
Abstract
Exercise modulates both brown adipose tissue (BAT) metabolism and white adipose tissue (WAT) browning in murine models. Whether this is true in humans, however, has remained unknown. An unblinded randomized controlled trial (ClinicalTrials.gov ID: NCT02365129) was therefore conducted to study the effects of a 24-week supervised exercise intervention, combining endurance and resistance training, on BAT volume and activity (primary outcome). The study was carried out in the Sport and Health University Research Institute and the Virgen de las Nieves University Hospital of the University of Granada (Spain). One hundred and forty-five young sedentary adults were assigned to either (i) a control group (no exercise, n = 54), (ii) a moderate intensity exercise group (MOD-EX, n = 48), or (iii) a vigorous intensity exercise group (VIG-EX n = 43) by unrestricted randomization. No relevant adverse events were recorded. 97 participants (34 men, 63 women) were included in the final analysis (Control; n = 35, MOD-EX; n = 31, and VIG-EX; n = 31). We observed no changes in BAT volume (Δ Control: −22.2 ± 52.6 ml; Δ MOD-EX: −15.5 ± 62.1 ml, Δ VIG-EX: −6.8 ± 66.4 ml; P = 0.771) or 18F-fluorodeoxyglucose uptake (SUVpeak Δ Control: −2.6 ± 3.1 ml; Δ MOD-EX: −1.2 ± 4.8, Δ VIG-EX: −2.2 ± 5.1; p = 0.476) in either the control or the exercise groups. Thus, we did not find any evidence of an exercise-induced change on BAT volume or activity in young sedentary adults.
Similar content being viewed by others


Introduction
Brown adipose tissue (BAT) is a mammalian thermogenic tissue, characterized by its ability to dissipate energy as heat via the action of uncoupling protein 1 (UCP1). This is mainly triggered by the activation of the sympathetic nervous system in response to cold1,2,3,4. In the late 2000s, several independent research groups showed BAT to be present and metabolically active in human adults5,6,7,8,9. Moreover, the presence of beige adipocytes, a brown-like type of adipocyte that expresses UCP1 and shows non-shivering thermogenic capacity10, was documented within white adipose tissue (WAT) depots in humans11. Beige adipocyte proliferation and activity can be increased through a process known as WAT browning12.
Over the last decade, BAT and beige adipocyte recruitment and activation have been thought potential targets for combating obesity and its comorbidities13. Initially, it was hypothesized that BAT might have a profound impact on human daily energy expenditure, and might therefore be enlisted to help reduce adiposity14 and improve cardiometabolic health15,16. Although this was found to be true for mice4,17,18, BAT seems to play only a minor role in human daily energy expenditure3,19. BAT is known, however, to secrete several endocrine signaling molecules that might orchestrate favorable cardiometabolic effects20,21,22. Recruiting or activating BAT and WAT browning might still have cardiometabolic health benefits. Mouse studies have shown that exercise induces WAT browning23,24, and exercise might thus be speculated to do the same in humans25. Indeed, exercise stimulates the secretion of many endocrine factors that increase BAT metabolism and WAT browning26. However, exercise also increases heat production, which might downregulate the thermogenic activity of BAT27. Unfortunately, little information is available regarding the effect of exercise on human BAT, and what there is, is controversial28,29.
In the present work, it was hypothesized that exercise training in young sedentary adults increases BAT volume and glucose uptake (as measured by 18F-fluorodeoxyglucose [18F-FDG] uptake) in an intensity-dependent manner (i.e., the greater the exercise intensity, the stronger the BAT responses). A randomized controlled trial was therefore undertaken to investigate the effect of a 24-week supervised exercise, intervention combining endurance and resistance training (moderate or vigorous intensity) on BAT volume, 18F-FDG uptake, and mean radiodensity in young sedentary adults. Here, we show no evidence that BAT volume, 18F-FDG uptake or mean radiodensity levels are modified in response to the exercise training intervention. While exercise reduces adiposity (−11% [mean for both exercise intensity groups]), and improves muscular (+15%) and cardiorespiratory fitness (+11%), these changes are not correlated with initial BAT volume, 18F-FDG uptake or mean radiodensity, nor any changes therein.
Results and discussion
145 young, sedentary adults were randomly assigned to either: (i) a control group (no exercise, hereinafter CON), (ii) a moderate-intensity exercise group (hereinafter MOD-EX), or (iii) a vigorous-intensity exercise group (hereinafter VIG-EX). Both exercise groups performed 150 min/week of endurance training, distributed over 3–4 sessions/week, plus 80 min per week of resistance exercise over two sessions/week (Supplementary Fig. S1). The primary endpoints were BAT volume, 18F-FDG uptake and mean radiodensity, as measured by a static 18F-FDG positron emission tomography/computed tomography (PET/CT) scan following 2 h of personalized cold exposure. The secondary endpoints included body weight and composition, cardiometabolic risk factors (i.e., blood pressure, fasting serum glucose, insulin, triacylglycerols, cholesterol, liver enzymes and C-reactive protein), and physical fitness (i.e., muscular strength and cardiorespiratory capacity).
Study participants
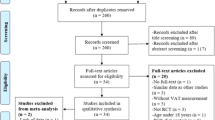
Out of 1127 initially interested individuals, 523 attended one of 76 scheduled information meetings. 126 of the latter individuals declined to participate, and 397 completed a pre-screening survey. Among these, 296 were eligible for screening (Fig. 1). When contacted to schedule their screening visit, 102 declined to participate. The remaining 194 participants provided informed consent to be included in the study, and began baseline assessment; however, 49 did not finish this phase (39 declined to participate, 8 had an abnormal exercise electrocardiogram, and 2 met a medical exclusion criterion). The first participant was enrolled on October 5th, 2015 and the last participant was enrolled on November 7th, 2016. Thus, 145 individuals were finally randomized into the three experimental groups. During the 24-week intervention period, another 38 participants dropped out of the study; 107 participants therefore completed it. Among these, three participants from the MOD-EX group, and two participants from the VIG-EX group, were excluded from the main analyses for attending <70% of the training sessions. Additionally, five participants (MOD-EX; n = 2 and VIG-EX; n = 3) were excluded from the main analyses due to problems in collecting the primary outcome data (the cooling vest or chiller involved suffered technical problems during testing, or the 18F-FDG tracer was improperly injected). The baseline characteristics of the remaining 97 participants (65% women, CON; n = 35, MOD-EX; n = 31, and VIG-EX; n = 31) were similar across the three experimental groups (all P ≥ 0.059, Table 1 and Supplementary Table S1).

BMI body mass index, CON control group, MOD-EX moderate-intensity exercise group, VIG-EX vigorous-intensity exercise group, ECG electrocardiogram.
No evidence of brown adipose tissue volume, 18F-fluorodeoxyglucose uptake, or mean radiodensity changes after 24 weeks of supervised exercise training
Neither the MOD-EX nor VIG-EX regimen significantly altered BAT volume (Δ [post-baseline values]: Δ CON = −22.2 ± 52.6 mL (mean ± standard deviation); Δ MOD-EX = −15.5 ± 62.1 mL; Δ VIG-EX = −6.8 ± 66.4 mL; p = 0.771, Fig. 2a). Nor did they alter 18F-FDG uptake (standardized uptake value [SUV] mean: Δ CON = −0.4 ± 0.7; Δ MOD-EX = −0.4 ± 1.0; Δ VIG-EX = −0.5 ± 1.1; P = 1.000, Fig. 2b; SUVpeak: Δ CON = −2.6 ± 3.1; Δ MOD-EX = −1.2 ± 4.8; Δ VIG-EX = −2.2 ± 5.1: P = 0.476, Fig. 2c). In addition, neither BAT volume nor 18F-FDG uptake in different BAT depots (i.e., laterocervical, supraclavicular, mediastinum or paravertebral areas; all P > 0.1, Fig. 2e) were significantly modified. BAT mean radiodensity (a proxy of fat content30 also remained unchanged (Δ CON = −0.04 ± 6.91 Hounsfield Units [HU]; Δ MOD-EX = 2.2 ± 3.5 HU; Δ VIG-EX = −2.7 ± 10.7 HU; P = 0.441, Fig. 2d). We repeated the analyses using mixed-effects regression models and the absence of evidence of BAT activation after supervised exercise training persisted (Supplementary Fig. S2).

