
Abstract
Prior work suggests that individuals with an eating disorder demonstrate task-based and overall differences in sociocognitive functioning. However, the majority of studies assessed specifically anorexia nervosa and often employed a single experimental paradigm, providing a piecemeal understanding of the applicability of various lab tasks in denoting meaningful differences across diverse individuals. The current study was designed to address these outstanding issues. Participants were undergraduate females who self-identified as having an official (n = 18) eating disorder diagnosis or disordered eating behaviours with no diagnosis (n = 18), along with a control group (n = 32). Participants completed three social tasks of increasing complexity with different outcome measures, namely a gaze cueing task, passive video-watching using eyetracking, and a task to measure preferred social distance. Results diverged as a function of group across tasks; only the control group produced typical social attention effects, the disordered eating group looked significantly more at faces, and the eating disorder group demonstrated a significantly larger preferred social distance. These results suggest variations in task efficacy and demonstrate that altered sociocognitive functioning extends beyond official eating disorder diagnosis.
Similar content being viewed by others


Introduction
Social cognition, or the act of perceiving, attending, remembering, and making judgments about social content, is a crucial process that allows us to navigate seamlessly through our environment1,2. In contrast, individuals with autism spectrum disorder (ASD)3, borderline personality disorder4, social anxiety5, and eating disorders such as anorexia nervosa (AN)6 and bulimia nervosa (BN)7 seem to show difficulties with various aspects of social cognition. For instance, those with an eating disorder have been found to have challenges with theory of mind8, emotional functioning8, and visual processing of body-related stimuli8,9. While there have been lab-based investigations focusing on differences in social cognition between different groups, this approach assumes that the various tasks used to measure social cognition are themselves effective at identifying meaningful differences in social cognition. Furthermore, and exacerbating this assumption, other potential limitations for determining the effectiveness of particular tasks do arise. For example, many investigations employ only one task to provide a measure of social cognition, which does not allow for meaningful cross-task comparisons or a determination of how representative that task is at providing an accurate measure of one’s social cognition. Also, many participant samples consist of highly homogenous subgroups8,9,10,11, which may minimize within-group differences and could lead to overly simplistic conclusions. Thus, our investigation's main aim was to (i) present multiple sociocognitive tasks, increasing in complexity, and (ii) employ a heterogenous, community sample of women who self-report various eating disorder behaviours. This was done to ascertain which tasks, if any, could stratify performance based on the way we grouped participants, namely those who self-reported receiving an official eating disorder diagnosis, those who self-reported eating disorder behaviours but no official diagnosis, or controls.
Social cognition in eating disorders
Previous attempts to outline altered social cognition in individuals with an eating disorder tended to focus on executive function impairments such as theory of mind12,13 and emotional processing14,15. For instance, the data suggest that individuals with AN have difficulty deciphering mental states when looking at eyes or facial expressions of various cartoons16, demonstrating impacted theory of mind. Another area of focus when investigating social cognition is how individuals look at or attend to images of food or bodies17,18. For example, individuals with AN have been found to look at images of food for less time than controls17 and demonstrate early preferential looking towards specific body areas they deem unattractive18. While recent literature has shown that individuals with eating disorders have challenges with social cognition, these conclusions were based on a subset of sociocognitive measures, with a large focus on those diagnosed with AN. Thus our work is focused on assessing other sociocognitive measures across individuals with different eating disorder presentations.
Task rationale
There are many ways to measure social cognition in the lab, from looking at or paying attention to a single item on-screen, all the way up to interacting with other people and their points of view (i.e., theory of mind). With that in mind, we chose tasks and activities that produce performance differences between neurotypical populations and those with reduced sociocognitive functioning. Ultimately, we sought to collect measures commonly employed in the field and assess different facets of social cognition.
First, we used the gaze cueing task because it is a standard laboratory tool in cognitive science, and there is some evidence that one’s level of real-world social competence is linked to performance on this task19,20,21. Second, we used eyetracking technology during a video-watching task to observe social attention during complex social scenarios with multiple stimuli as, currently, gaze behaviour is the most common measurement technique for studying social cognition in real-world settings. Finally, to increase ecological validity, we used the preferred interpersonal space task to measure one’s preferred interpersonal space in a social context.
The cueing task
The cueing task is one of the most widely-used laboratory tasks to measure spatial attention22,23. Several researchers have used variations of this task to measure attention across the lifespan24,25,26, within various clinical populations19,27,28, and in combination with eyetracking29,30, EEG31, and fMRI32,33. The general procedure begins with a cue to direct attention to a spatial location, followed sometime later by a target that appears either in the cued or uncued location. By manipulating the type of spatial cue (i.e., a simple luminance change, symbolic shape, arrow, or face with an averted gaze), one can assess the cues' propensity to shift attention. Further, by manipulating the length of time between the presentation of the cue and the target, one can measure how quickly different cues shift attention, and by manipulating the likelihood that the cue predicts the location of the target (rarely, at chance, most of the time)34,35, one can again make claims about how automatically the various cues shift attention.
Turning to the gaze cueing task, which provides a measure of social attention25,34,36,37, control participants respond faster for gazed-at (cued) as compared to not gazed-at (uncued) targets, even when the face is unlikely to look at the target; this difference in response times is known as the gaze cueing effect. While this task assesses one’s natural propensity to orient attention in the direction of another’s gaze, individual differences have been found to modulate the magnitude of the gaze cueing effect. Specifically, individuals with anxiety19, ASD21,27,38,39, and those with a smaller social network size38 produce smaller gaze cueing effects, suggesting that the gaze cueing task may be a strong index of social functioning in real life.
There has been one investigation to date within the eating disorder population where individuals with AN completed three cueing tasks, with averted gaze, arrow, and a finger pointing left or right acting as cues10. Unlike controls, they found that the individuals with AN did not show early attention shifts for either the gaze or arrow cues; all three cues produced late shifts of attention for both groups. The authors took the lack of an early cueing effect as evidence for impaired bottom-up attention for gaze and arrow cues, but not for body-related cues10, suggesting that individuals with AN may not have a natural propensity to attend to eyes. While this data provides preliminary evidence that individuals with AN may not preferentially attend to eyes, there was no distinction from arrow cues, making it less clear whether it is attention in general, or social attention in particular, that is affected. Further, it is unclear whether absent early orienting for gaze is specific to those with AN or whether this pattern is a hallmark for those with an eating disorder in general. Finally, it remains unclear whether the cueing task parameters are adequate to detect differences in real-life social cognition.
