
Abstract
The objective was to study the longitudinal associations between inattention/hyperactivity symptoms and night-waking in preschool-years, in light of their joint evolution. Within the French birth-cohort study EDEN, repeated measures of 1342 children’s night-waking and inattention/hyperactivity symptoms were collected at age 2, 3 and 5–6 through questionnaires. Trajectories were computed using group-based modeling. Logistic regressions, adjusted for confounding factors, were used to measure the association between trajectories and to determine risk factors for belonging to the identified joint trajectories. Two night-waking trajectories were observed, 20% of the children had a trajectory of “common night-waking”, and 80% a trajectory of “rare night-waking”. The children were distributed in three inattention/hyperactivity trajectories, a low (47%), medium (40%) and high one (13%). Both night-waking and inattention/hyperactivity trajectories showed persistence of difficulties in preschool years. The risk of presenting a high inattention/hyperactivity trajectory compared to a low one was of 4.19[2.68–6.53] for common night-wakers, compared to rare night-wakers. Factors associated with joint trajectories were parent’s education level and history of childhood behavioral problems, and the child’s gender, night-sleep duration and collective care at 2 years of age. Results suggest that children presenting behavioral difficulties would benefit from a systematic investigation of their sleep quality and conversely.
Similar content being viewed by others

Introduction
Night-waking is very common amongst preschool-aged children, with 36% signaling their awakening at least once a night1. It is one of the primary complaints of parents to pediatricians2 and has been shown to be persistent within preschool years3. Early inattention/hyperactivity symptoms have also been shown to be persistent over this age range4 and predictive of later poor cognitive development5 and academic underachievement6,7. However, little is known about the associations between night-waking and inattention/hyperactivity in preschool years. In light of the early onset and persistence of night waking and inattention/hyperactivity symptoms, it is essential to study both behaviors in early development.
A systematic literature review8 found 6 studies investigating the association between night-waking and inattention/hyperactivity symptoms in preschool years9,10,11,12,13,14 all with a cross sectional design. Half reported that more night-waking was associated with higher inattention/hyperactivity symptoms10,12,14. In the Hatzinger et al. study11, this association was observed in boys only, while Hall et al.9 and Lehmkulh et al.13 found no significant association. In a previous longitudinal study conducted in the EDEN birth-cohort15 including 1342 children, we showed that children presenting a common night-waking trajectory from age 2 to 5–6 had higher scores of attention/hyperactivity symptoms at age 5–6, compared to children presenting a rare night-waking trajectory. As associations between sleep and behavior may be bidirectional16, we hypothesized that the associations between night-waking and inattention/hyperactivity symptoms could be better understood by studying their joint evolution throughout preschool years.
Thus, the objective of the present study was to investigate the joint trajectories of night-waking and inattention/hyperactivity symptoms from age 2 to 5–6, and their associations with parental and child characteristics, using group-based trajectory modeling.
Methods
Study population
The EDEN birth cohort study recruited pregnant women before their 24th week of amenorrhea between 2003 and 2006 in two French university hospitals, Poitiers and Nancy17. Inclusion criteria were age older than 18 years old, absence of diabetes mellitus, functional literacy in French language and ability to give informed consent. Additional inclusion criteria were social security coverage status and having no plan to change address within the next 3 years. Women with multiple pregnancies were excluded.
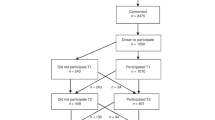
Among the 3758 women invited to participate, 2002 (53%) agreed to enroll in the study. Due to miscarriages, stillbirths and attrition, 1899 children were included at birth. Written informed consent was obtained twice from parents: at enrolment for themselves and after the child’s birth for their child. The study was approved by the Research Ethics Committee of Bicêtre Hospital (Comité Consultatif de Protection des Personnes dans la Recherche Biomédicale) and by the Data Protection Authority (Commission Nationale de l’Informatique et des Libertés). All methods were performed in accordance with relevant guidelines and regulations. Further details on the EDEN study protocol have been published elsewhere17.
