
Abstract
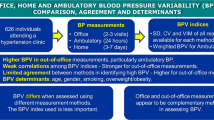
Self-measured blood pressure (BP) at home (HBP) has been commonly used in clinical practice. Although the unattended office BP (UBP), in which a patient is left alone before and during the measurement, has been investigated, the advantages of UBP over HBP or conventionally measured attended office BP obtained using automated devices (CBP) remain unclear. We performed a multicenter clinical study in Japan to compare the UBP, CBP, and HBP among 308 patients with hypertension at 3 clinics (women, 57.8%; mean age 71.8 years; under antihypertensive drug therapy, 96.4%). The patients measured HBP twice in the morning and twice in the evening for 5 days according to the Japanese Society of Hypertension guidelines. Using the Omron HEM-907 cuff-oscillometric device, the UBP and CBP were measured in line with the protocol in the Systolic blood PRessure INtervention Trial (SPRINT) and in accordance with the guidelines, respectively. Correlation coefficients were ≤0.16 for the comparison of UBP versus morning and evening HBP for the systolic measurement, whereas they were approximately 0.5 (P < 0.001) for the diastolic measurement. The difference between UBP minus HBP was small on average but varied among individuals (mean ± SD for UBP minus morning HBP: 0.9 ± 17.8/−4.5 ± 10.5 mmHg; UBP minus evening HBP: 5.7 ± 17.8/−0.1 ± 11.3 mmHg). In contrast, the measurement values of CBP and UBP were highly correlated (r ≥ 0.72), but the difference between CBP minus UBP was 10.4 ± 12.0/4.2 ± 6.5 mmHg. Based on the low correlations and wide range of differences, UBP cannot be used as an alternative to HBP.
Similar content being viewed by others

Introduction
Self-measured blood pressure (BP) at home (HBP) has been commonly used in clinical practice. HBP can identify white-coat and masked hypertension [1, 2], and has a stronger prognostic ability for cardiovascular complications than conventional office BP measured by medical staff [3,4,5]. Because ambulatory BP monitoring has been limited in its dissemination by practical and economic concerns [6], HBP measurement may become a practical and reliable standard for out-of-office BP measurement. The Japanese Society of Hypertension Guidelines for the Management of Hypertension published in 2014 (JSH 2014) [7] led the world in promoting the prioritization of HBP measurement for the diagnosis and treatment of hypertension in routine clinical practice.
Advantages of so-called automated office BP (AOBP) measurement have been highlighted [8, 9] following the publication of impressive results in the Systolic blood PRessure INtervention Trial (SPRINT), wherein significant reductions in cardiovascular complications (by 25%) and even mortality (by 27%) were demonstrated among patients whose AOBP was treated to achieve a target of <120 mmHg for systolic BP compared with a target of <140 mmHg [10,11,12] However, the characteristics of AOBP have yet to be well defined. The initial definition of AOBP [13, 14] does not include antecedent rest, which results in a lower BP value [15] and is recommended in recent guidelines [7, 16, 17]. Furthermore, the use of automated devices for office BP measurement has become increasingly common in recent clinical practice [18]. The essential difference between the initially defined AOBP [13, 14] and conventionally measured office BP therefore comes down to the difference in whether the medical staff is unattended or attended during the measurement. Controversial findings regarding the difference in the unattended office BP and HBP have been reported [19, 20], and whether unattended office BP can be treated as an alternative to HBP or as just a variant of office BP measurements by automated devices also remains unclear. We, therefore, conducted a multicenter clinical study in Japan to compare the HBP, unattended office BP, and conventionally measured attended office BP assessed using automated devices among patients with hypertension.