Video watching tasks
One way to increase the complexity of social content is to present various scenes or film clips to participants and ask them to look at, respond to, or judge what is happening40,41. Eyetracking technology is one way to observe naturalistic eye movements when passively viewing social stimuli42. Presenting complex social scenes to participants allows researchers to measure an individual’s propensity to look at certain stimuli over others, which is a limitation of the cueing task43. Moreover, while gaze behaviour may not fully index one’s attentional focus at all times44, eye movements are an important way to take in information and signal information to others. These so-called dual functions of gaze45,46 highlight the rich information one can attain through investigations into participant gaze behaviour while mimicking more ecologically-valid contexts than the cueing task, providing further insight into individual sociocognitive functions.
Research findings indicate that control individuals tend to look primarily at faces and eyes during social viewing tasks47,48,49. Similar to the individual variability found with the gaze cueing task, looking behaviour also varies across individuals, as participants with a higher number of autism-like traits or with social anxiety tend to avoid fixating on faces50,51. Intriguingly, some data suggest an optimal “looking rate” towards faces; those who focus less may miss important social cues, while those who over-fixate on faces may seem threatening during social interactions52. Turning to eyetracking for those with an eating disorder, only a handful of studies have investigated looking patterns for social stimuli. Pertinent to the current study, Pinhas and colleagues9 presented images of people with different body sizes and pictures of social interactions to those with and without AN. While control individuals spent similar amounts of time looking at all three types of images, those with AN looked most at thin body shapes, followed by larger body shapes, and looked least at pictures of social interactions, leading the authors to suggest that social interactions may not be as rewarding for those with AN9. To date, investigations into BN have been limited, focusing more on emotional processing rather than social interactions as a whole14,15,53. The closest study we could find measured the ability of patients with BN to “read the mind in the films”; while overall performance was similar between individuals with BN and controls, those with BN were better able to recognize negative emotions when watching films, potentially suggesting a bias for negative content54. Dovetailing with laboratory findings, real-time social interactions also provide evidence for reduced fixations on the eyes of a conversation partner for those diagnosed with AN9,55. Taken together, there is some research suggesting differences in gaze behaviour towards social content across those with and without AN; it remains unclear whether looking rates diverge within different manifestations of eating disorders.
Preferred interpersonal space task
While laboratory tasks like the cueing task and passive viewing tasks allow for precise experimental control and measurement, it is also essential to consider how social cognition manifests in real-time settings20,56. One ecologically-valid way to measure social cognition in a face-to-face setting while still maintaining a degree of experimental control is by measuring preferred interpersonal space via the stop-distance paradigm4. The stop-distance paradigm is a live, social interaction in which a confederate walks towards a participant. The participant is instructed to say “stop” when they feel uncomfortable, therefore providing a quantifiable measure of one’s personal space. Social distance is the average preferred interpersonal space someone may exhibit around a stranger in the real world. The social distance someone chooses can represent appropriateness, comfort, and intimacy with another person57, impacting sociality.
The stop-distance paradigm has been used to provide a real-world measure of individual differences in sociality in those with borderline personality disorder4, social anxiety5, and ASD58,59. However, to date, this paradigm has not been employed to investigate preferred interpersonal space in those with an eating disorder. Those with borderline personality disorder and social anxiety have been found to have a considerably larger preferred social distance than controls. However, for those with ASD, the findings are mixed; while one study found that people with ASD present with a smaller preferred social distance than controls58, Perry and colleagues5 suggest that the preferred social distance in the ASD group is much more variable, with the level of social anxiety as a good predictor of distance. Despite potential discrepancies with the ASD findings, the stop-distance paradigm appears to be a useful tool to capture individual differences in social cognition in a real-world setting. As environmental context could influence one’s sociality, obtaining an interpersonal, dyadic measurement of social cognition provides another method of determining sociocognitive functioning for those with an eating disorder.
In sum, there is compelling evidence to suggest that individuals with eating disorders may have reduced sociocognitive ability, potentially comparable to individuals with ASD10,27,56,58,59. The dearth of information about how the broader eating disorder community perceives, attends, and interacts with the social world around them is a key reason to investigate this population. Moreover, there is a need to investigate the efficacy of various sociocognitive measures at highlighting potential differences in functioning across the spectrum of eating disorders.
The present study employed three tasks to obtain a multifaceted measure of sociocognitive function. The participant sample consisted of women who self-identified as currently experiencing or having a history of an eating disorder (ED), along with women with no formal diagnosis but who self-report having disordered eating habits (DE) and control individuals. In the lab, participants (i) performed a gaze cueing task to measure social attention to a single face, (ii) watched a short movie clip depicting complex social interactions while their eye movements were tracked, and (iii) completed a face-to-face task to measure preferred social distance in real life. If the tasks are sensitive enough to variations in sociocognitive function, then we would expect differences in performance across all three groups across all three measures. If, however, some tasks are more sensitive than others at detecting variations in social cognition, then only some measures will indicate a meaningful difference between the ED and DE groups.
Method
Participants
A total of 72 undergraduate female students participated in the study, for which 68 were retained; 32 controls (M = 19.2 years, SD = 1.39) and 36 participants who identified as either currently (n = 16) or at some point in the past (n = 20) having an eating disorder (M = 19.7 years, SD = 1.65; see Table 1 for further details). Prior to data collection, participants completed a general pre-screening questionnaire, where they were asked, “Have you ever been diagnosed with an eating disorder?”. Those individuals who answered NO were eligible to participate as a control participant, and those individuals who answered YES and signed up for the study completed a lab-generated questionnaire, where those individuals who reported having an official diagnosis were classified as the eating disorder group (n = 18, M = 19.1, SD = 0.87; henceforth denoted ED; n = 8 currently experiencing ED, n = 10 remitted/recovered ED) and those 18 participants who self-reported experiencing eating disorder symptoms with no formal diagnosis were classified as the disordered eating group (M = 20.3, SD = 2; henceforth denoted DE; n = 8 currently experiencing ED, n = 10 remitted/recovered ED). We did not calculate Body Mass Index (BMI) due to unreliable weight data and the lack of height information. Instead, we relied on a combination of validated ED psychopathology questionnaires and self-reported ED-relevant information. We performed post-hoc independent sample t-tests between the three groups on the eating disorder examination questionnaire short (EDE-QS) scores. The control group scored significantly lower than the ED (t(48) = − 5.6, p < 0.001) and DE groups (t(48) = − 6.8, p < 0.001), while there was no difference between the ED and DE group (t(34) = 2.0, p > 0.05).
Sample size was determined in the following manner. For the gaze cueing task, we referred to a paper that compiled and calculated sample sizes from the literature, where they found that employing a detection task with fixation cue required a sample size of 10 participants60. Turning to the video-watching and stop-distance tasks, less prior work has been conducted, rendering it more difficult to ascertain an adequate sample size. We thus used G*Power 3.161 to estimate the sample size needed to detect differences (if any) between the three groups in the proportion of time spent looking at the eyes or preferred interpersonal distance via repeated-measures ANOVAs with a between-subjects factor. We estimated an effect size f = 0.25, α = 0.05, Power = 0.9, three groups, and two measures, and returned a total sample size of 54 participants.