a Total BAT volume. b Total BAT SUVmean. c Total BAT SUVpeak. d Total BAT mean radiodensity (CON n = 25; MOD-EX n = 17; VIG-EX n = 16). E Regional BAT volume, SUVmean, and SUVpeak. SUV values are shown relative to lean mass. Δ was calculated as post-intervention minus baseline values for every outcome. P values are from analyses of covariance adjusting for baseline values (n = 97). In panel e, all P values ≥0.1. CON control group, HU Hounsfield Units, MOD-EX Moderate-intensity exercise group, VIG-EX Vigorous-intensity exercise group. Bars represent mean and standard deviation. Source data are provided as a Source Data file.
Previous clinical studies have shown that BAT volume and 18F-FDG uptake in response to mild-cold and thermoneutral exposures are different in women and men31,32, which was also confirmed in this cohort33. However, the absence of evidence of BAT activation after exercise training was recorded for both sexes when analyzed separately (all P > 0.7). Only participants who attended ≥70% of the training sessions were included in the main analyses (Supplementary Fig. S3), although the results did not change when sensitivity analyses were performed including participants whose attendance was <70% and ≥85%.
Following the recommendations of the Brown Adipose Reporting Criteria in Imaging STudies (BARCIST 1.034) report, BAT was defined as those imaging voxels with a radiodensity between −190 and −10 HU, and a SUV higher than an individualized threshold (1.2/[lean mass/body mass]). Both our research group and others have reported there to be inter-study heterogeneity regarding the criteria used for BAT quantification in 18F-FDG PET/CT scans (i.e., radiodensity range and SUV threshold)35,36,37. Our group also showed that the most frequently used criteria for measuring BAT provide non-comparable estimates of BAT volume and 18F-FDG uptake35. Hence, the use of different criteria might sometimes allow the effect of an intervention to be detected. Accordingly, in the present work, sensitivity analyses were performed using alternative criteria to quantify BAT (i.e., radiodensity: −250/−50 HU and SUV threshold >2.0; and radiodensity: −180/−10 HU and SUV threshold > 1.5). The lack of evidence of BAT activation persisted (all P > 0.5).
In agreement with the present results, a previous study29 showed that six weeks of moderate resistance training did not modify BAT 18F-FDG uptake, although a slight reduction in BAT volume was seen in the laterocervical region in 11 men. However, the latter study did not include a control group, limiting the conclusions that can be drawn. BAT volume and 18F-FDG uptake are strongly influenced by outdoor temperature, with activation greater in colder months38,39,40,41,42,43,44,45,46,47; therefore, not including a control group leaves it impossible to know if any changes in BAT volume and/or 18F-FDG uptake were the result of seasonal temperature variation or a consequence of the intervention. The present results clearly support this notion, since the Δ outdoor ambient temperature was negatively associated with Δ BAT volume, Δ 18F-FDG uptake and Δ BAT mean radiodensity (all R2 > 0.09 and P < 0.001, Fig. 3a–d) in all three groups. These correlations remained unaltered when BAT-related outcomes were calculated for individual BAT depots separately (all r ≤ −0.207 and P ≤ 0.043, Fig. 3e). At baseline, we found that outdoor ambient temperature at which the PET/CT scans were performed negatively correlated with BAT-related outcomes (all r ≥ −0.364 and P < 0.001, Supplementary Table S2), although these significant correlations disappeared when post-intervention values were used instead (Supplementary Table S2). After observing these correlations, we performed the main analyses adding the outdoor ambient temperature as covariate and the results did not change (all P ≥ 0.182; Supplementary Table S3). In addition, we found weak to moderate correlations (range from r = 0.515 to r = 0.872) between baseline and post-intervention BAT-related outcomes, which suggests that our protocol is reproducible despite the presence of large seasonal variation (Supplementary Table S4).

a Total BAT volume. b Total BAT standardized uptake value (SUV) mean. c Total BAT SUVpeak. d Total BAT mean radiodensity (CON n = 25; MOD-EX n = 17; VIG-EX n = 16). e Regional BAT volume, SUVmean, and SUVpeak. SUV values are shown relative to lean mass. P and β values are obtained from linear regression analyses. β non-standardized coefficients, BAT brown adipose tissue, CON Control group, HU Hounsfield units, MOD-EX moderate-intensity exercise group, R2 explained variance, SUV standardized uptake value, VIG-EX vigorous-intensity exercise group, WAT white adipose tissue.
The present BAT assessments were made after a personalized 2 h cold exposure, i.e., based on the participants’ shivering threshold - a proxy of cold tolerance16. While this method is widely used15,33,34 it has been suggested that it might not be entirely adequate. Shivering patterns are variable among individuals, making the detection of shivering onset difficult to be determined objectively48,49. Moreover, exercise has been reported to increase cold tolerance50, and could therefore alter the detection of shivering onset during post-intervention personalized cold exposure, introducing a bias regarding the effect of exercise on BAT recruitment/activation. In the present work, however, the shivering threshold (assessed via the cooling vest water temperature at the onset of shivering [see Methods]) was not modified in any of the groups after the intervention (P = 0.154, Supplementary Table S1).
The lack of evidence of BAT volume, 18F-FDG uptake or mean radiodensity modification after exercise training is in line with the results of cross-sectional studies that show no association of BAT-related outcomes with objectively measured free-living physical activity51 or muscular or cardiorespiratory fitness52. Case-control studies have revealed, however, that endurance-trained athletes show lower BAT volumes and 18F-FDG uptakes than their sedentary counterparts53,54. It is thus conceivable that the high volume of exercise training undertaken by endurance-trained athletes reduces BAT volume and 18F-FDG uptake as an adaptation to high activity energy expenditure levels, while the more moderate exercise training regimens implemented in the present study do not. This hypothesis concurs with the constrained total energy expenditure model, which suggests that low levels of physical activity do not inhibit energy-consuming physiological processes such as BAT thermogenesis55, whereas higher levels of physical activity do in order to maintain total daily energy expenditure within a homeostatic range56,57.
Although 18F-FDG PET/CT scanning is still the most widely used technique for the in vivo assessment of human BAT, the use of 18F-FDG has important limitations58. Cold exposure increases BAT 18F-FDG uptake, but the amount of 18F-FDG taken up does not necessarily mimic the BAT’s thermogenic activity, since most glucose taken up by BAT does not fuel mitochondrial oxidative capacity59,60. Accordingly, insulin infusions increase human BAT 18F-FDG uptake without increasing BAT perfusion, suggesting that the increase in 18F-FDG uptake is not paralleled by increased BAT thermogenic activity61. 18F-FDG is taken up by BAT through insulin-independent (glucose transporter 1, GLUT-1) and insulin-dependent (GLUT-4) mechanisms62. Consequently, BAT insulin sensitivity is likely to partially bias the assessment of BAT volume and activity, when performing 18F-FDG uptake quantification63. Any intervention that changes BAT insulin sensitivity might therefore result in a different 18F-FDG uptake, regardless of the change in BAT thermogenic activity. Indeed, exercise is known to increase insulin sensitivity in many peripheral tissues64, so it is plausible that it modifies BAT insulin sensitivity too. Moreover, exercise training increases mitochondrial oxidative capacity in skeletal muscle65, and it might likewise increase BAT oxidative metabolism rather than BAT 18F-FDG uptake. BAT oxidative metabolism, as well as the uptake of fatty acids in human BAT, has been recently quantified by 11C-acetate, 15O-oxygen and 18F-fluoro-thiaheptadecanoic acid (18FTHA) PET in response to cold exposure in humans48,66,67,68. Thus, it would be interesting to ascertain in future studies if assessing BAT metabolism by methods other than glucose uptake would unveil whether exercise can activate/recruit BAT.