Methods
Study population
The present COmparison of Self-measured home, Automated unattended office and Conventional attended office blood pressure (COSAC) study was part of a multicenter clinical study comparing the self-measured HBP, unattended office BP, and conventionally measured attended office BP using automated devices among patients with hypertension. The entire study project was designed by the working group of the Japanese Society of Hypertension (see “Acknowledgements”). The study was conducted at Miyakawa Clinic of Internal Medicine and Pediatrics (Yokohama, Japan), Katsuya Clinic (Amagasaki, Japan), and Yokohama Sotetsu bldg. Clinic of Internal Medicine (Yokohama, Japan) where the working group members (MM, TK, and HM, respectively) were administered. The study protocol complies with the recent Declaration of Helsinki for the Investigation of Human Patients [21] and is registered with the UMIN Clinical Trial Registry as an observational study (UMIN000026721; http://www.umin.ac.jp/ctr). The institutional review board of the University of the Ryukyus approved the study protocol (#1042 on February 2, 2017), and all study participants provided their informed consent.
Eligible patients were those with essential hypertension and ≥50 years of age who were able to measure and record their HBP by themselves regularly. Patients who declined to participate in the study or were considered ineligible by their doctors were excluded. Because no similar clinical study comparing these 3 BP values had been conducted, we arbitrarily set the target population size to 300, with doctors at the 3 clinics recruiting 100 patients each. Ultimately, 308 patients across all 3 clinics completed the initial assessment.
BP measurement
HBP values were measured over 5 days just before the clinic visit for the general assessment with office BP measurements. At the clinic visit, study doctors measured the conventional attended office BP before measurement of the unattended office BP to prevent unexpected effects of the unattended office BP measurement on the conventional office BP values. The study patients were asked to maintain the same antihypertensive medications during the HBP and office BP measurements.
The doctors instructed patients on HBP measurement in accordance with the JSH 2014 Guidelines [7] and confirmed the effective use of the popular upper-arm cuff-oscillometric BP monitor. Patients were asked to measure their HBP in the sitting position twice every morning after at least 2 min of rest. They had to obtain these measurements within 1 h of waking, before breakfast, and before taking antihypertensive medication. They were also asked to measure their HBP twice every evening just before going to bed.
Unattended office BP was captured using the validated [22] upper-arm cuff-oscillometric Omron HEM-907 (Omron Healthcare Co. Ltd., Kyoto, Japan) automated sphygmomanometer, which was also used in SPRINT [10,11,12]. Trained medical staff in each clinic set the monitor to automatically wait 5 min and then activate to measure the BP three times consecutively at 1-min intervals. Once the staff left the examination room after attaching a proper-size arm-cuff to the study patient, the patient sat alone in a back-supported chair for the resting period, after which the measurement was automatically performed. Throughout the process, the patient was not completing questionnaires, talking, or texting. This measurement procedure fully complied with the most stringent unattended BP measurement conditions used in SPRINT—patients were left alone during the antecedent rest as well as the BP measurements [12].
Conventional attended office BP was measured in accordance with the JSH 2014 Guidelines [7]. All three study doctors used the same Omron HEM-907 automated sphygmomanometer and directly measured the BPs of their patients in the consultation room. After a few minutes of rest, they measured the office BP twice at the Katsuya Clinic and Yokohama Sotetsu bldg. Clinic with a 1- to 2-min interval, but only once at Miyakawa Clinic, while maintaining the arm-cuff position at the level of the heart in a seated position.
Other measurements and quality control
We used the questionnaire to obtain information on each patient’s medical history and related conditions. We asked the doctors to define each patient’s complications according to the common definition used in Japan, e.g., diabetes mellitus was determined by the use of antidiabetic drugs, a fasting blood glucose concentration of ≥7.0 mmol/L, a random blood glucose concentration of ≥11.1 mmol/L, or diabetes documented in the clinic records. A history of cardiovascular disease included both nonfatal stroke and nonfatal myocardial infarction. The body mass index was the body weight in kilograms divided by the height in meters squared. The amount of antihypertensive medication in individuals was standardized using the defined daily doses (2018 version) [23], which is the assumed average maintenance dose per day for a drug used for its main indication in adults developed by the World Health Organization Collaborating Centre for Drug Statistics Methodology System of Defined Daily Doses.