Participants were all recruited through the University of Alberta’s introductory psychology research participant pool and compensated with course credit. All procedures and protocols were reviewed and approved by the University of Alberta’s Research Ethics Board 2 (REB 2) and adhere to the principles of the Helsinki Declaration. All participants provided written informed consent.
Apparatus
The gaze cueing task and video watching task were run on a Windows PC using a 22.5-in VIEWPixx monitor. Matlab and Psychtoolbox-362 were used to run the gaze cueing task, while Experiment Builder (SR Research; Mississauga, ON) was used to run the video watching task. Eye movements were recorded using the EyeLink 1000 Plus eye tracker (SR Research; Mississauga, ON), with a temporal resolution of 2000 Hz and a spatial resolution of at least 1˚. Nine-point calibration and drift correction were performed at the beginning of the task and repeated during the experiment as necessary (the average spatial error was no greater than 0.42, with maximum error not exceeding 0.80). DataViewer (SR Research, Mississauga, ON) was used to visualize the gaze behaviours and extract the values.
Stimuli
For the gaze cueing task, the stimuli were similar to prior studies34,39,63 that utilized a picture of a female face (6.5 cm W × 8.6 cm H; roughly 4.7 × 6.2 degrees of visual angle) depicting a neutral expression taken from the B series of the Karolinska Directed Emotional Faces database (KDEF)64, model code BF23NES. Eye gaze was adjusted to look left or right with Adobe Photoshop software. The target “X” (approximately 0.6 × 0.7 degrees of visual angle) appeared 6.4 degrees of visual angle (°) to the left or right of the face on-screen. Participants sat approximately 70 to 90 cm from the screen with their head on a chin rest.
For the video watching task, participants watched a six-minute and 15-s video clip of the American version of The Office (NBC), at dimensions of 12.7° (H) × 22° (W), centred on a grey screen. The clip was a shortened version of the Pilot episode of The Office, chosen to include both social and non-social scenes. The included segments from the episode were 0:00–3:00 min, 3:30–4:16 min, 8:39–8:52 min, 8:57–9:17 min 14:00–15:30 min, and 22:13–22:28 min. The clips were cut by exporting the episode from a DVD and using iMovie.
Design and procedure
The tasks were completed as part of a larger ongoing study, whereby participants filled out a battery of self-reports, completed a gaze cueing task, a video watching task with a passive watching and event segmentation component, and a preferred interpersonal space task. The present investigation concentrated on analyzing the gaze cueing task, passive watching, and preferred interpersonal space task. We chose not to include the event segmentation component for the video watching task, whereby individuals made button presses to signify what they perceived to be separate events within the video, as this task addresses a different research question.
Gaze cueing task
Standard procedures were used for the gaze cueing task25,63. Gaze direction (left, right), target location (left, right), and cue-target interval (100, 400, 700 ms) were all equally likely to occur, and participants were informed of this contingency. As per Fig. 1A, each trial began with a fixation cross in the middle of the screen, where participants were asked to focus their attention for the duration of the task. Next, the female face appeared in the center of the screen with eyes looking either left or right. After a cue-target interval of 100, 400, or 700 ms, the target appeared on either the left or right and participants were asked to detect the target via keypress as quickly and as accurately as possible once they perceived the target. The cue and the target remained on the screen until a response was made or until 1,000 ms had passed. No error feedback was provided. The eye tracker was recalibrated between blocks as needed.

(A) depicts the gaze cueing task sequence, with the bottom-left image depicting a cued trial and the bottom-right depicting an uncued trial. (B) shows mean interparticipant correct response times as a function of Cue validity and Cue-target interval by group (Controls, DE, and ED; error bars are standard error of the difference between the means). (C) depicts both the average magnitude of gaze cueing (calculated as the average uncued RT—the average cued RT) for each group (coloured bars) and the individual data points illustrating each participant’s magnitude of gaze cueing.
Participants completed 228 trials split across six blocks of 38 trials, with 36 target-present trials and two target-absent trials per block. The target-absent, or ‘catch’ trials, were to ensure participants were paying attention and not responding sporadically, and accounted for roughly 6% of all trials. Response time was measured from target onset, and participants completed five practice trials at the start of the task.
Video watching task
Participant eye movements were tracked with the eye tracker for the duration of the video. Before the video started, nine-point calibration was completed. Participants passively watched a 6-min and 15-s clip from the American version of The Office (NBC), and were simply instructed to “watch the video”. The Office was chosen to maintain consistency with pre-existing research65 and due to its fast-paced structure and complicated social nature.
Preferred interpersonal space task
Participants began standing face-to-face, 9 feet, 5 inches away from one of three female confederates (who strove to maintain consistency in eye contact, gait, posture, and clothing across all participants). The confederate slowly approached the participant, who was instructed to “say stop when you feel uncomfortable”4. Final toe-to-toe and nose-to-nose distance were measured using a measuring tape, save for the first two individuals we tested, where we obtained just the toe-to-toe distance. Thus those two individuals were removed from the relevant analyses. A total of three trials were run, and mean preferred distances (cm) were calculated.
Eating disorder examination questionnaire short (EDE-QS)
The EDE-QS is a validated twelve-question self-report tool that measures the range and severity of eating disorder features66,67. Participants answer a set of statements regarding their behaviours and attitudes. The first ten questions investigate the frequency of disordered eating within the last seven days. Subscales also measure restraint, eating concern, shape and weight concerns. The possible responses range from zero to three (0 = 0 days, 1 = 1–2 days, 2 = 3–5 days, 3 = 6–7 days). The last two questions ask the respondent to report their attitudes towards their weight over the past seven days. The responses are given in a Likert scale (0 = not at all, 1 = slightly, 2 = moderately, 3 = markedly). The total score is retrieved by summing up the responses. A higher total score represents a higher expression of ED.
Results
Data handling
Gaze cueing task
Errors were defined as trials in which participants responded too quickly (i.e., RTs < 100 ms, known as anticipations: 0.6% of trials), too slowly (i.e., RTs > 1000 ms, known as time outs: 0.7% of trials) or responded during a no-target trial (6% of trials, known as catch trials: 1.2% of trials), and were removed from analyses. Anyone with greater than 10% errors was also removed from the analyses, resulting in a loss of two participants (one control participant and one ED participant). Due to a technical error, data was not obtained for an additional control subject.