Even if a better PET radiotracer were available, PET/CT imaging would still be affected by important limitations when evaluating the effect of exercise on BAT recruitment/activation. It has been suggested that the human BAT detectable by PET/CT scanning in the laterocervical and supraclavicular areas is composed of a combination of brown and beige-like adipocytes69,70,71,72,73. Most preclinical studies have shown that exercise induces WAT browning23,24, although these results might be just applicable to room temperature environments (i.e., below thermoneutrality74,75). Thus, exercise might not increase the volume or activity of the brown-like depots detectable by PET/CT scanning, but may still induce the browning of small clusters of adipocytes, that are not detected by this technique. If this is the case, the limited resolution of PET imaging (usually 4 mm) would not allow the appearance of beige cells within the WAT to be captured58. The effect of exercise on BAT volume/activity and WAT browning needs to be further explored as better methods become available.
The present finding that exercise seems not to alter BAT volume nor activity in human adults should also be tested in new studies involving different types of exercise program and populations. It is well known that different exercise types (endurance vs. resistance vs. a combination of both) and intensities induce different physiological adaptations76. The present exercise regimens combined resistance and endurance exercises, but it cannot be determined from the results whether the resistance or endurance components on their own might have different effects on BAT recruitment/activation. Interestingly, we found that outdoor ambient temperature influenced BAT volume, 18F-FDG uptake and radiodensity, which might be masking the possible effect of exercise on BAT recruitment/activity. Thus, other study designs and experimental settings, with longer durations, and taking into account the potential effect of outdoor ambient temperature, should be implemented for addressing this scientific question. Finally, BAT presence and activity are reported to be blunted by aging6,13,77,78,79 and metabolic disease46. Since the present work involved relatively healthy young sedentary adults, the findings made may not apply to older or metabolically compromised individuals.
Twenty-four weeks of supervised exercise training reduces adiposity and increases muscular and cardiorespiratory fitness
Exercise reduced both total body fat (Δ CON = −0.3 ± 3.5 kg; Δ MOD-EX = −2.1 ± 2.3 kg; Δ VIG-EX = −2.7 ± 3.8 kg; P = 0.021) and visceral fat mass (Δ CON = −8.6 ± 90.3 g; Δ MOD-EX = −44.5 ± 57.9 g; Δ VIG-EX = −66.7 ± 91.3 g; P = 0.021), although post-hoc comparisons detected differences only between the CON and VIG-EX groups (Fig. 4a and Supplementary Table S1). As expected, exercise tended to increase lean mass in both intervention groups, although only a trend was seen with respect to the control group (P = 0.213, Fig. 4a and Supplementary Table S1). No evidence of a reduction in body weight (P = 0.283, Fig. 4a), or improvements on blood pressure, fasting serum concentrations of glucose, insulin, liver enzymes (i.e., γ-GT, ALT and ALP), cholesterol (i.e., HDL-C and LDL-C), triacylglycerols, and C-reactive protein (all P ≥ 0.092, Fig. 4b and Supplementary Table S1) after the exercise intervention were observed. These findings concur with those of previous exercise intervention studies in relatively healthy individuals80,81. The lack of evidence of an improvement in cardiometabolic risk factors after exercise training may be related to the young age (22 ± 2 years old) and the relatively healthy status of the present participants, whose cardiometabolic risk markers were usually within normal ranges.

a Body weight and composition parameters, b cardiometabolic risk factors, and c physical fitness parameters. Δ was calculated as post-intervention minus baseline value for every outcome. Serum concentrations were log10 transformed. P values are from analyses of covariance (ANCOVAs), adjusting for baseline values. * and † indicate significant differences between pairs after Bonferroni correction. BP Blood pressure, CON Control group, HDL-C high-density lipoprotein cholesterol, MOD-EX Moderate-intensity exercise group, RM repetition maximum, VAT visceral adipose tissue, VO2 oxygen consumption, VIG-EX vigorous-intensity exercise group. Bars represent the mean and standard deviation. Source data are provided as a Source Data file.
The intervention enhanced lower body muscular strength as measured via the repetition maximum (RM) leg press test (Δ CON = 3.7 ± 30.8 kg; Δ MOD-EX = 20.5 ± 31.1 kg; Δ VIG-EX = 26.3 ± 37.7 kg; P = 0.049, Fig. 4c, and Supplementary Table S1), whereas a lack of effect was observed on RM bench press or handgrip strength results after the exercise intervention (all P ≥ 0.993, Supplementary Table S1). In addition, the intervention increased the time to exhaustion in a maximum effort test (Δ CON = 21.8 ± 124.0 s; Δ MOD-EX = 144.2 ± 109.8 sec; Δ VIG-EX = 142.2 ± 96.2 s; P < 0.001, Fig. 4c) and VO2peak (Δ CON = 28 ± 371 mL/min; Δ MOD-EX = 305 ± 367 mL/min; Δ VIG-EX = 285 ± 376 mL/min; P = 0.006, Fig. 4c and Supplementary Table S1), although no significant differences were seen between the exercise groups. Only those participants who attended ≥70% of the total training sessions were included in the main analyses (Supplementary Fig. S3), but the results remained unaltered when other attendance criteria were taken into account (<70%, or ≥85%).
Exercise-induced changes in adiposity, muscular, and cardiorespiratory fitness do not correlate with any changes in brown adipose tissue
Preclinical studies have shown that, during exercise, BAT secretes signaling molecules that favor skeletal muscle function82,83,84. Thus, it may be hypothesized that individuals with higher BAT volumes might benefit to a greater extent from exercise. However, no significant correlations were detected between baseline values, or any change in BAT-related outcomes, and any exercise-induced changes in body composition, cardiometabolic risk profile, muscular strength or cardiorespiratory capacity (all P > 0.1, Supplementary Table S5). Although significant correlations were found between changes in total plasma cholesterol and BAT-related outcomes in the CON and MOD-EX groups, these did not persist after false discovery rate correction (all q values ≥0.54; Supplementary Table S5). These data agree with the findings of a previous study in which no relationship was seen between exercise-induced reduction in adiposity or improvement in the lipoprotein profile, and exercise-induced changes in BAT 18F-FDG uptake29. These observations suggest that the cardiometabolic improvements induced by the exercise intervention were not mediated by BAT activation, at least as quantified by 18F-FDG PET-CT.
In conclusion, there was no evidence of changes in BAT-related outcomes after 24-week supervised exercise intervention combining resistance and endurance training at different intensities in young sedentary adults. The exercise intervention reduced adiposity and enhanced muscular and cardiorespiratory fitness to a comparable extent in both exercise groups, but seemed not to modify other cardiometabolic risk factors. These exercise-induced changes in adiposity, muscular and cardiorespiratory fitness were not correlated with any individual changes in BAT-related outcomes, suggesting that the observed exercise-induced benefits are independent of BAT in such young sedentary adults.