HBP measurements were recorded on paper and then collected and inspected by each study doctor. The numbers of patients who reported identical systolic/diastolic morning HBPs between 2 consecutive days were 2, 1, 0, and 1 between days 1–2, 2–3, 3–4, and 4–5, respectively, and all these readings came from different patients, indicating markedly limited, if any, reporting bias in the present study. All BP and other measurement data were then sent to the data management center at the University of the Ryukyus. The data manager (YI) independently inspected the collected data and made inquiries to the study doctors as necessary. Before and during the study period, the investigators had biannual meetings in connection with the major scientific conferences and regular monitoring at the three clinic sites to ensure the quality of the study.
Statistical analyses
We used SAS software, version 9.4 (SAS Institute Inc., Cary, NC, USA) for database management and statistical analyses. The statistical significance was α < 0.05 in 2-sided tests. All data are expressed as the mean (SD) unless otherwise stated.
For the HBP, the average morning and evening HBP values were separately analyzed because previous studies have shown that these measurements have different prognostic meanings [24, 25]. For the unattended and attended office BP values, all of the readings were averaged for the analysis.
We performed the Kruskal–Wallis test and Fisher’s exact test to compare means and proportions, respectively. Bland and Altman plots were used to examine the agreement between BP values. Pearson’s correlation coefficients were calculated to determine the correlation between each BP value because BPs can be treated as a normal distribution. The correlations of the mean difference between in-office BPs and HBPs were also assessed to determine whether a white-coat effect, defined as the conventional attended office BP minus the HBP, was present in the unattended office BP. We further applied multiple linear regression models to explore independent factors associated with the mean difference between BP values. For the multivariate analysis, the following factors were included: sex, age, overweight (body mass index ≥ 25 kg/m2), current smoking and drinking status, diabetes, dyslipidemia, cardiovascular disease history, clinic sites, and defined daily doses.
Results
The clinical characteristics of the 308 eligible patients are shown in Table 1. A total of 178 (57.8%) were women, and the mean age was 71.8 years, including 244 patients (79.2%) who were ≥65 years old. All but 11 patients (96.4%) had their BP measured under antihypertensive drug medication. Office BPs were measured from 08:20 to 18:50 within a routine clinical practice at each site, and the median time between attended and unattended office BPs was 10 min (interquartile range: 5–15 min). Of the 308 patients, 304 measured morning HBP over 5 days, and the others performed measurements over 4 days. Evening HBPs were measured by 300 patients, of whom 299, 298, and 295 patients measured evening HBPs over 3, 4, and 5 days, respectively.
Table 2 lists the correlations between unattended and attended office BP and morning and evening HBP. Scatter plots of unattended office and morning HBPs are shown in Supplementary Fig. 1. In the systolic measurement, crude correlation coefficients did not reach 0.10 (P > 0.11) for the comparison of HBPs vs. office BPs, except for attended BP vs. morning HBP (r = 0.12; P = 0.037). In contrast, the measurement values of attended BP vs. unattended BP and those of morning HBP vs. evening HBP were highly correlated (r ≥ 0.73 and ≥0.52, respectively; P < 0.0001). The correlation coefficients of HBP vs. office BPs were approximately 0.5 (P < 0.0001) in diastolic measurements. Similar results were observed when we adjusted for confounders. Of note, the average 3 consecutive unattended office BP measurements ranged from 129.4 (16.5)/71.1 (12.1) mmHg to 128.2 (16.0)/69.9 (12.1) mmHg as the first to third measurements, showing almost identical values among patients (r ≥ 0.90).