Video watching task
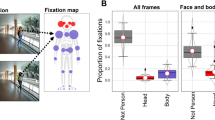
Dynamic interest areas (IAs) were drawn around the actors’ eyes, heads and the background using DataViewer software (SR Research; Mississauga, ON). Gaze behaviour was calculated by determining the proportion of time fixating on the three interest areas (IAs)—the eyes, heads and background—by adding up the total proportion of time fixating on each of the IAs across the entire film clip. Technical issues with the eye tracker resulted in the loss of one control participant.
Preferred interpersonal space task
Nose-to-nose distances were calculated between participants and confederate 3 times to obtain an average nose-to-nose distance. We did not obtain nose-to-nose measures for one ED and one DE participant, and only 31 control participants were included in these analyses due to one outlier.
Data analyses
The data were analyzed in the following order. First, we analyzed whether performance varied across the control, DE, and ED groups for the three experimental tasks. In addition, we computed the scaled Jeffrey-Zellner-Siow (JZS) Bayes factor (BF) to determine whether our main findings were in favour of the null hypothesis using the default Cauchy r scaling value (0.707)68. This approach employs a noninformative prior, employs odds ratios rather than reference cutoffs, and takes into account sample size. Following this, we investigated whether our sociocognitive measures varied systematically with eating disorder symptomology as measured using the EDE-QS questionnaire66, applying Pearson correlation analyses.
Gaze cueing task
We ran three repeated-measures ANOVAs, one for each of the three groups (control, DE, ED), as a function of Cue validity (cued, uncued) and Cue-target interval (100, 400, 700 ms) as within-subject factors (see Fig. 1A for an example task sequence). In line with prior work23,34,63, and as depicted in Fig. 1B,C, the control group showed a typical gaze cueing effect, with faster responses for cued as compared to uncued trials [Cue validity: F(1,31) = 10.4, p < 0.01, ηp2 = 0.25, 95% CI [397.6, 404.8]], that did not vary as a function of timing [Cue validity x Cue-target interval, F < 1, p > 0.4, , ηp2 = 0.03]. In contrast, neither the DE nor the ED group showed significant gaze cueing effects [Cue validity: DE: F(1,17) = 1.1, p > 0.3, ηp2 = 0.06, 95% CI [426.9, 430.0]; ED: F(1,17) = 1.7, p > 0.2, ηp2 = 0.09, 95% CI [414.4, 417.7], nor did this change with target presentation timing [Cue validity x Cue-target interval, both Fs < 1, ps > 0.7, ηp2s < 0.02], indicating no spontaneous attention shifts in response to viewing averted gaze.
We next calculated the magnitude of the gaze cueing effect (average uncued RT– average cued RT) for each participant, and conducted t-tests to determine whether the magnitude was significantly greater than zero for each group. Our control participants demonstrated a robust gaze cueing effect (t(31) = 3.2, p < 0.01, 95% CI [3.1, 13.8], scaled JZS BF = 12.54 favouring the alternative), while the DE and ED groups did not (DE: t(17) = 1.0, p > 0.3, 95% CI [-3.1, 9.2], scaled JZS BF = 2.60 favouring the null; ED: t(17) = 1.3, p > 0.2, 95% CI [-2.1, 8.8], scaled JZS BF = 2.0 favouring the null).
Video watching task
Based on prior work focusing on looking times for the eyes specifically47,69, we ran independent-samples t-tests to compare the proportion of time participants spent looking at the actors' eyes across the control, DE, and ED subgroups (see Table 2 for all data). Perhaps unexpectedly, the proportion of time controls spent looking at the eyes did not differ from either the DE group (t(48) = − 1.6, p = 0.1, Cohen’s d = 0.48, scaled JZS BF = 1.26 favouring the null) or the ED group (t < 1, p > 0.6, Cohen’s d = 0.15, scaled JZS BF = 3.08 favouring the null). The DE group looked significantly more at the eyes as compared to the ED group (t(34) = 2.1, p < 0.05, Cohen’s d = 0.69, scaled JZS BF = 1.60 favouring the alternative). In contrast to the gaze cueing task's findings, the passive video watching task appears sensitive to differences in gaze behaviour across the DE and ED groups.
Preferred interpersonal space task
On average, the preferred social distances were 39.3 cm for the control group, 38.1 cm for the DE group and 58.3 cm for the ED group (see Fig. 2). The numerical difference between the ED group and the other two groups were confirmed with independent samples t-tests, whereby the control group (t(46) = -2.60, p < 0.05, Cohen’s d = 0.72, scaled JZS BF = 4.08 favouring the alternative) and the DE group (t(32) = -2.22, p < 0.05, Cohen’s d = 0.76, scaled JZS BF = 2.05 favouring the alternative) had smaller preferred social distances as compared to the ED group (note, there was no difference between the control and DE group, t(46) < 1, p > 0.8, Cohen’s d = 0.07, scaled JZS BF = 3.29 favouring the null).

Depicts both the average nose-to-nose difference (in cm) as a function of group (coloured bars), along with the individual data points illustrating each participant’s preferred social distance.
Correlation of eating disorder symptomology and social attention
Finally, we investigated whether eating disorder symptomology varied systematically with our social attention measure obtained from the gaze cueing task. To do so, we calculated the magnitude of gaze cueing (see Fig. 1C) by calculating the average RT for cued and uncued trials and subtracting the cued from uncued RTs (i.e., average uncued RT—average cued RT); positive scores indicate the gaze cue has preferentially directed attention, and zero or negative scores indicate attention is not affected by gaze. We found a significant negative correlation between the total EDE-QS66 score and the magnitude of gaze cueing (r = − 0.32, p < 0.01; Fig. 3), with greater eating disorder symptom severity in the past week related to smaller magnitudes of gaze cueing. In other words, those individuals who reported more eating disorder symptoms were less likely to shift their attention in the direction gazed at by an isolated face.

Depicts each participant's average magnitude of gaze cueing (x-axis) as a function of total EDE-QS score (y-axis). Different coloured data points denote group membership.
Discussion
The purpose of this study was to test the efficacy of various sociocognitive tasks at stratifying performance across a community sample of women either with or without a formal eating disorder diagnosis, along with controls. We found that women in both the ED and DE groups did not show a reliable magnitude of gaze cueing for the gaze cueing task, while control participants showed intact gaze cueing. Intriguingly, we found that reduced or reversed magnitudes of gaze cueing were linked to higher acute eating disorder symptomatology, as per the EDE-QS66. In the video watching task, we found a different pattern of results, whereby the DE group fixated significantly more on the actors’ eyes as compared to the ED group. In contrast, for the preferred interpersonal space task where participants were placed in a real-life, face-to-face interaction, the ED group had a significantly larger preferred interpersonal distance than the control and DE groups, who shared a similar preferred distance. Together, our work suggests the different tasks are not equally sensitive at detecting variations in social cognition, which we discuss further below.