Methods
Participant details
The study was approved by the Ethics Committee on Human Research of the University of Granada (no. 924) and by the Servicio Andaluz de Salud (Centro de Granada, CEI-Granada, Spain). All participants provided informed consent in order to be included. A total of 145 young sedentary adults aged 18–25 years old participated in the Activating Brown Adipose Tissue Through Exercise (ACTIBATE) study (ClinicalTrials.gov ID: NCT02365129; Fig. 1)85. For participant recruitment, the study was advertised through social networks, local media, and via posters. The inclusion criteria included self-reported sedentary lifestyle (performing a maximum of 20 min of moderate-to-vigorous physical activity per day on less than three days per week), being a non-smoker, not taking any medication, and having a stable body weight over the last three months. The exclusion criteria were: having been diagnosed with diabetes, hypertension, or any other significant medical condition (either life-threatening or that might interfere with or be aggravated by exercise), being pregnant, using medication deemed to affect energy metabolism, or to be frequently exposed to cold temperatures85.
Study design
After baseline examination, participants were assigned to one of three groups via computer-generated simple unrestricted randomization86: (i) a control group (no exercise, CON), (ii) a moderate-intensity exercise group (MOD-EX), and (iii) a vigorous-intensity exercise group (VIG-EX). The study was conducted over two consecutive years (from September 2015 to June 2016, and from September 2016 to June 2017). In both years, participants were enrolled over four waves (16–24 participants each) starting between September and December. The first participant was enrolled on October 5th, 2015 and the last participant was enrolled on November 7th, 2016. All outcome assessments were made at the same time of day before and after the 24 weeks intervention. All participants were instructed not to modify their normal routine or their physical activity or dietary pattern over the study period.
Supervised exercise training program
A detailed description of the supervised exercise training program used in this work, which combined resistance and endurance training as recommended by World Health Organization (WHO) guidelines87, has been previously published82. For 24 weeks, participants trained 3–4 times per week, completing a total of 150 min/week of endurance exercise (performed in all sessions) and 80 min/week of resistance exercise (performed over 2 sessions/week) at the same training center. Both resistance and endurance training were individualized to each participant’s physical fitness. The MOD-EX group performed resistance training at 50% of the repetition maximum (RM), whereas the VIG-EX group trained with loads equivalent to 70% RM. The calculation of RM loads is described below and was adjusted monthly (Supplementary Fig. S1). All endurance training in the MOD-EX group was performed at 60% heart rate reserve (HRres), whereas in the VIG-EX group it was performed for 75 min/week at 60% HRres and 75 min/week at 80% HRres. HRres was calculated as the difference between the resting and maximum heart rates. The exercise intervention was organized in five phases of different duration, starting with a four-week familiarization phase (see detailed description Supplementary Fig. S1).
Participants exercised in groups of 10–12 people at the same time of day over the 24 weeks intervention (either 8.30–10.30 a.m., 4–6 p.m., 6–8 p.m., or 8–10 p.m). Attendance was registered via an electronic attendance sheet. Adherence to the prescribed intensity of endurance training was quantified by heart rate monitors (RS800CX, Polar Electro Öy, Kempele, Finland).
Primary endpoints: brown adipose tissue measurements
Shivering threshold test
For personalizing the cooling protocol used to activate BAT, the participants’ shivering threshold was determined 48–72 h before BAT volume and metabolism assessments. Participants first entered a warm room (22.1 ± 1.6 °C) where they rested in a sitting position for 30 min. They then entered in an air-conditioned room (19.8 ± 0.5 °C) and sat in a chair. After 15 min, they were asked to put on a temperature-controlled, water-perfused cooling vest covering the abdomen, chest, and supraclavicular region (Polar Products Inc., Stow, OH, USA). The water temperature was initially set at 16.6 °C and reduced slightly every 10 min until reaching 5.5 °C. If shivering was not detected at this point, the water temperature was decreased by 0.6 °C every 15 min until 3.8 °C was reached. If shivering did not occur, participants remained in the cold room for another 45 min (water at 3.8 °C). Shivering onset was visually detected by the researcher and confirmed by the participants themselves. The water temperature at shivering onset was deemed the shivering threshold and was used for determining the cooling vest water temperature during the personalized cooling protocol before the 18F-FDG-PET/CT scan (4 °C above the shivering threshold). If shivering did not occur, participants started the personalized cooling protocol before the 18F-FDG-PET/CT scan with the water temperature set at 3.8 °C.
Personalized cooling protocol and positron emission tomography/computed tomography scanning
Forty-eight to 72 h after the shivering threshold test, participants went to the Hospital Virgen de las Nieves in Granada (Spain) for the assessment of BAT volume, 18F-FDG uptake, and radiodensity. After resting in a warm room, they were placed in a cool room (19.5–20 °C) wearing the same cooling vest with the water temperature set at the personalized temperature, as explained above. After the first hour of cold exposure, the participants received an injection of 18F-FDG (~185 MBq) and the water temperature was increased by 1 °C to avoid shivering. The water temperature was also slightly increased at any time participants reported shivering. One hour later, they were subjected to 18F-FDG-PET/CT scanning in the supine position using a Siemens Biograph 16 PET/CT scanner (Siemens, Erlangen, Germany). Image acquisition covered an area of two BED positions from the atlas vertebra to thoracic vertebra 6, approximately. The natural calendar day when the baseline, and post-intervention PET/CT scan were performed was recorded from day 1 (January 1st) to day 365/366 (December 31st).
BAT volume, 18F-FDG uptake, and mean radiodensity
BAT volume, 18F-FDG uptake and BAT mean radiodensity were determined following current recommendations34 and using the Beth Israel plug-in for the FIJI program v.188. Several regions of interest (ROIs) were semi-automatically outlined from the atlas vertebra to thoracic vertebra 4, on both the left and right sides of the body: laterocervical, supraclavicular, mediastinum, and paravertebral, which were later computed as a single ROI, as extensively described elsewhere36,89. BAT was defined as those voxels within the ROI showing: (i) a radiodensity between −190 and −10 HU; and (ii) a standardized uptake value (SUV) higher than an individualized threshold (1.2/[lean body mass/body mass])34. BAT volume was calculated as the sum of all voxels meeting the above-mentioned criteria. BAT 18F-FDG uptake was determined as the average SUV of all voxels meeting the above-mentioned criteria (SUVmean), and as the average of the three voxels showing the highest 18F-FDG uptake within 1 cm3 of the voxel with the highest 18F-FDG uptake among those meeting the criteria described above (SUVpeak). SUV values were expressed as a function of lean body mass89. BAT mean radiodensity was determined as the average radiodensity of those voxels meeting the aforementioned criteria in a single ROI covering the body (except the mouth) from the atlas to thoracic vertebra 4. Twenty-eight participants showed several voxels classified as BAT outside of the anatomical areas where BAT is located; their data were excluded from BAT mean radiodensity analyses. For sensitivity analyses, BAT volume, 18F-FDG uptake, and BAT mean radiodensity were also determined using other common criteria (i.e., radiodensity: −250/−50 HU and SUV threshold >2.0; and radiodensity: −180/−10 HU and SUV threshold >1.5)35,36.
Outdoor ambient temperature
We downloaded the outdoor ambient temperature from the Spanish National Meteorological Agency daily during the period of the study (from September 1, 2015 to July 1, 2017).