Measures
Inattention/hyperactivity symptoms
The child’s inattention/hyperactivity score was obtained at three time points, when the child was 2, 3 and 5–6 years old. At age 2, parents completed a paper-based questionnaire including 6 questions, where they stated whether their child never, sometimes, or frequently displayed the following behaviors over the last 3 months: 1) couldn’t stay in place, was agitated or hyperactive, 2) was distracted, had difficulties completing an activity, 3) was constantly squirming, 4) couldn’t concentrate or maintain his/her attention over a long time span, 5) had difficulties waiting for his turn during a game, 6) was inattentive. A score between 0 and 12 was obtained, with 12 the highest inattention/hyperactivity score. At age 3 and 5–6, parents completed the Strengths and Difficulties Questionnaire (SDQ)18. It is a commonly used questionnaire11,12,14 that has been validated in preschool-aged children19 and in a French non-clinical pediatric population20. Parents had to state whether those 5 statements concerning their child were not true, somewhat true or certainly true over the last 6 months: 1) restless, overactive, cannot stay still for long, 2) constantly fidgeting or squirming, 3) easily distracted, concentration wanders, 4) thinks things out before acting, 5) good attention span, sees work through to the end. A score between 0 and 10 was obtained, with 10 the highest inattention/hyperactivity score. To ensure comparability between inattention/ hyperactivity scores throughout the follow-up period, raw scores were transformed into z-scores, using the within population mean and standard deviation at each age.
Night-waking
In the same paper-based questionnaire, parents reported how many times a week their child woke up during the night at age 2, 3 and 5–6. In accordance with the literature21,22, “frequent night waking” was defined as the child waking every other night or more, as opposed to “no or occasional night waking”.
Covariates
The child’s characteristics included gender, birth order (first/other) and term at birth (weeks of amenorrhea). Parental characteristics were household income at inclusion (less than 1500€, between 1500 and 3000€ or more than 3000€ per month), education (defined as the highest number of years of study reached by one of both parents), history of parental behavior problems in childhood (one or both parents who declared to have had a behavioral problem during childhood), mother’s age at delivery, mother’s depressive symptoms (Center for Epidemiologic Studies-Depression Scale (CES-D) score of 23 or more, threshold validated in French women23), smoking tobacco during pregnancy. The child’s lifestyle and sleep at age 2 included the number of hours spent in front of the television per day, main care arrangement (in large collective settings like preschool or day care centers vs. childminder), the child’s night-sleep duration at age 2, and the child’s sleep habits which were defined as inadvisable if the child had an irregular sleep time or fell asleep with parental presence (yes/no).
Statistical analyses
Children were excluded from the analyses if information on both night-waking and inattention/hyperactivity was missing for more than one time point, resulting in a sample size of 1342 children (71% of the children included at birth). Amongst them, missing data for the covariates represented only 2.0% of the total data, thus simple imputation were performed (i.e. mean value for continuous variables and the modal value for categorical ones). To optimize the analysis of repeated measures in a context of co-evolving outcomes, Nagin’s method for group-based trajectory modeling24 (PROC TRAJ procedure, SAS 9.4 SAS institute INC, Cary, NC, USA®) was used to compute joint trajectories of night-waking and inattention/hyperactivity from age 2 to 5–6. This method allowed us to identify within our population distinctive developmental trajectories for both outcomes. The model provides for each child his/her probability of membership to the different trajectories. It also provides the probability of each combination of night-waking and inattention/hyperactivity trajectories, called joint probabilities and the conditional probabilities, which are the probability of belonging to a night-waking trajectory knowing the inattention/hyperactivity trajectory, and vice-versa. The joint and conditional probabilities are weighted by the individual probability of membership to the different trajectories. We attributed for each child the trajectory of night-waking and the trajectory of inattention/hyperactivity for which he/she had the highest probability of belonging. We used logistic regressions to assess the associations between trajectories, unadjusted and adjusted for the recruitment center (Poitiers or Nancy) and the covariates described above. Using adjusted multinomial logistic regressions, we then investigated the risk factors in association with the joint trajectories.
Results
Population description
Children included in the analyses, compared to those who were not, came from families with higher income (31% versus 19% with a total income >3000€ per months, p < 0.01) and higher education (1.3 years mean difference, p < 0.01). Included mothers also showed less depressive symptoms during pregnancy (7% versus 14%, p < 0.01). The population characteristics are described in Table 1. Mothers were on average 30 years old at delivery and 47% of the children were girls. At the age of 2, children watched on average 43 minutes of television per day. As previously reported3, the optimal trajectory model for describing night-waking patterns was a two-group model (Fig. 1, panel A). The first trajectory, showing low and decreasing prevalence of night-waking over the years was labelled “rare night-waking” represented 80% (N = 1073) of the population. The second trajectory, labelled “common night-waking” trajectory, represented the remaining 20% (N = 269) of the population and was characterized by a peak in night-waking prevalence at age 3. Three trajectories of inattention/hyperactivity were identified (Fig. 1, panel B), labelled low, medium and high inattention/hyperactivity trajectories, representing respectively 47% (N = 630), 40% (N = 538) and 13% (N = 174) of the population. The three trajectories were distinct from the beginning, and remained relatively steady throughout the follow-up, reflecting a perseverance of the inattention/hyperactivity score rank in preschool years. However, the gap between children belonging to the high inattention/hyperactivity trajectory and the others widened over the years.