Our results for the cueing task suggest that while the task is sensitive enough to detect the presence or absence of social attention for each group, the task was not able to distinguish between the two eating disorder groups. One possibility for this finding could be that the cueing task is simply not sensitive enough to detect differences between the ED and DE groups, while a second possibility could be that there are truly no significant differences between those with an official eating disorder diagnosis versus those who have disordered eating behaviours but do not have a formal diagnosis. These results dovetail with those from Dalmaso and colleagues10, who found that individuals with AN did not produce a gaze cueing effect, yet also extends this conclusion to a broader eating disorder population that spans specific diagnoses. What we mean by this is, aside from the current study, we are unaware of any other research differentiating between women who are officially diagnosed with an eating disorder and those who present with eating disorder symptomology without official diagnosis. More broadly, this finding provides evidence suggesting that spectrum-like features exist for eating disorder symptomatology and diagnoses.
The video watching task provided us with a naturalistic measure of overt attention, parsing fine-grained eye movement differences between the ED and DE groups. Following the cueing task results, we expected that the ED and DE groups would spend less time looking at the eyes during the video. However, we found that the DE group looked at the eyes significantly more than the ED group, with the proportion of time controls looked at the eyes falling between the two groups. While these results may seem surprising, we refer to prior work to contextualize our findings. Specifically, while the data show that some individuals with reduced sociocognitive functioning, such as those with AN and ASD, tend to spend less time looking at the eyes in static images9,50, other work demonstrates that abnormal attentional orienting can also consist of excessive fixations on social stimuli, as seen in Williams syndrome52,70,71. Thus adverse consequences can exist on each side of the spectrum; individuals who tend to focus less on faces may miss important social cues, while individuals who over-fixate on faces may appear to be threatening during social interactions52. Both patterns can lower social adjustment and impact social quality of life72. Of note, there has been very little work to date investigating passive looking rates to video clips in those with reduced social functioning, however with their increased ecological validity and natural social interactions, future work should tease apart potential differences between looking at static social scenes versus dynamic social interactions across individuals with different levels of social functioning.
The preferred interpersonal space task introduced a real-life component to our study to supplement the laboratory-based sociocognitive tasks. Our results show that the ED group preferred a larger distance between themselves and a confederate, as compared to the DE and control groups, who showed no significant differences in interpersonal space. Similar to the video-watching task, the preferred interpersonal space task also appears to function well enough to differentiate between our ED and DE groups, suggesting that this task may be a suitable tool when studying sociocognitive functioning. Prior work has investigated preferred interpersonal space in those with borderline personality disorder and social anxiety, and have found a clearcut difference between controls and these groups, where those diagnosed with borderline personality disorder or social anxiety have shown larger preferred social distances as compared to controls4,5. In contrast, our work, along with prior work investigating preferred social distance in those with ASD, has revealed nuances; preferred social distance in those with ASD seems to be affected more by level of anxiety, and our work suggests that only those with an official eating disorder diagnosis have a larger preferred social distance. We propose that this nuanced pattern of results could be indicative of a spectrum-like composition for individuals with an eating disorder, similar to the spectrum-like nature of ASD. Intriguingly, our results dovetail with recent work investigating inhibition of return (IOR) in those with and without an AN diagnosis73. IOR is a phenomenon whereby participants are slower to respond to targets that appear in the same location as the previous trial, suggesting that we inhibit our attention from returning to the same location over again36. Of note, when completing this task with another person, while control participants demonstrated inhibition effects for both their own previous responses as well as their partner’s (a so-called social IOR effect74) those with AN were found to only produce social IOR, which was larger in magnitude than controls73. When examined alongside our finding of greater preferred interpersonal space for the ED group, there is evidence to suggest that individuals with an eating disorder may be overly attentive to other individuals in real life social interactions, which manifests as providing additional space between themselves and others. Further, as the social IOR paradigm has good ecological validity, the convergence between findings from the stop-signal and sIOR tasks lends additional credibility to the stop-distance paradigm.
Taken together, our investigation demonstrates at least two benefits of using multiple sociocognitive measures with various levels of complexity to parse differences between highly diverse populations. The first insight of our work is that our study demonstrated that the way in which a construct is operationalized may fundamentally change the conclusions one can draw. Specifically, in our case, each task yielded a slightly different picture. For example, if only the gaze cueing task was used, then our data would have both complemented and extended those of Dalmaso and colleagues10; namely, the conclusion would be that social attention is altered not only for those with anorexia nervosa, but also in a community sample of those with and without an official eating disorder diagnosis. While this would be an important extension of prior work, the conclusion would also potentially erroneously suggest that there is no difference in social attention across those with an eating disorder versus those with disordered eating. In contrast, the additional eye tracking and preferred social distance tasks provided a different data pattern, with greater proportions of time looking towards the eyes for those presenting with DE, and larger real life preferred social distances for those in our ED group. When examining sociocognitive functioning through such a holistic lens, we arrive at different conclusions—one that demonstrates a potential spectrum of eating disorder behaviours that might not necessarily be captured by one single task alone. Therefore, there is strong support for conducting research that assesses multiple measures of a construct within the same group of individuals.
The second important insight highlights the validity of using community samples to study social cognition in those with an eating disorder. While prior work has adopted the approach of focusing on homogeneous groups9,10,11, which has clear methodological benefits, we aimed to better understand whether various facets of social cognition do or do not differ between groups as well as within individuals with different eating disorder presentations. Our study found some evidence of reduced sociocognitive functioning in both the ED and DE groups, suggesting that changes in social cognition may be further-reaching than prior research suggests. This could be due to the fact that the prevalence of eating disorder symptoms found within a clinical sample varies from that of larger community sample, with greater instances of purging in bulimia nervosa, and binge/purge-type AN in community samples75,76,77. By virtue of recruiting participants from a clinical sample, only specific symptomatic dimensions may be present, rather than the array of symptoms found across those who exhibit disordered eating behaviours78. Thus it could be that the heterogenous constellation of symptoms in our eating disorder groups explain the pattern of results seen in this study. While there is no prior research that can directly support our interpretations, the broader claim holds, namely that individuals with diverse disordered eating profiles, officially diagnosed or not, appear to have difficulties with aspects of social cognition, highlighting the importance of looking beyond key symptoms addressed within a clinical sample.
No study is without limitations, including the current investigation. For instance, by its very nature, a diverse group will be comprised of smaller sub-diagnostic groups, which may have limited the study’s power. However, a secondary goal was to investigate whether there is variability in social cognition across different instantiations of eating disorder symptomology, thus requiring a diverse sample. A second limitation was the self-report nature of one’s diagnosis (formal or informal). While this is a legitimate concern, in spite of participant self-report we found differences in social cognition as a function of category membership, supporting the notion that the difficulties with sociocognitive function highlighted in those with AN extend to others who exhibit disordered eating behaviours.