Secondary endpoints
Anthropometrics and body composition
Body composition (i.e., fat, lean, and visceral adipose tissue mass) was measured by dual-energy X-ray absorptiometry scanning using a Hologic Discovery Wi device (Hologic Inc., Bedford, MA, USA). Participant height and weight (barefoot and wearing light clothing) were determined using a model 799 SECA scale and stadiometer (Electronic Column Scale, Hamburg, Germany). Body mass index (BMI) was calculated as body mass (kg) divided by height squared (m2).
Cardiometabolic risk factors
At 1–3 weeks before starting the exercise intervention, and at 3–4 days after the last exercise session, blood samples were drawn in the morning following an overnight fast. These samples were centrifuged and the serum aliquoted and stored at −80 °C for future analyses. Glucose, cholesterol, high-density lipoprotein cholesterol (HDL-C), and triacylglycerols were assessed using an AU5832 automated analyzer (Beckman Coulter Inc., Brea CA, USA). Low-density lipoprotein cholesterol (LDL-C) was estimated using the Friedewald formula90. Insulin was measured using the Access Ultrasensitive Insulin Chemiluminescent Immunoassay Kit (Beckman Coulter Inc., Brea, CA, USA). The homeostatic model assessment (HOMA) index was calculated as insulin (µU/mL) x glucose (mmol/L)/22.5. C-reactive protein was measured by immunoturbidimetric assay, employing the same automated analyzer as above. Liver enzyme (γ-GT, ALT, or ALP) concentrations were determined using a Beckman Coulter AU5832 analyzer and the appropriate Beckman Coulter reagent. Resting blood pressure was measured in the sitting position before and after exercise training on three non-consecutive days using an automatic Omrom M2 device (Omron Healthcare, Kyoto, Japan). Three measurements were made and the mean blood pressure calculated as diastolic blood pressure + 0.33 × (systolic blood pressure-diastolic blood pressure).
Physical fitness
Physical fitness was assessed in two different sessions, one focusing on muscular strength and the other on cardiorespiratory fitness. Before each session, participants fasted for 3–5 h, performed no vigorous exercise in the previous 48 h, nor moderate exercise in the previous 24 h, and did not consume caffeine-containing beverages on the day of the tests.
Muscular strength
Muscular strength was determined via the handgrip strength and RM leg and bench press tests. The handgrip strength test was performed using a Takei 5401 digital Grip-D hand dynamometer (Takei, Tokyo, Japan). Participants were asked to squeeze the grip gradually and continuously, until reaching maximum intensity. The test was performed twice with each hand, alternating between hands with a 1 min rest after each attempt. Men executed the test with the grip span of the dynamometer fixed at 5.5 cm, while it was adjusted to the hand size for women, according to a validated equation91. The maximum strength recorded in each hand was selected and the mean used in analyses.
Leg press RM was assessed using an A300/Model 2531 pneumatic leg press machine (Keiser Corporation, Fresno, CA, USA). To warm-up, participants first performed a set of 10 repetitions with a self-selected light weight. They then performed a set of eight repetitions using a load with which they could perform a 15-repetition maximum. After a 1 min recovery period, the resistance load was increased by the researcher, aiming to set a target load at which the participant could perform fewer than 10 repetitions (all participants were instructed to perform as many repetitions as they could). The test was stopped after 3–4 repetitions if the participants felt they could perform more than 10 repetitions with the resistance load set. A greater load was then selected, and the test repeated after resting for 5 min. No more than three attempts were allowed for assessing the RM. Later, following a similar procedure, each participant performed a bench press RM test using a bench within a Model 3111 pneumatic power rack (Keiser Corporation, Fresno, CA, USA). The RM was estimated by a standard equation92.
Cardiorespiratory fitness
Cardiorespiratory fitness (i.e., maximum oxygen consumption) was assessed by a maximum graded exercise test on a treadmill, (H/P/Cosmos Sports & Medical GmbH, Nussdorf-Traunstein, Germany), following the modified Balke protocol93. The warm-up consisted of walking at 3 km/h for 1 min, followed by 2 min at 4 km/h (0% slope). The incremental protocol started at a speed of 5.3 km/h and 0% slope. The slope was then increased by 1% every minute until the participants became exhausted (i.e., volitional exhaustion). Finally, participants went through a cooling-down period, walking at 4 km/h (0% slope) for 5 min. During the whole test, respiratory gas exchange (oxygen consumption [VO2] and carbon dioxide production [VCO2]) was recorded via indirect calorimetry using a CPX Ultima CardioO2 metabolic cart (Medical Graphics Corp, St. Paul, MN, USA), equipped with a model 7400 plastic facemask (Hans Rudolph Inc., Kansas City, MO, USA) and a preVent™ high metabolic flow sensor (Medical graphics Corp, St. Paul, MN, USA). The VO2peak was registered after excluding obvious artefacts.
We also measured other variables (secondary outcomes) such as appetite-related sensations and energy intake in an ad libitum meal test, thermal perceptions, heart rate variability and energy expenditure in response to cold and a standardized meal85. However, for the shake of simplicity and clarity we decided not to include those outcomes in this manuscript.
Quantification and statistical analysis
A conservative approach to sample size estimation was followed, and a relatively large standard deviation assumed based on the heterogeneity of the data published on humans up to the time when the study was designed (March 2014). Increases of 10% and 20% were anticipated in activated BAT volume at 24 weeks in the MOD-EX and VIG-EX groups respectively (rising from a baseline level of 50–70 mL), along with a standard deviation of 50–60 mL. Assuming an effect in either direction, differences of at least 10% in BAT volume could be detected with a power of >80% and an α of 0.05 in a group of 17 participants per study group. To study sex differences, a total of 34 participants (17 men and 17 women) were required for each group. Assuming a maximum loss to follow-up of 30%, 150 participants were thus targeted (i.e., 50 per group). The IBM-SPSS Sample power software (version 22) was used for calculations.
Data are expressed as mean ± standard deviation (SD), unless otherwise stated. Data normality was examined using the Shapiro-Wilk test, visual histograms, and Q-Q plots. None of the blood markers were normally distributed; their values were therefore log10 transformed for analyses. Delta values (Δ: post-baselines values) were calculated for every outcome. To study the effect of the intervention on the primary (i.e., Δ BAT-related outcomes) and secondary (i.e., Δ body composition, Δ cardiometabolic risk factors, Δ physical fitness) endpoints, analyses of covariance (ANCOVA) were conducted including the corresponding baseline value as a covariate. Bonferroni post-hoc adjustments for multiple comparisons were used to examine differences between the three groups. As sensitivity analyses, we performed mixed-effects regression models with random intercepts to the primary hypothesis with BAT volume, BAT SUVmean, BAT SUVpeak, and BAT mean radiodensity (Supplementary Fig. S2). Pearson correlations were performed to analyze the correlation between Δ outdoor ambient temperature and Δ BAT-related outcomes calculated for specific depots. Univariate linear regression models were used to examine the association between the outdoor ambient temperature when the baseline PET/CT scan was performed and the Δ BAT-related outcomes. Partial correlations analyses were performed between the Δ body composition, the Δ cardiometabolic risk profile and the Δ physical fitness parameters, and the initial BAT-parameters and Δ BAT-related outcomes adjusting for the outdoor ambient temperature when the baseline PET/CT scan was performed. In these correlations, all P values were corrected by the two-stage step-up procedure of Benjamini, Krieger and Yekutieli for multiple comparisons, controlling for the false discovery rate94. All statistical analyses were performed using the Statistical Package for the Social Sciences v.22.0 (IBM Corporation, Chicago, IL, USA). All graphs were plotted using GraphPad Prism software v.7 (GraphPad Software, San Diego, CA, USA). Significance was set at P < 0.05.