Trajectories of night-waking and inattention/hyperactivity amongst 1342 children aged 2 to 5–6 years, of the EDEN birth cohort. (A) Frequent night-waking trajectories. White triangles represent the “common night-waking” trajectory (N = 1076, 80%) and the white squares the “rare night-waking” one (N = 269, 20%). (B) Inattention/hyperactivity z-scores trajectories. The black triangles, circles and squares represent respectively the high (N = 174, 13%), medium (N = 538, 40%) and low (N = 630, 47%) inattention/hyperactivity z-score trajectories.
Associations between trajectories
Table 2 describes the interrelationship between night-waking and inattention/hyperactivity trajectories from age 2 to 5–6 years, and provides the conditional and joint probabilities. The probability of having a high inattention/hyperactivity trajectory when belonging to the common night-waking trajectory was of 0.20, versus 0.13 (p = 0.01) when belonging to the rare one. The probability of having a common night-waking trajectory when belonging to the high inattention/hyperactivity trajectory was of 0.31, versus 0.14 (p < 0.01) when belonging to the low one.
Figure 2 provides the distributions of the trajectories after the child attribution to the trajectories for which he/she had the highest probability of belonging. In the panel A are reported the crude distribution of inattention/hyperactivity trajectories by night-waking trajectories and vice-versa for panel B. The distribution of inattention/hyperactivity trajectories significantly differed according to the night-waking trajectories (p < 0.01). Amongst children belonging to the rare night-waking trajectory (panel A), more than half belonged to the low inattention/hyperactivity trajectory and 11% to the high inattention/hyperactivity one. In the common night waking trajectory, only 22% of the children belonged to the low inattention/hyperactivity trajectory and more than 20% to the high inattention/hyperactivity one. In panel B, the prevalence of children belonging to the common night-waking trajectory was similar within both the high and medium inattention/hyperactivity trajectories with respectively 32.2% and 28.6% (p = 0.37). These prevalences were both significantly higher than the one observed in the low inattention/hyperactivity trajectory (p < 0.01).

Prevalences of inattention/hyperactivity and night-waking trajectories. (A) Distribution of inattention/hyperactivity trajectories by night-waking trajectories. (B) Distribution of night-waking trajectories by inattention/hyperactivity trajectories.
Associations between joint trajectories and covariates
The adjusted associations between the joint trajectories of night-waking and inattention/hyperactivity and covariates are reported in Table 3. The distributions of covariates by joint trajectories are in the supplementary data. Joint trajectories showed global associations with parental education and parent’s history of behavior problems in childhood, child gender, collective care arrangement and night-sleep duration. Children who were first born, had shorter night sleep and had parents with a shorter education and more parental history of childhood behavioral problems were more likely to present a joint “common night-waking trajectory and high inattention/hyperactivity”, compared to children in the joint “rare night-waking and low inattention/hyperactivity trajectories” (Reference group). Similarly, risk factors for belonging to the joint “rare night-waking high inattention/hyperactivity, compared to the reference group were to be a boy, have shorter night-sleep, to have for main care arrangement a collective care, to have a mother who smoked tobacco during pregnancy, parents with a shorter education and more parental history of childhood behavioral problems.
Adjusted associations between trajectories
Multivariate logistic regressions indicated that the associations between night-waking and inattention/hyperactivity trajectories described previously remained significant after adjustment for included covariates (Table 4). When comparing children with a medium or a high inattention/hyperactivity trajectory to those with a low one, the risk of belonging to the common night-waking trajectory were respectively of OR = 3.73 CI 95% [2.66–5.23] (p < 0.01) and OR = 4.24 CI 95% [2.72–6.63] (p < 0.01). Children belonging to the high inattention/hyperactivity trajectory compared to the medium one had equivalent risk of belonging to the common night-waking trajectory (p = 0.51).