In sum, we believe that multiple experimental measures, varying in complexity, are necessary to draw conclusions around particular constructs, especially when the investigation involves heterogeneous community samples. The current study adopted this approach and found that two sociocognitive tasks were efficacious in parsing between ED and DE performance, while the third was able to make a broad-stroked distinction across controls and those with ED or DE. By combining multiple tasks, cross-task evaluations about efficacy and sensitivity of the tasks themselves can be made. Thus, we argue for the importance of drawing from diverse community samples and using various tasks. At the same time, we recognize that this approach may lead to less clear-cut patterns of results. In spite of potential limitations, we believe that multi-task experiments offer unique insights about sociocognitive measuring in the lab, are more representative of real-life behaviours, and underscore the human mind's impressive complexities.
References
Nummenmaa, L. & Calder, A. J. Neural mechanisms of social attention. Trends Cogn. Sci. 13, 135–143. https://doi.org/10.1016/j.tics.2008.12.006 (2009).
Pfeiffer, U. J., Vogeley, K. & Schilbach, L. From gaze cueing to dual eye-tracking: Novel approaches to investigate the neural correlates of gaze in social interaction. Neurosci. Biobehav. Rev. 37, 2516–2528. https://doi.org/10.1016/j.neubiorev.2013.07.017 (2013).
Baron-Cohen, S., Campbell, R., Karmiloff-Smith, A., Grant, J. & Walker, J. Are children with autism blind to the mentalistic significance of the eyes?. Br. J. Dev. Psychol. 13, 379–398. https://doi.org/10.1111/j.2044-835x.1995.tb00687.x (1995).
Fineberg, S. K. et al. Individuals with borderline personality disorder show larger preferred social distance in live dyadic interactions. Psychiat. Res. 260, 384–390. https://doi.org/10.1016/j.psychres.2017.11.054 (2018).
Perry, A., Rubinsten, O., Peled, L. & Shamay-Tsoory, S. G. Don’t stand so close to me: A behavioral and ERP study of preferred interpersonal distance. Neuroimage 83, 761–769. https://doi.org/10.1016/j.neuroimage.2013.07.042 (2013).
Zucker, N. L. et al. Anorexia nervosa and autism spectrum disorders: Guided investigation of social cognitive endophenotypes. Psychol. Bull. 133, 976–1006. https://doi.org/10.1037/0033-2909.133.6.976 (2007).
Dejong, H. et al. Social cognition in bulimia nervosa: A systematic review. Eur. Psychiat. 28, 1–6. https://doi.org/10.1016/j.eurpsy.2011.07.002 (2013).
Adenzato, M., Todisco, P. & Ardito, R. B. Social cognition in anorexia nervosa: Evidence of preserved theory of mind and impaired emotional functioning. PLoS ONE https://doi.org/10.1371/journal.pone.0044414 (2012).
Pinhas, L. et al. Attentional biases to body shape images in adolescents with anorexia nervosa: An exploratory eye-tracking study. Psychiat. Res. 220, 519–526. https://doi.org/10.1016/j.psychres.2014.08.006 (2014).
Dalmaso, M. et al. Altered orienting of attention in anorexia nervosa. Psychiat. Res. 229, 318–325. https://doi.org/10.1016/j.psychres.2015.06.044 (2015).
Ambwani, S. et al. Seeing things differently: An experimental investigation of social cognition and interpersonal behavior in anorexia nervosa. Int. J. Eat. Disord. 49, 499–506. https://doi.org/10.1002/eat.22498 (2016).
Bora, E. & Köse, S. Meta-analysis of theory of mind in anorexia nervosa and bulimia nervosa: A specific İmpairment of cognitive perspective taking in anorexia nervosa?. Int. J. Eat. Disord. 49, 739–740. https://doi.org/10.1002/eat.22572 (2016).
Leppanen, J., Sedgewick, F., Treasure, J. & Tchanturia, K. Differences in the theory of mind profiles of patients with anorexia nervosa and individuals on the autism spectrum: A meta-analytic review. Neurosci. Biobehav. Rev. 90, 146–163. https://doi.org/10.1016/j.neubiorev.2018.04.009 (2018).
Harrison, A., Sullivan, S., Tchanturia, K. & Treasure, J. Emotional functioning in eating disorders: Attentional bias, emotion recognition and emotion regulation. Psychol. Med. 40, 1887–1897. https://doi.org/10.1017/s0033291710000036 (2010).
Bydlowski, S. et al. Emotion-processing deficits in eating disorders. Int. J. Eat Disord. 37, 321–329. https://doi.org/10.1002/eat.20132 (2005).
Russell, T. A., Schmidt, U., Doherty, L., Young, V. & Tchanturia, K. Aspects of social cognition in anorexia nervosa: Affective and cognitive theory of mind. Psychiat. Res. 168, 181–185. https://doi.org/10.1016/j.psychres.2008.10.028 (2009).
Giel, K. E. et al. Attentional processing of food pictures in individuals with snorexia nervosa: An eye-tracking study. Biol. Psychiat. 69, 661–667. https://doi.org/10.1016/j.biopsych.2010.09.047 (2011).
Bauer, A. et al. Visual processing of one’s own body over the course of time: Evidence for the vigilance-avoidance theory in adolescents with anorexia nervosa?. Int. J. Eat. Disord. 50, 1205–1213. https://doi.org/10.1002/eat.22771 (2017).
Süßenbach, F. & Schönbrodt, F. Not afraid to trust you: Trustworthiness moderates gaze cueing but not in highly anxious participants. J. Cogn. Psychol. 26, 670–678. https://doi.org/10.1080/20445911.2014.945457 (2014).
Hayward, D. A., Voorhies, W., Morris, J. L., Capozzi, F. & Ristic, J. Staring reality in the face: A comparison of social attention across laboratory and real world measures suggests little common ground. Can. J. Exp. Psychol. 71, 212–225. https://doi.org/10.1037/cep0000117 (2017).
Bayliss, A. P. & Tipper, S. P. Gaze and arrow cueing of attention reveals individual differences along the autism spectrum as a function of target context. Br. J. Psychol. 96, 95–114. https://doi.org/10.1348/000712604x15626 (2005).
Posner, M. I. Orienting of attention. Quart. J. Exp. Psychol. 32, 3–25. https://doi.org/10.1080/00335558008248231 (1980).
Hayward, D. A. & Ristic, J. Exposing the cuing task: The case of gaze and arrow cues. Atten. Percept. Psychophys. 77, 1088–1104. https://doi.org/10.3758/s13414-015-0877-6 (2015).
Ross-Sheehy, S., Schneegans, S. & Spencer, J. P. The infant orienting with attention task: Assessing the neural basis of spatial attention in infancy. Infancy 20, 467–506. https://doi.org/10.1111/infa.12087 (2015).
