Preferred exercise mode and affective responses in physically active adults. Psychol Sport Exerc 2003; 4: 347–356.
Maki KC, Langbein WE, Reid-Lokos C . Energy cost and locomotive economy of handbike and rowcycle propulsion by persons with spinal cord injury. J Rehabil Res Dev 1995; 32: 170–178.
Looney MA, Rimmer JH . Aerobic exercise equipment preferences among older adults: a preliminary investigation. J Appl Meas 2003; 4: 43–58.
Taylor JA, Picard G, Widrick JJ . Aerobic capacity with hybrid FES rowing in spinal cord injury: comparison with arms-only exercise and preliminary findings with regular training. PMR 2011; 3: 817–824.
Brurok B, Torhaug T, Karlsen T, Leivseth G, Helgerud J, Hoff J . Effect of lower extremity functional electrical stimulation pulsed isometric contractions on arm cycling peak oxygen uptake in spinal cord injured individuals. J Rehabil Med 2013; 45: 254–259.
Hasnan N, Ektas N, Tanhoffer AIP, Tanhoffer R, Fornusek C, Middleton J et al. Exercise responses during FES cycling in individuals with spinal cord injury. Med Sci Sports Exerc 2013; 45: 1131–1138.
Ginis KAM, Hicks AL, Latimer AE, Warburton DER, Bourne C, Ditor DS et al. The development of evidence-informed physical activity guidelines for adults with spinal cord injury. Spinal Cord 2011; 49: 1088–1096.
Borg G . Psychophysical bases of perceived exertion. Med Sci Sports Exerc 1982; 14: 377–381.
Cleeland CS, Ryan KM . Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore 1994; 23: 129–138.
Raichle KA, Osborne TL, Jensen MP, Cardenas D . The reliability and validity of pain interference measures in persons with spinal cord injury. J Pain 2006; 7: 179–186.
Hol AT, Eng JJ, Miller WC, Sproule S, Krassioukov AV . Reliability and validity of the six-minute arm test for the evaluation of cardiovascular fitness in people with spinal cord injury. Arch Phys Med Rehabil 2007; 88: 489–495.
Pelletier CA, Jones G, Latimer-Cheung AE, Warburton DE, Hicks AL . Aerobic capacity, orthostatic tolerance, and exercise perceptions at discharge from inpatient spinal cord injury rehabilitation. Arch Phys Med Rehabil 2013; 94: 2013–2019.
Collins EG, Gater D, Kiratli J, Butler J, Hanson K, Langbein WE . Energy cost of physical activities in persons with spinal cord injury. Med Sci Sports Exerc 2010; 42: 691–700.
Cowan RE, Ginnity KL, Kressler J, Nash MS . Assessment of the talk test and rating of perceived exertion for exercise intensity prescription in persons with paraplegia. Top Spinal Cord Inj Rehabil 2012; 18: 212–219.
Paulson TA, Bishop NC, Eston RG, Goosey-Tolfrey VL . Differentiated perceived exertion and self-regulated wheelchair exercise. Arch Phys Med Rehabil 2013; 94: 2269–2276.
Acknowledgements
This work was supported by Rick Hansen Institute (2010-80), Ontario Neurotrauma Foundation (2009-RHI-MTNI-801).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Pelletier, C., Ditor, D., Latimer-Cheung, A. et al. Exercise equipment preferences among adults with spinal cord injury. Spinal Cord 52, 874–879 (2014). https://doi.org/10.1038/sc.2014.146
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2014.146
This article is cited by
-
Acute physiological comparison of sub-maximal exercise on a novel adapted rowing machine and arm crank ergometry in people with a spinal cord injury
Spinal Cord (2022)
-
The ability of heart rate or perceived exertion to predict oxygen uptake varies across exercise modes in persons with tetraplegia
Spinal Cord (2021)
-
Sprint interval training versus moderate-intensity continuous training during inpatient rehabilitation after spinal cord injury: a randomized trial
Spinal Cord (2020)
-
The short-term effect of ultrasound and peripheral nerve stimulator-guided femoral nerve block with phenol on the outcomes of patients with traumatic spinal cord injury
Spinal Cord (2018)