The mean difference in the BP values between unattended and morning home measurements, attended and morning home measurements, and attended and unattended measurements were 0.9 (17.8)/−4.5 (10.5), 11.3 (18.3)/−0.3 (10.8), and 10.4 (12.0)/4.2 (6.5) mmHg, respectively, as shown in the Bland and Altman plots in Figs. 1–3. The differences between unattended and evening HBPs and attended and evening HBPs were 5.7(17.8)/−0.1(11.3) mmHg (Supplementary Fig. 2) and 16.3(19.1)/4.3(11.8) mmHg (Supplementary Fig. 3), respectively, and that between morning and evening HBP was 4.7(9.4)/4.3(6.1) mmHg (Supplementary Fig. 4). The mean differences between unattended BP and HBP and between attended BP and HBP—the white-coat effect in a narrow and broad sense, respectively—were highly correlated (morning HBP-based white-coat effects, r = 0.78/0.81; evening-based, 0.79/0.84; P < 0.0001). This finding was consistently observed when patients from the 3 clinic sites were analyzed separately (r ≥ 0.68/≥0.67, P < 0.0001). Correlation coefficients in the Bland and Altman plots were significant when office and HBPs were assessed (Figs. 1 and 2, and Supplementary Figs. 2 and 3; P < 0.0001), but not when attended and unattended as well as morning and evening HBPs were assessed (Fig. 3 and Supplementary Fig. 4; P ≥ 0.080). BPs and defined daily doses in the cross-classification of patients based on HBPs and office BPs are shown in Supplementary Table 1.

Bland and Altman plots for the comparison between unattended office blood pressure and morning home blood pressure in a systolic and b diastolic measurements. Mean differences and ±2 SD between paired measurements are represented by full and dotted lines, respectively. The correlation coefficients between the difference and the mean were 0.48 (P < 0.0001) for systolic and 0.29 (P < 0.0001) for diastolic measurements

Bland and Altman plots for the comparison between conventionally measured attended office blood pressure and morning home blood pressure in a systolic and b diastolic measurements. Mean differences and ±2SD between paired measurements are represented by full and dotted lines, respectively. The correlation coefficients between the difference and the mean were 0.53 (P < 0.0001) for systolic and 0.32 (P < 0.0001) for diastolic measurements

Bland and Altman plots for the comparison between conventionally measured attended office blood pressure and unattended office blood pressure in a systolic and b diastolic measurements. Mean differences and ±2SD between paired measurements are represented by full and dotted lines, respectively. The correlation coefficients between the difference and the mean were 0.10 (P = 0.080) for systolic and 0.055 (P = 0.34) for diastolic measurements
A multiple regression analysis showed that the clinic sites consistently affected the differences in the office vs. HBP values for systolic (Table 3) and diastolic (Table 4) measurements. Basic characteristics, such as sex, age, and antihypertensive treatment, represented as defined daily doses, did not markedly affect the BP changes (P ≥ 0.055), except for age and sex concerning unattended BP vs. morning HBP and attended BP vs. unattended BP in systolic measurements (P ≤ 0.050). The results were essentially similar when we assessed evening HBP, as shown in Supplementary Tables 2 and 3. When we compared the difference in the measurements according to the prescribed timing of antihypertensive drugs, neither morning nor evening-to-bedtime prescription significantly affected the difference (P ≥ 0.21), except for the difference between attended office and morning HBP in the systolic measurements (Supplementary Table 4; 13.8 [19.0] mmHg among patients with a morning prescription vs. 9.0 [18.0] mmHg among those with an evening-to-bedtime prescription; P = 0.042)
Based on the morning HBP, 87 (28.2%) patients had uncontrolled hypertension ( ≥ 135/ ≥ 85 mmHg). Although the average morning HBP among patients with uncontrolled hypertension was 13.7 (7.1)/9.0 (8.3) mmHg higher than that among the other 228 controlled patients (P < 0.0001), the intensity of antihypertensive treatment, as represented by defined daily doses, was not significantly different (1.11 [0.83] vs. 0.94 [0.66] unit, P = 0.16). Furthermore, the uncontrolled and controlled patients did not demonstrate substantially different office BPs (unattended BP, 131.5 (14.2)/73.0 (13.5) vs. 127.9 (16.2)/69.5 (11.1) mmHg, P = 0.035/0.029; attended BP, 141.1 (16.6)/77.8 (14.7) vs. 138.6 (17.0)/73.5 (10.9) mmHg, P = 0.18/0.026). Similarly, 46 (15.3%) patients had uncontrolled hypertension based on their evening HBP, with a 17.6 (7.5)/13.2 (8.5) mmHg difference (P < 0.0001) compared with that of 254 controlled patients. However, the defined daily doses significantly differed between the uncontrolled and controlled patients (1.29 [0.92] vs. 0.93 [0.67] unit, P = 0.0089). The unattended office BP values in patients with uncontrolled and controlled evening hypertension were 133.8 (15.0)/74.8 (13.7) and 128.3 (15.9)/69.7 (11.5) mmHg, respectively (P = 0.022/0.012), and the corresponding attended BP values were 142.0 (17.6)/79.1 (15.5) and 139.2 (16.8)/74.0 (11.5) mmHg, respectively (P = 0.27/0.031).