Discussion
Associations between trajectories
The present study showed that both night-waking and inattention/hyperactivity symptoms were persistent through preschool years. Their trajectories between 2 and 5–6 were highly associated, even after adjusting for multiple confounding factors. These results are in accordance to those reported by Touchette et al. between night sleep duration and hyperactivity16. In their study including 2057 children of the “Quebec longitudinal study of child development”, they found that hyperactivity scores were persistent from age 1.5 to 5, and, except for 5% of the children, night sleep durations were also persistent. Nocturnal sleep durations and hyperactivity trajectories were also significantly associated (X² = 75.1, p < 0.01).
Associations between joint trajectories and covariates
In the adjusted analyses, factors that were globally associated with joint trajectories were parental education, history of childhood behavioral problems, child gender, collective care and night-sleep duration. These results are in accordance with previous literature as male gender25 and shorter parental education26 are common predictors of hyperactivity symptoms. Associations have also been found with lower socio-economic status and night-waking27.
Socio-economic factors
Shorter education often involves unfavorable prenatal conditions and environment for children as well as less access to education and medical care, which could explain the observed increase in behavioral difficulties for this group. The global association between income and joint trajectories was not significant. Yet, children growing in a wealthy family (>3000€/months), compared to those with a household income of less than 1500€/months, were less likely to belong to the joint “high inattention/hyperactivity and common night-waking” trajectory (the least favorable joint trajectory). The lack of global association could be due to a low variance in income in our study sample. The EDEN birth cohort population presents higher income than the general French population17 and further selection due to missing data for night waking or inattention/hyperactivity deepened the miss representativeness of the sample.
The associations with psychoactive substances other than tobacco were not possible in this study, due to very low declared use. It is possible that this low declaration rate is due to the lack of representativeness of our study sample as described above. Other studies are necessary to further understand the specific role of the different psychoactive substances.
Parental history of behavioral problems
History of childhood behavioral problems was associated independently of the socio-economic factors to joint trajectories. According to recent literature, the role of genetic in ADHD is substantial28. The genes that have been associated in the disease are mostly involved in the dopaminergic29 and serotonergic30 systems. Thus the independent association between the parent’s childhood behavioral problems with the child joint trajectories, especially those involving medium or high inattention/hyperactivity trajectories, could be explained by genetics, under the hypothesis that genetics also plays a role in the lower spectrum of attention/hyperactivity difficulties. Another explanation for this association is that there might be unmeasured residual effects of the social environment.
Gender
Our results regarding gender were consistent with the literature, boys have repeatedly been shown to have greater risk of hyperactive symptoms in preschool years25. Touchette et al. similarly found that risk factors of belonging to the least favorable joint trajectory (short-persistent nocturnal sleep duration and high hyperactivity) compared to the most favorable one (11 h persistent nocturnal sleep duration and low hyperactivity) were to be a boy, and to have parents with a low education. But unlike our results, they also found that lower income was a risk factor of presenting the least favorable joint trajectory.
Concordance with sleep duration
As commented above, our findings with night-waking are very similar to those found in night-sleep duration, although our multivariate analyses were adjusted for this factor. Thus, sleep quality is associated with inattention/hyperactivity development independently of sleep quantity. Those results suggest that night-waking should be addressed in parallel to sleep quantity during consultations.
Limitations
The methodology used in our analysis allowed us to describe the joint evolution of night-waking and inattention/hyperactivity and their association, while taking into account confounding factors. Yet there are limitations to be noted in this study. The measurements used for night-waking and inattention/hyperactivity were both subjective. Thus the declared night awakenings were those noticed by parents, indicating the child’s capacity to fall back asleep on his/her own. Also, parents who perceive their child’s sleep as more problematic may also perceive their daytime behaviors as more problematic, thus the associations found are affected by the parent’s belief of normative child behavior. We used a sub-scale of Strengths and Difficulties Questionnaire to assess inattention/hyperactivity. This test has shown good detection power for externalizing behavior when compared to a professionally conducted semi-structured interview31 and has been validated in French children20. A second limit of this study is a relative lack of statistical power in the analysis of adjusted associations between covariates and the joint trajectories. Joint trajectories resulted in a six-group variable, with two including less than 60 children. Adjusting for confounding factors may help reducing bias but at the expense of robustness and statistical power. Thus we were not able to determine whether the lack of associations found with certain factors were due to a low statistical power.