Reporting summary
Further information on research design is available in the Nature Research Reporting Summary linked to this article.
Data availability
Source data as well as the study protocol (see supplementary note 1) are provided with this paper. All of the individual participant data collected during the trial, after deidentification, will be available for any researchers who provide a methodologically sound proposal. Proposals should be directed to ruizj@ugr.es. To gain access, data requestors will need to sign a data access agreement and the data will be provided to achieve the aims of the approved proposal. All type of analysis is allowed. These proposals may be submitted up to 60 months following article publication. After this period, data will be available in our University’s data warehouse but without investigator support other than deposited metadata. Source data are provided with this paper.
References
Nedergaard, J., Bengtsson, T. & Cannon, B. Unexpected evidence for active brown adipose tissue in adult humans. Am. J. Physiol. Endocrinol. Metab. 293, E444–E452 (2007).
Orava, J. et al. Brown adipose tissue function is accompanied by cerebral activation in lean but not in obese humans. J. Cereb. Blood Flow. Metab. 34, 1018–1023 (2014).
Din, M. U. et al. Human brown adipose tissue [(15)O]O2 PET imaging in the presence and absence of cold stimulus. Eur. J. Nucl. Med. Mol. imaging 43, 1878–1886 (2016).
Cannon, B. & Nedergaard, J. Brown adipose tissue: function and physiological significance. Physiological Rev. 84, 277–359 (2004).
van Marken Lichtenbelt, W. D. et al. Cold-activated brown adipose tissue in healthy men. N. Engl. J. Med. 360, 1500–1508 (2009).
Cypess, A. M. et al. Identification and importance of brown adipose tissue in adult humans. N. Engl. J. Med. 360, 1509–1517 (2009).
Virtanen, K. A. et al. Functional brown adipose tissue in healthy adults. N. Engl. J. Med. 360, 1518–1525 (2009).
Saito, M. et al. High incidence of metabolically active brown adipose tissue in healthy adult humans: effects of cold exposure and adiposity. Diabetes 58, 1526–1531 (2009).
Zingaretti, M. C. et al. The presence of UCP1 demonstrates that metabolically active adipose tissue in the neck of adult humans truly represents brown adipose tissue. FASEB J. 23, 3113–3120 (2009).
Petrovic, N. et al. Chronic peroxisome proliferator-activated receptor gamma (PPARgamma) activation of epididymally derived white adipocyte cultures reveals a population of thermogenically competent, UCP1-containing adipocytes molecularly distinct from classic brown adipocyt. J. Biol. Chem. 285, 7153–7164 (2010).
Wu, J. et al. Beige adipocytes are a distinct type of thermogenic fat cell in mouse and human. Cell 150, 366–376 (2012).
Montanari, T., Pošćić, N. & Colitti, M. Factors involved in white-to-brown adipose tissue conversion and in thermogenesis: a review. Obes. Rev. 495–513. https://doi.org/10.1111/obr.12520 (2017).
Ruiz, J. R. et al. Role of human brown fat in obesity, metabolism and cardiovascular disease: strategies to turn up the heat. Prog. Cardiovasc. Dis. 61, 232–245 (2018).
Hanssen, M. J. W. et al. Short-term cold acclimation recruits brown adipose tissue in obese humans. Diabetes 65, 1179–1189 (2016).
Hanssen, M. J. et al. Short-term cold acclimation recruits brown adipose tissue in obese humans. Diabetes 65, 1179–89 (2016).
van der Lans, A. A. J. J. et al. Cold-activated brown adipose tissue in human adults: methodological issues. AJP Regul. Integr. Comp. Physiol. 307, R103–R113 (2014).
Luna, F., Roca, P., Oliver, J. & Antenucci, C. D. Maximal thermogenic capacity and non-shivering thermogenesis in the South American subterranean rodent Ctenomys talarum. J. Comp. Physiol. B 182, 971–983 (2012).
Berbée, J. F. P. et al. Brown fat activation reduces hypercholesterolaemia and protects from atherosclerosis development. Nat. Commun. 6, 6356 (2015).
Din, M. U. et al. Postprandial oxidative metabolism of human brown fat indicates thermogenesis. Cell Metab. 1–10 https://doi.org/10.1016/j.cmet.2018.05.020 (2018).
Deshmukh, A. S. et al. Proteomics-based comparative mapping of the secretomes of human brown and white adipocytes reveals EPDR1 as a novel batokine. Cell Metab. 30, 963–975.e7 (2019).
Scheele, C. & Wolfrum, C. Brown adipose crosstalk in tissue plasticity and human metabolism. Endocr. Rev. 41, 53–65 (2020).
Villarroya, F., Cereijo, R., Villarroya, J. & Giralt, M. Brown adipose tissue as a secretory organ. Nat. Rev. Endocrinol. 13, 26–35 (2017).
Lehnig, A. C. et al. Exercise training induces depot-specific adaptations to white and brown adipose tissue. iScience 11, 425–439 (2019).
De Matteis, R. et al. Exercise as a new physiological stimulus for brown adipose tissue activity. Nutr., Metab., cardiovascular Dis. 23, 582–590 (2013).
Ruiz, J. R., Martinez-Tellez, B., Sanchez-Delgado, G., Aguilera, C. M. & Gil, A. Regulation of energy balance by brown adipose tissue: at least three potential roles for physical activity. Br. J. Sports Med. https://doi.org/10.1136/bjsports-2014-094537 (2015).
Mendez-Gutierrez, A., Osuna-Prieto, F. J., Aguilera, C. M., Ruiz, J. R. & Sanchez-Delgado, G. Endocrine mechanisms connecting exercise to brown adipose tissue metabolism: a human perspective. Curr. Diabetes Rep. 20, 40 (2020).
Sanford, J. A. et al. Molecular Transducers of Physical Activity Consortium (MoTrPAC): mapping the dynamic responses to exercise. Cell 181, 1464–1474 (2020).
Motiani, P. et al. Decreased insulin-stimulated brown adipose tissue glucose uptake after short-term exercise training in healthy middle-aged men. Diabetes Obes. Metab. 19, 1379–1388 (2017).
Motiani, P. et al. Exercise training alters lipoprotein particles independent of brown adipose tissue metabolic activity. Obes. Sci. Pract. 5, 258–272 (2019).
Din, U. M. et al. Human brown fat radiodensity indicates underlying tissue composition and systemic metabolic health. J. Clin. Endocrinol. Metab. 102, 2258–2267 (2017).
Pfannenberg, C. et al. Impact of age on the relationships of brown adipose tissue with sex and adiposity in humans. Diabetes 59, 1789–1793 (2010).
Fletcher, L. A. et al. Sexual dimorphisms in adult human brown adipose tissue. Obesity 28, 241–246 (2020).
Martinez-Tellez, B. et al. A new personalized cooling protocol to activate brown adipose tissue in young adults. Front. Physiol. 8, 863 (2017).
Chen, K. Y. et al. Brown Adipose Reporting Criteria in Imaging STudies (BARCIST 1.0): recommendations for standardized FDG-PET/CT experiments in humans. Cell Metab. 24, 210–222 (2016).
Martinez-Tellez, B. et al. The impact of using BARCIST 1.0 criteria on quantification of BAT volume and activity in three independent cohorts of adults. Sci. Rep. 8, 8567 (2018).
Martinez-Tellez, B. et al. Distribution of brown adipose tissue radiodensity in young adults: implications for cold [18F]FDG-PET/CT analyses. Mol. Imaging Biol. https://doi.org/10.1007/s11307-019-01381-y (2019).
Fraum, T. J. et al. Repeatability of quantitative brown adipose tissue imaging metrics on positron emission tomography with 18F-fluorodeoxyglucose in humans. Cell Metab. 30, 212–224.e4 (2019).