Discussion
We performed the COSAC study to identify the clinical significance of AOBP officially used in SPRINT [11] —unattended office BP measured by automated devices—in comparison with HBP. Surprisingly, the unattended office BP and HBP provided essentially different information, based on our findings concerning the correlation coefficients and Bland and Altman plots. However, high correlations were noted between conventional attended BP and unattended BP despite fundamental differences, suggesting that the attendance of medical staff may raise patients’ BPs by an average of 11/4 mmHg. Unattended office BP might be a useful alternative to conventional attended office readings when considering the shift in the values, which might correspond to a sort of white-coat effect.
The unattended office BP measured by automated devices is also called the AOBP; however, there is some confusion regarding the definition of AOBP. AOBP was initially defined as multiple readings (three or more) [14] recorded automatically with the patient resting undisturbed in a quiet place in the absence of an observer [13, 14], but no antecedent rest time was defined. In SPRINT, the office BP was measured using the automated Omron HEM-907 cuff-oscillometric monitor [22] with a 5-min rest period before the first measurement and a 1-min interval between measurements. The SPRINT investigators later reported that 38 of the 88 SPRINT clinic sites complied with the definition of AOBP [13, 14], but staff attended measurements during the rest time and/or during the measurement at the other 50 sites, although the BPs measured during the trial were almost identical on cross-classification of the attended and unattended site groups. In the present study, fully conforming unattended office BP was measured as the unattended BP, and the attended office BP was measured using the same HEM-907 device but with measurements directly performed by study doctors according to the JSH 2014 guidelines [7], which recommend a few minutes of rest and 1- to 2-min intervals. Therefore, the key difference in the condition between the two in-office measurements is whether patients were alone in a separate room during the measurement. The unattended condition allows us to refine the BP information by eliminating an aspect of the white-coat effect incurred by being in the presence of medical staff.
In the present study, the mean difference between the attended and unattended office systolic BP was larger in women than in men (by 3.0 mmHg) as well as in nonsmokers than in smokers (by 4.9 mmHg). These factors have been reported to enhance the white-coat effect [26, 27], implying that the fundamental differences between attended and unattended office BP can be explained in part by the white-coat effect in a narrow sense. However, the unattended BP is measured at a clinic or in a screening setting, and the remaining portion of the white-coat effect—which can be called the clinic effect—still remains, as the circumstances are quite different from relaxing at home. Unattended BP measurements may therefore be a useful alternative to conventional office measurements [13, 28]. The currently observed high reproducibility of the three consecutive unattended BP readings in each patient (r ≥ 0.90) also supports the positive application of the measurement. However, the prognostic significance of the unattended BP is not equivalent to the out-of-office measurements because of the inability to entirely eliminate the clinic effect during in-office measurement.
The weak association between office BPs and HBPs observed in the present study remains a matter of debate. The majority of the study patients (96.4%) received antihypertensive drug treatment. In the Ohasama study, correlations between conventional BP and morning HBP were stronger among untreated participants (r = 0.55/0.50 in systolic/diastolic measurement) than among treated patients (r = 0.29/0.38) [29]. Though not fully addressed, antihypertensive drug treatment might reduce the reliability of office BP reading, resulting in the low correlations observed among treated patients. Moreover, the time intervals between office BPs vs. morning and evening HBPs varied, from at least 1 h to more than a half day. Such diverse time intervals might contribute to these lower correlations compared with the high correlations between attended and unattended office BP.