Friesen, C. K. & Kingstone, A. The eyes have it! Reflexive orienting is triggered by nonpredictive gaze. Psychon. Bull. Rev. 5, 490–495. https://doi.org/10.3758/Bf03208827 (1998).
Langley, L. K., Friesen, C. K., Saville, A. L. & Ciernia, A. T. Timing of reflexive visuospatial orienting in young, young-old, and old-old adults. Atten. Percept. Psychophys. 73, 1546–1561. https://doi.org/10.3758/s13414-011-0108-8 (2011).
Ristic, J. et al. Eyes are special but not for everyone: The case of autism. Cogn. Brain Res. 24, 715–718. https://doi.org/10.1016/j.cogbrainres.2005.02.007 (2005).
Kingstone, A., Friesen, C. K. & Gazzaniga, M. S. Reflexive joint attention depends on lateralized cortical connections. Psychol. Sci. 11, 159–166. https://doi.org/10.1111/1467-9280.00232 (2000).
Tian, X., Yoshida, M. & Hafed, Z. M. A microsaccadic account of attentional capture and inhibition of return in Posner cueing. Front. Syst. Neurosci. 10, 1–23. https://doi.org/10.3389/fnsys.2016.00023 (2016).
Caldani, S. et al. Impairment in Attention focus during the Posner cognitive task in children with ADHD: An eye tracker study. Front. Pediatr. 8, 1–8. https://doi.org/10.3389/fped.2020.00484 (2020).
Lassalle, A. & Itier, R. J. Fearful, surprised, happy, and angry facial expressions modulate gaze-oriented attention: Behavioral and ERP evidence. Soc. Neurosci. 8, 583–600. https://doi.org/10.1080/17470919.2013.835750 (2013).
Thiel, C. M., Zilles, K. & Fink, G. R. Cerebral correlates of alerting, orienting and reorienting of visuospatial attention: An event-related fMRI study. Neuroimage 21, 318–328. https://doi.org/10.1016/j.neuroimage.2003.08.044 (2004).
Hietanen, J. K., Leppänen, J. M., Nummenmaa, L. & Astikainen, P. Visuospatial attention shifts by gaze and arrow cues: An ERP study. Brain Res. 1215, 123–136. https://doi.org/10.1016/j.brainres.2008.03.091 (2008).
Driver, J. et al. Gaze perception triggers reflexive visuospatial orienting. Vis. Cogn. 6, 509–540. https://doi.org/10.1080/135062899394920 (1999).
Hayward, D. A. & Ristic, J. Measuring attention using the Posner cuing paradigm: The role of across and within trial target probabilities. Front Hum Neurosci 7, 1–11. https://doi.org/10.3389/fnhum.2013.00205 (2013).
Posner, M. I. & Cohen, Y. In Attention and Performance X (eds Bouma, H. & Bouwhuis, D. G.) 531–556 (Erlbaum, 1984).
Langton, S. R. H. & Bruce, V. Reflexive visual orienting in response to the social attention of others. Vis. Cogn. 6, 541–567. https://doi.org/10.1080/135062899394939 (1999).
Hayward, D. A. & Ristic, J. Feature and motion-based gaze cuing is linked with reduced social competence. Sci. Rep. 7, 44221. https://doi.org/10.1038/srep44221 (2017).
Lassalle, A. & Itier, R. J. Autistic traits influence gaze-oriented attention to happy but not fearful faces. Soc. Neurosci. 10, 70–88. https://doi.org/10.1080/17470919.2014.958616 (2015).
Iacoboni, M. et al. Watching social interactions produces dorsomedial prefrontal and medial parietal BOLD fMRI signal increases compared to a resting baseline. Neuroimage 21, 1167–1173. https://doi.org/10.1016/j.neuroimage.2003.11.013 (2004).
Boggia, J. & Ristic, J. Social event segmentation. Quart. J. Exp. Psychol. 68, 731–744. https://doi.org/10.1080/17470218.2014.964738 (2015).
Eckstein, M. K., Guerra-Carrillo, B., Miller Singley, A. T. & Bunge, S. A. Beyond eye gaze: What else can eyetracking reveal about cognition and cognitive development?. Dev. Cognit. Neurosci. 25, 69–91. https://doi.org/10.1016/j.dcn.2016.11.001 (2017).
Pereira, E. J., Birmingham, E. & Ristic, J. The eyes do not have it after all? Attention is not automatically biased towards faces and eyes. Psychol. Res. https://doi.org/10.1007/s00426-018-1130-4 (2019).
Hunt, A. R. & Kingstone, A. Covert and overt voluntary attention: Linked or independent?. Cogn. Brain Res. 18, 102–105. https://doi.org/10.1016/j.cogbrainres.2003.08.006 (2003).
Gobel, M. S., Kim, H. S. & Richardson, D. C. The dual function of social gaze. Cognition 136, 359–364. https://doi.org/10.1016/j.cognition.2014.11.040 (2015).
Risko, E. F., Richardson, D. C. & Kingstone, A. Breaking the fourth wall of cognitive science. Curr. Dir. Psychol. Sci. 25, 70–74. https://doi.org/10.1177/0963721415617806 (2016).
Birmingham, E., Bischof, W. F. & Kingstone, A. Get real! Resolving the debate about equivalent social stimuli. Vis. Cogn. 17, 904–924. https://doi.org/10.1080/13506280902758044 (2009).
Võ, M. L. H., Smith, T. J., Mital, P. K. & Henderson, J. M. Do the eyes really have it? Dynamic allocation of attention when viewing moving faces. J. Vis. 12, 3–3. https://doi.org/10.1167/12.13.3 (2012).
End, A. & Gamer, M. Preferential processing of social features and their interplay with physical saliency in complex naturalistic scenes. Front. Psychol. https://doi.org/10.3389/fpsyg.2017.00418 (2017).
Rigby, S. N., Stoesz, B. M. & Jakobson, L. S. Gaze patterns during scene processing in typical adults and adults with autism spectrum disorders. Res. Autism Spectr. Disord. 25, 24–36. https://doi.org/10.1016/j.rasd.2016.01.012 (2016).
Chen, J., Van Den Bos, E. & Westenberg, P. M. A systematic review of visual avoidance of faces in socially anxious individuals: Influence of severity, type of social situation, and development. J. Anxiety Disord. 70, 102193. https://doi.org/10.1016/j.janxdis.2020.102193 (2020).
Riby, D. M. & Hancock, P. J. Do faces capture the attention of individuals with Williams syndrome or autism? Evidence from tracking eye movements. J. Autism Dev. Disord. 39, 421–431. https://doi.org/10.1007/s10803-008-0641-z (2009).