Conclusion
There was a persistence of both night-waking and inattention/hyperactivity in preschool years, and the two behaviors co-evolve. Children who were first born, boys, from less educated families with a history of childhood behavior problems had a higher risk of presenting joint common night-waking and high inattention/hyperactivity trajectories. The results suggest that children presenting behavioral difficulties would benefit from a systematic investigation of their sleep quality and an adapted medical care such as cognitive behavioral therapy, and conversely.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author SP upon reasonable request but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
References
National Sleep Foundation. 2004 Sleep in America Poll. (2004).
Anders, T. F. & Eiben, L. A. Pediatric sleep disorders: a review of the past 10 years. J Am Acad Child Psy 36, 9–20 (1997).
Reynaud, E. et al. Night-waking trajectories and associated factors in French preschoolers from the EDEN birth-cohort. Sleep Med. 27–28, 59–65 (2016).
Salla, J. et al. Childhood trajectories of inattention-hyperactivity and academic achievement at 12 years. Eur. Child Adolesc. Psychiatry 25, 1195–1206 (2016).
Turney, K. & McLanahan, S. The academic consequences of early childhood problem behaviors. Soc. Sci. Res. 54, 131–145 (2015).
Hinshaw, S. P. On the distinction between attentional deficits/hyperactivity and conduct problems/aggression in child psychopathology. Psychol. Bull. 101, 443–463 (1987).
Pingault, J.-B. et al. The developmental course of childhood inattention symptoms uniquely predicts educational attainment: a 16-year longitudinal study. Psychiatry Res. 219, 707–709 (2014).
Reynaud, E., Vecchierini, M.-F., Heude, B., Charles, M.-A. & Plancoulaine, S. Sleep and its relation to cognition and behaviour in preschool-aged children of the general population: a systematic review. J. Sleep Res. 27, e12636 (2018).
Hall, W. A., Scher, A., Zaidman-Zait, A., Espezel, H. & Warnock, F. A community-based study of sleep and behaviour problems in 12- to 36-month-old children. Child Care Health Dev. 38, 379–389 (2012).
Zaidman-Zait, A. & Hall, W. A. Children’s night waking among toddlers: relationships with mothers’ and fathers’ parenting approaches and children’s behavioural difficulties. J. Adv. Nurs. 71, 1639–1649 (2015).
Hatzinger, M. et al. Sleep actigraphy pattern and behavioral/emotional difficulties in kindergarten children: association with hypothalamic-pituitary-adrenocortical (HPA) activity. J. Psychiatr. Res. 44, 253–261 (2010).
Hiscock, H., Canterford, L., Ukoumunne, O. C. & Wake, M. Adverse associations of sleep problems in Australian preschoolers: national population study. Pediatrics 119, 86–93 (2007).
Lehmkuhl, G., Fricke-Oerkermann, L., Wiater, A. & Mitschke, A. Sleep disorders in children beginning school: their causes and effects. Dtsch. Ärztebl. Int. 105, 809–814 (2008).
Wada, K. et al. Associations of endogenous melatonin and sleep-related factors with behavioral problems in preschool Japanese children. Ann. Epidemiol. 23, 469–474 (2013).
Reynaud, E. et al. Night-waking and behavior in preschoolers: a developmental trajectory approach. Sleep Med. 43, 90–95 (2018).
Touchette, E. et al. Short nighttime sleep-duration and hyperactivity trajectories in early childhood. Pediatrics 124, e985–993 (2009).
Heude, B. et al. Cohort Profile: The EDEN mother-child cohort on the prenatal and early postnatal determinants of child health and development. Int. J. Epidemiol, https://doi.org/10.1093/ije/dyv151 (2015).
Goodman, R. The Strengths and Difficulties Questionnaire: a research note. J. Child Psychol. Psychiatry 38, 581–586 (1997).
Croft, S., Stride, C., Maughan, B. & Rowe, R. Validity of the strengths and difficulties questionnaire in preschool-aged children. Pediatrics 135, e1210–1219 (2015).
Shojaei, T., Wazana, A., Pitrou, I. & Kovess, V. The strengths and difficulties questionnaire: validation study in French school-aged children and cross-cultural comparisons. Soc. Psychiatry Psychiatr. Epidemiol. 44, 740–7 (2009).
Zuckerman, B., Stevenson, J. & Bailey, V. Sleep Problems in Early Childhood: Continuities, Predictive Factors, and Behavioral Correlates. Pediatrics 80, 664–71 (1987).