Ouellet, V. et al. Outdoor temperature, age, sex, body mass index, and diabetic status determine the prevalence, mass, and glucose-uptake activity of 18F-FDG-detected BAT in humans. J. Clin. Endocrinol. Metab. 96, 192–199 (2011).
Martinez-Tellez, B. et al. Association of wrist and ambient temperature with cold-induced brown adipose tissue and skeletal muscle 18F-FDG uptake in young adults. Am. J. Physiol. Regul. Integr. Comp. Physiol. https://doi.org/10.1152/ajpregu.00238.2018 (2018).
Kim, S., Krynyckyi, B. R., Machac, J. & Kim, C. K. Temporal relation between temperature change and FDG uptake in brown adipose tissue. Eur. J. Nucl. Med. Mol. Imaging 35, 984–989 (2008).
Senn, J. R. et al. Outdoor temperature influences cold induced thermogenesis in humans. Front. Physiol. 9, 1–9 (2018).
Persichetti, A. et al. Prevalence, mass, and glucose-uptake activity of 18F-FDG-detected brown adipose tissue in humans living in a temperate zone of Italy. PLoS ONE 8, 1–8 (2013).
Pace, L. et al. Determinants of physiologic 18F-FDG uptake in brown adipose tissue in sequential PET/CT examinations. Mol. Imaging Biol. 13, 1029–1035 (2011).
Bahler, L., Deelen, J. W., Hoekstra, J. B., Holleman, F. & Verberne, H. J. Seasonal influence on stimulated BAT activity in prospective trials: a retrospective analysis of BAT visualized on 18F-FDG PET-CTs and 123I-mIBG SPECT-CTs. J. Appl. Physiol. 120, 1418–1423 (2016).
Lee, P. et al. Temperature-acclimated brown adipose tissue modulates insulin sensitivity in humans. Diabetes 177, 1–59 (2014).
Becher, T. et al. Brown adipose tissue is associated with cardiometabolic health. Nat. Med. 27 58–65 (2021).
Acosta, F. M. et al. Relationship between the daily rhythm of distal skin temperature and brown adipose tissue 18 F-FDG uptake in young sedentary adults. J. Biol. Rhythms 074873041986540. https://doi.org/10.1177/0748730419865400 (2019).
Blondin, D. P. et al. Dietary fatty acid metabolism of brown adipose tissue in cold-acclimated men. Nat. Commun. 8, 14146 (2017).
Hohtola, E. & González-Alonso, J. Motor unit function during cold induced thermogenesis in muscle—new perspectives on old concepts. Acta Physiol. 228, 1–2 (2020).
Behm, D. G. & Carter, T. B. Effect of exercise-related factors on the perception of time. Front. Physiol. 11, 1–11 (2020).
Acosta, F. M. et al. Association of objectively measured physical activity with brown adipose tissue volume and activity in young adults. J. Clin. Endocrinol. Metab. https://doi.org/10.1210/jc.2018-01312 (2018).
Martinez-Tellez, B., Sanchez-Delgado, G., Amaro-Gahete, F. J., Acosta, F. M. & Ruiz, J. R. Relationships between cardiorespiratory fitness/muscular strength and 18F-fluorodeoxyglucose uptake in brown adipose tissue after exposure to cold in young, sedentary adults. Sci. Rep. 9, 11314 (2019).
Vosselman, M. J. et al. Low brown adipose tissue activity in endurance trained compared to lean sedentary men. Int. J. Obes. 1–7. https://doi.org/10.1038/ijo.2015.130 (2015).
Singhal, V. et al. Effect of chronic athletic activity on brown fat in young women. PLoS One 11, e0156353 (2016).
Sanchez-Delgado, G., Martinez-Tellez, B., Gil, A. & Ruiz, J. R. Is brown adipose tissue-mediated adaptive thermogenesis the missing component of the constrained total energy expenditure model? Ann. Nutr. Metab. 69, 51–53 (2016).
Pontzer, H. Energy constraint as a novel mechanism linking exercise and health. Physiology 33, 384–393 (2018).
Pontzer, H. et al. Constrained total energy expenditure and metabolic adaptation to physical activity in adult humans. Curr. Biol. 1–8. https://doi.org/10.1016/j.cub.2015.12.046 (2016).
Carpentier, A. C. et al. Brown adipose tissue energy metabolism in humans. Front. Endocrinol. 9, 1–21 (2018).
Blondin, D. P. et al. Increased brown adipose tissue oxidative capacity in cold-acclimated humans. J Clin Endocrinol Metab. https://doi.org/10.1210/jc.2013-3901 (2014).
Abu-Farha, M. et al. Brown adipose tissue energy metabolism in humans. Front. Endocrinol. 1, 447 (2018).
Orava, J. et al. Different metabolic responses of human brown adipose tissue to activation by cold and insulin. Cell Metab. 14, 272–279 (2011).
Hoeke, G., Kooijman, S., Boon, M. R., Rensen, P. C. N. & Berbeé, J. F. P. Role of brown fat in lipoprotein metabolism and atherosclerosis. Circulation Res. 118, 173–182 (2016).
Schilperoort, M., Hoeke, G., Kooijman, S. & Rensen, P. C. N. Relevance of lipid metabolism for brown fat visualization and quantification. Curr. Opin. Lipidol. 27, 242–248 (2016).
Cartee, G. D. et al. Prolonged increase in insulin-stimulated glucose transport in muscle after exercise. Am. J. Physiol. Endocrinol. Metab. 256, 494–499 (1989).
Fiorenza, M. et al. High-intensity exercise training enhances mitochondrial oxidative phosphorylation efficiency in a temperature-dependent manner in human skeletal muscle: implications for exercise performance. FASEB J. 33, 8976–8989 (2019).
Richard, M. A. et al. Determination of a pharmacokinetic model for [11c]-acetate in brown adipose tissue. EJNMMI Res. 9, 1–16 (2019).
Blondin, D. P. et al. Inhibition of intracellular triglyceride lipolysis suppresses cold-induced brown adipose tissue metabolism and increases shivering in humans. Cell Metab. 25, 438–447 (2017).
Din, U. M. et al. Human brown adipose tissue [15O]O2 PET imaging in the presence and absence of cold stimulu. Eur. J. Nucl. Med. Mol. Imaging 43, 1878–1886 (2016).
Cypess, A. M. et al. Anatomical localization, gene expression profiling and functional characterization of adult human neck brown fat. Nat. Med. 19, 635–639 (2013).
de Jong, J. M. A. et al. Human brown adipose tissue is phenocopied by classical brown adipose tissue in physiologically humanized mice. Nat. Metab. 1, 830–843 (2019).
Kajimura, S. & Spiegelman, B. M. Confounding issues in the “humanized” BAT of mice. Nat. Metab. 2, 303–304 (2020).
Kellman, G. M. et al. MR imaging of the supraclavicular region: normal anatomy. Am. J. Roentgenol. 148, 77–82 (1987).
Sun, W. et al. snRNA-seq reveals a subpopulation of adipocytes that regulates thermogenesis. Nature 587, 98–102 (2020).
Aldiss, P. et al. Exercise training in obese rats does not induce browning at thermoneutrality and induces a muscle-like signature in brown adipose tissue. Front. Endocrinol. 11, 1–14 (2020).
McKie, G. L. et al. Housing temperature affects the acute and chronic metabolic adaptations to exercise in mice. J. Physiol. 597, 4581–4600 (2019).