Renwick, B. et al. Social perception in people with eating disorders. Eur. Psychiat. 28, 436–441. https://doi.org/10.1016/j.eurpsy.2013.03.004 (2013).
Kenyon, M. et al. Theory of mind in bulimia nervosa. Int. J. Eat. Disord. 45, 377–384. https://doi.org/10.1002/eat.20967 (2012).
Harrison, A., Watterson, S. V. & Bennett, S. D. An experimental investigation into the use of eye-contact in social interactions in women in the acute and recovered stages of anorexia nervosa. Int. J. Eat. Disord. https://doi.org/10.1002/eat.22993 (2018).
Dalmaso, M., Castelli, L. & Galfano, G. Social modulators of gaze-mediated orienting of attention: A review. Psychon. B Rev. 27, 833–855. https://doi.org/10.3758/s13423-020-01730-x (2020).
Kaitz, M., Bar-Haim, Y., Lehrer, M. & Grossman, E. Adult attachment style and interpersonal distance. Attach. Hum. Dev. 6, 285–304. https://doi.org/10.1080/14616730412331281520 (2004).
Asada, K. et al. Reduced personal space in individuals with autism spectrum disorder. PLoS ONE 11, e0146306. https://doi.org/10.1371/journal.pone.0146306 (2016).
Perry, A., Levy-Gigi, E., Richter-Levin, G. & Shamay-Tsoory, S. G. Interpersonal distance and social anxiety in autistic spectrum disorders: A behavioral and ERP study. Soc. Neurosci. 10, 354–365. https://doi.org/10.1080/17470919.2015.1010740 (2015).
Chica, A. B., Martín-Arévalo, E., Botta, F. & Lupiáñez, J. The spatial orienting paradigm: How to design and interpret spatial attention experiments. Neurosci. Biobehav. Rev. 40, 35–51. https://doi.org/10.1016/j.neubiorev.2014.01.002 (2014).
Faul, F., Erdfelder, E., Lang, A.-G. & Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39, 175–191. https://doi.org/10.3758/bf03193146 (2007).
Brainard, D. H. The psychophysics toolbox. Spat. Vis. 10, 433–436. https://doi.org/10.1163/156856897x00357 (1997).
Hayward, D. A. & Ristic, J. The uniqueness of social attention revisited: Working memory load interferes with endogenous but not social orienting. Exp. Brain Res. 231, 405–414. https://doi.org/10.1007/s00221-013-3705-z (2013).
Lundqvist, D., Flykt, A. & Öhman, A. (Karolinska Institutet, 1998).
Byrge, L., Dubois, J., Tyszka, J. M., Adolphs, R. & Kennedy, D. P. Idiosyncratic brain activation patterns are associated with poor social comprehension in autism. J. Neurosci. 35, 5837–5850. https://doi.org/10.1523/jneurosci.5182-14.2015 (2015).
Fairburn, C. G. & Beglin, S. J. Assessment of eating disorders: Interview or self-report questionnaire?. Int. J. Eat. Disord. 16, 363–370. https://doi.org/10.1002/1098-108X(199412) (1994).
Gideon, N. et al. Development and psychometric validation of the EDE-QS, a 12 item short form of the eating disorder examination questionnaire (EDE-Q). PLoS ONE 11, e0152744. https://doi.org/10.1371/journal.pone.0152744 (2016).
Rouder, J. N., Speckman, P. L., Sun, D., Morey, R. D. & Iverson, G. Bayesian t-tests for accepting and rejecting the null hypothesis. Psychon. Bull. Rev. 16, 225–237. https://doi.org/10.3758/pbr.16.2.225 (2009).
Birmingham, E., Bischof, W. F. & Kingstone, A. Saliency does not account for fixations to eyes within social scenes. Vision. Res. 49, 2992–3000. https://doi.org/10.1016/j.visres.2009.09.014 (2009).
Riby, D. M. & Hancock, P. J. Viewing it differently: Social scene perception in Williams syndrome and autism. Neuropsychologia 46, 2855–2860. https://doi.org/10.1016/j.neuropsychologia.2008.05.003 (2008).
Riby, D. M., Hancock, P. J., Jones, N. & Hanley, M. Spontaneous and cued gaze-following in autism and Williams syndrome. J. Neurodev. Disord. 5, 13. https://doi.org/10.1186/1866-1955-5-13 (2013).
Kerr-Gaffney, J., Harrison, A. & Tchanturia, K. Cognitive and affective empathy in eating disorders: A systematic review and meta-analysis. Front. Psychiatry https://doi.org/10.3389/fpsyt.2019.00102 (2019).
Dalmaso, M. et al. Altered social attention in anorexia nervosa during real social interaction. Sci. Rep. 6, 23311. https://doi.org/10.1038/srep23311 (2016).
Welsh, T. N. et al. Does Joe influence Fred’s action? Inhibition of return across different nervous systems. Neurosci. Lett. 385, 99–104. https://doi.org/10.1016/j.neulet.2005.05.013 (2005).
Fairburn, C. G., Welch, S. L., Norman, P. A., O’Connor, M. E. & Doll, H. A. Bias and bulimia nervosa: How typical are clinic cases?. Am. J. Psychiatry 153, 386–391. https://doi.org/10.1176/ajp.153.3.386 (1996).
Garfinkel, P. E. et al. Bulimia nervosa in a Canadian community sample: Prevalence and comparison of subgroups. Am. J. Psychiatry 152, 1052–1058. https://doi.org/10.1176/ajp.152.7.1052 (1995).
Garfinkel, P. E. et al. Should amenorrhoea be necessary for the diagnosis of anorexia nervosa? Evidence from a Canadian community sample. Br. J. Psychiatry 168, 500–506. https://doi.org/10.1192/bjp.168.4.500 (1996).
Favaro, A., Ferrara, S. & Santonastaso, P. The spectrum of eating disorders in young women. Psychosom. Med. 65, 701–708. https://doi.org/10.1097/01.psy.0000073871.67679.d8 (2003).
Acknowledgements
This research was partially funded through internal start-up funds (DAH), an NSERC Discovery Grant (DAH), and a summer studentship (DSH) from the Women and Children’s Health Research Institute (WCHRI) at the University of Alberta, Canada, alongside with the Stollery Children’s Hospital Foundation and supporters of the Lois Hole Hospital for Women.
Author information
Authors and Affiliations
Contributions
D.A.H. developed the initial study concept and study design. D.S.H. and N.J. implemented the study and data collection. D.S.H. and D.A.H. conducted the data analyses. All authors wrote the manuscript. All authors approve the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Heath, D.S., Jhinjar, N. & Hayward, D.A. Altered social cognition in a community sample of women with disordered eating behaviours: a multi-method approach. Sci Rep 11, 14683 (2021). https://doi.org/10.1038/s41598-021-94117-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-94117-4
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