Shang, C.-Y., Gau, S. S.-F. & Soong, W.-T. Association between childhood sleep problems and perinatal factors, parental mental distress and behavioral problems. J. Sleep Res. 15, 63–73 (2006).
Fuhrer, R. & Rouillon, F. La version française de l’échelle CES-D (Center for Epidemiologic Studies-Depression Scale). Description et traduction de l’échelle d’auto-évaluation. Psychiatrie et Psychobiologie 163–166 (1989).
Nagin, D. Group-based modeling of development. (Harvard University Press, 2005).
Romano, E., Tremblay, R. E., Farhat, A. & Côté, S. Development and prediction of hyperactive symptoms from 2 to 7 years in a population-based sample. Pediatrics 117, 2101–2110 (2006).
Smith, E. et al. Preschool hyperactivity specifically elevates long-term mental health risks more strongly in males than females: a prospective longitudinal study through to young adulthood. Eur. Child Adolesc. Psychiatry 26, 123–136 (2017).
Bagley, E. J., Kelly, R. J., Buckhalt, J. A. & El-Sheikh, M. What keeps low-SES children from sleeping well: the role of presleep worries and sleep environment. Sleep Med. 16, 496–502 (2015).
Ptacek, R., Kuzelova, H. & Stefano, G. B. Genetics in Psychiatry - up-to-date review 2011. Neuro Endocrinol. Lett. 32, 389–399 (2011).
Bellgrove, M. A. et al. Association between dopamine transporter (DAT1) genotype, left-sided inattention, and an enhanced response to methylphenidate in attention-deficit hyperactivity disorder. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 30, 2290–2297 (2005).
Oades, R. D. et al. The influence of serotonin- and other genes on impulsive behavioral aggression and cognitive impulsivity in children with attention-deficit/hyperactivity disorder (ADHD): Findings from a family-based association test (FBAT) analysis. Behav. Brain Funct. BBF 4, 48 (2008).
Goodman, R. & Scott, S. Comparing the Strengths and Difficulties Questionnaire and the Child Behavior Checklist: Is Small Beautiful? J. Abnorm. Child Psychol. 27, 17–24.
Acknowledgements
Collaborators: We thank the EDEN mother-child cohort study group (I. Annesi-Maesano, J.Y. Bernard, J. Botton, M.A. Charles, P. Dargent-Molina, B. de Lauzon-Guillain, P. Ducimetière, M. de Agostini, B. Foliguet, A. Forhan, X. Fritel, A. Germa, V. Goua, R. Hankard, B. Heude, M. Kaminski, B. Larroque, N. Lelong, J. Lepeule, G. Magnin, L. Marchand, C. Nabet, F. Pierre, R. Slama, M.J. Saurel-Cubizolles, M. Schweitzer, O. Thiebaugeorges). We thank all funding sources for the EDEN study: Foundation for Medical Research (FRM, n° ARS-3.29), National Agency for Research (ANR, n° 03-BLAN-0359-01, n° 06-SEST-03501, n° 06-SEST-03502), National Institute For Research In Public Health (IRESP: TGIR cohorte santé 2008 program), French Ministry of Health (DGS, n° CV05000146), French Ministry of Research, INSERM Bone and Joint Diseases National Research (PRO-A) and Human Nutrition National Research Programs (n° 4NU06G), Paris-Sud University, Nestlé, French National Institute for Population Health Surveillance (InVS, n° 05-PCTT2043), French National Institute for Health Education (INPES, n° 007/05 DAS), the European Union FP7 programs, Diabetes National Research Program, Mutuelle Générale de l’Education Nationale complementary health insurance (MGEN), French national agency for food security, French speaking association for the study of diabetes and metabolism (ALFEDIAM).
Author information
Authors and Affiliations
Contributions
Eve Reynaud carried out the analyses, interpreted the data, and drafted the initial manuscript. Anne Forhan participated in the data collection, managed the EDEN database and gave guidance for the statistical analyses. Barbara Heude PhD, Marie-Aline Charles MD MPH designed and coordinated the data collection and reviewed the manuscript. Sabine Plancoulaine MD PhD supervised the conception, design and interpretation of the analyses and critically reviewed the manuscript. All authors and approved the final manuscript as submitted.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Reynaud, E., Forhan, A., Heude, B. et al. Association of night-waking and inattention/hyperactivity symptoms trajectories in preschool-aged children. Sci Rep 8, 15412 (2018). https://doi.org/10.1038/s41598-018-33811-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-33811-2
Keywords
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