Williams, M. A. et al. Resistance exercise in individuals with and without cardiovascular disease: 2007 update: a scientific statement from the American Heart Association Council on Clinical Cardiology and Council on Nutrition, Physical Activity, and Metabolism. Circulation 116, 572–584 (2007).
Rossato, M. Aging and brown adipose tissue activity decline in human: does the brain extinguish the fire? Aging Clin. Exp. Res. 28, 579–581 (2016).
Heaton, J. M. The distribution of brown adipose tissue in the human. J. Anat. 112, 35–39 (1972).
Enerbäck, S. Human brown adipose tissue. Cell Metab. 11, 248–252 (2010).
Harrington, D. M. et al. Cardiometabolic risk factor response to a lifestyle intervention: a randomized trial. Metab. Syndr. Relat. Disord. 13, 125–131 (2015).
Mikus, C. R. et al. The effects of exercise on the lipoprotein subclass profile: a meta-analysis of 10 interventions. Atherosclerosis 243, 364–372 (2015).
Lynes, M. D. et al. The cold-induced lipokine 12,13-diHOME promotes fatty acid transport into brown adipose tissue. Nat. Med. 23, 631–637 (2017).
Stanford, K. I. et al. 12,13-diHOME: an exercise-induced lipokine that increases skeletal muscle fatty acid uptake. Cell Metab. 27, 1111–1120.e3 (2018).
Kong, X. et al. Brown adipose tissue controls skeletal muscle function via the secretion of myostatin. Cell Metab. 0, 1–13 (2018).
Sanchez-Delgado, G. et al. Activating brown adipose tissue through exercise (ACTIBATE) in young adults: Rationale, design and methodology. Contemp. Clin. Trials 45, 416–425 (2015).
Schulz, K. F. & Grimes, D. A. Generation of allocation sequences in randomised trials: chance, not choice. Lancet 359, 515–519 (2002).
World Health Organization. WHO global recommendations on physical activity for health (World Health Organization, Geneva, Switzerland, 2010).
Schindelin, J. et al. Fiji: an open-source platform for biological-image analysis. Nat. Methods 9, 676–682 (2012).
Leitner, B. P. et al. Mapping of human brown adipose tissue in lean and obese young men. Proc. Natl Acad. Sci. USA 114, 8649–8654 (2017).
Friedewald, W. T., Levy, R. I. & Fredrickson, D. S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 18, 499–502 (1972).
Ruiz-Ruiz, J., Mesa, J. L. M., Gutiérrez, A. & Castillo, M. J. Hand size influences optimal grip span in women but not in men. J. Hand Surg. 27, 897–901 (2002).
Wathen, D. Load assignment. In: Essentials of Strength Training and Conditioning. (ed. Baechle, T. R.). pp. 435–439, (Champaign, Human Kinetics, 1994).
Balke, B. & Ware, R. W. An experimental study of physical fitness of Air Force personnel. U. S. Armed Forces Med. J. 10, 675–688 (1959).
Benjamini, Y., Krieger, A. M. & Yekutieli, D. Adaptive linear step-up procedures that control the false discovery rate. Biometrika 93, 491–507(2006).
Acknowledgements
The authors thank all the participants who took part in the study, as well as those researchers who contributed to the study design (Drs. Barbara Cannon, Jan Nedergaard, José A Lopez Calbet, John Blundell, Graham Finlayson, Catherine Gibbons, Jose Antonio Jimenez-Rios, Emilio Martinez de Vitoria, and Maria Dolores Ruiz), data collection (Dr. Carlos de Teresa, Socorro Navarrete, Rosa Lozano, Esther Brea, Dr. Jose Rubio Lopez, Dr. Jose M Pascual, Dr. Josune Olza, Dr. Francisco Ruiz Ojeda, Amalia Cano Nieto, María Ruiz Ruiz, Laura Frutos, Marina Bórrallo, Miguel Angel Contreras Gomez, Juan Prados-Ruiz, Abdel-Karim Ruiz, Dr. Yolanda García Rivero, and Dr. Ángel Ramirez Navarro), and to the discussion of the results (Brooks Leitner and Dr. Mariëtte Boon). This study was funded by the Spanish Ministry of Economy and Competitiveness via the Fondo de Investigación Sanitaria del Instituto de Salud Carlos III (PI13/01393; J.R.R.) and PTA-12264I, Retos de la Sociedad (DEP2016-79512-R; J.R.R.) and European Regional Development Funds (ERDF; J.R.R.), the Spanish Ministry of Education (FPU13/04365 (G.S.D.), FPU14/04172 (F.A.G.), FPU15/04059 (J.M.A.), FPU16/03653 (A.M.G.), FPU16/02828 (F.J.O.P.), FPU16/05159 (H.X.), FPU17/01523 (L.O.A.), FPU19/01609 (L.J.F.)), International Doctoral Studies Scholarship no. 440575 from the Mexican National Council of Science and Technology (CONACYT; WDMA), the Fundación Iberoamericana de Nutrición (FINUT; JRR), the Redes Temáticas de Investigación Cooperativa RETIC (Red SAMID RD16/0022; J.R.R.), the AstraZeneca HealthCare Foundation (J.R.R.), the University of Granada Plan Propio de Investigación 2016 -Excellence actions: Unit of Excellence on Exercise and Health (UCEES) (J.R.R.)- and Plan Propio de Investigación 2018 - Programa Contratos-Puente and Programa Perfecionamiento de Doctores (G.S.D.), the Junta de Andalucía, Consejería de Conocimiento, Investigación y Universidades (ERDF; ref. SOMM17/6107/UGR; JRR), the Junta de Andalucía, Consejería de Economía, Conocimiento, Empresas y Universidad (ref. P18-RT-4455; J.R.R.), the Fundación Alfonso Martín Escudero (B.M.T. and G.S.D.), the Maria Zambrano fellowship by the Ministerio de Universidades y la Unión Europea–NextGenerationEU (RR_C_2021_04; B.M.T.), and the Novo Nordisk Foundation (NNF18OC0032394; M.S.). This study was performed as part of a PhD thesis conducted within the Biomedicine Doctoral Studies Program of the University of Granada, Spain. The funding agencies had no role in study design, data collection and analysis or manuscript writing.
Author information
Authors and Affiliations
Contributions
Conceptualization, I.L., F.B.O., J.M.L.E., A.G., and J.R.R.; Methodology, B.M.T., G.S.D., F.M.A., J.M.L.L. and J.R.R.; Investigation, B.M.T., G.S.D., F.M.A., J.M.A., F.A.G., W.D.M.A., E.M.R., V.M.H., F.J.O.P., L.J.F., H.X., L.O.A., M.A.T, A.M.G., J.R.R.; Writing—Original Draft, BMT, G.S.D., and J.R.R.; Writing—Review & Editing, All authors; Funding Acquisition, C.M.A., A.G., and J.R.R.; Resources, M.S., P.C.N.R., C.M.A., J.M.L.E., A.G., and J.R.R.; Supervision, J.R.R.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Lauren Sparks and the other, anonymous, reviewers for their contribution to the peer review of this work. Peer reviewer reports are available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Martinez-Tellez, B., Sanchez-Delgado, G., Acosta, F.M. et al. No evidence of brown adipose tissue activation after 24 weeks of supervised exercise training in young sedentary adults in the ACTIBATE randomized controlled trial. Nat Commun 13, 5259 (2022). https://doi.org/10.1038/s41467-022-32502-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41467-022-32502-x
This article is cited by
-
Lactate coordinated with exercise promoted the browning of inguinal white adipose tissue
Journal of Physiology and Biochemistry (2024)
-
The Different Shades of Thermogenic Adipose Tissue
Current Obesity Reports (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