There were significant associations between the difference and the mean, i.e., correlation coefficients in the Bland and Altman plots, when office BPs vs. HBPs were assessed (P < 0.0001), indicating that there was a systemic proportional trend in each relationship. The 2017 ACC/AHA Guidelines [17] proposed that corresponding thresholds for hypertension based on conventional office and HBP measurement are at similar levels in the lower BP range (both 120/80 mmHg and 130/80 mmHg), but those in-office measurements were set higher than home measurements in the higher BP range (office BP corresponding to HBP; 140/90 to 135/85 mmHg, and 160/100 to 145/90 mmHg). Such discrepancies in the higher range and similarity in the lower range were based on previous reports for the distribution of office and HBP and outcome-driven operational thresholds by a participant-level meta-analysis [30]. However, no significant associations within the Bland and Altman plots were observed when unattended office BP and attended office BP were assessed (P ≥ 0.080), implying the similarity between unattended and attended office BP.
The consumption of office space and long measurement time reduce the feasibility of employing unattended BP measurements in clinical practice. The unattended BP reading used in the present study requires >10 min per person to obtain a few minutes for preparation and clean up, 5 min for resting before the first measurement, 3 min for resting across the intervals, and a further few minutes during cuff inflation and deflation based on the end-to-start principle, i.e., intervals are counted from the end of complete cuff deflation of the previous measurement to the start of the subsequent measurement (Table 5). Another device commonly used to measure the AOBP is the BpTRU [31] (BpTRU Medical Devices, Coquitlam, Canada; the company ceased operations in 2017), which performs six readings but averages the second to sixth readings as the default setting. Because the interval in BpTRU is based on the start-to-start principle, i.e., the interval is calculated from the start of the previous measurement to the start of the subsequent measurement (Table 5) [32], the five recorded readings with the BpTRU take as much time as three readings with other devices [32]. However, regardless of variations in measurement devices, unattended office BP measurements would not be feasible for application in routine outpatient settings. The overall length of consultation time with a general practitioner was reported to be 10.7 (6.7) min in 6 European countries [33] and 10.1 (5.3) min according to a recent surveillance of 22 Japanese diabetes physicians in central Tokyo [34]. If we introduce unattended BP measurement to all outpatients, then we should prepare at least one extra separate room with a person in charge to manage the unattended BP measurement under the condition that the cost of the measurement is not generally reimbursed. Furthermore, we could not provide any rationale to concentrate medical resources on unattended office BP measurement based on the current study.
In 2016, Filipovský et al. [20] reported on the relationship between HBP, unattended office BP measured by the BpTRU device, and conventional office BP measured by a mercury sphygmomanometer among 353 patients with hypertension (women 49.6%, mean age 61.4 years, under antihypertensive drug treatment 97.5%) at a single clinic site. Two or more antihypertensive drugs were prescribed for 82% of patients. Although patients rested 5 min before the first measurement, the mean unattended office BP values dropped from 135/79 mmHg at the second measurement to 129/77 mmHg at the 6th measurement. In contrast to the corresponding level in our study, the unattended office BP level was significantly lower than both the attended office BP determined by a mercury sphygmomanometer and the HBP by 15.0 (13.8)/8.0 (7.3) mmHg (n = 353) and 10.0 (17.9)/4.2 (8.3) mmHg (n = 114), respectively, with large individual differences. However, Bauer and colleagues reported that unattended office BP measured by the Omron HEM-907 device was significantly higher than the HBP by 8.7 (17.3)/1.7 (10.2) mmHg among 107 patients with hypertension (women 45.8%, mean age 69.5 years, under antihypertensive drug treatment 90.7%) from 4 clinic sites who had attended these offices for at least 1 year [19]. The HBP measurement conditions in those studies [19, 20] were similar to our own, as more than 90% of patients took antihypertensive drugs, and before visits to a clinic, patients measured their HBP for 7 days [19] or for 7 days with the exclusion of the first-day values (both morning and evening) [20] using their own HBP measurement devices. Of note, 33.6% of German patients used a wrist device [19], while all other patients [19, 20] as well as our own used an upper-arm cuff device. In addition to large differences in average BP between the unattended office BP and HBP among these studies, a large individual difference was commonly observed, supporting our finding that unattended BP could not be used as an alternative to HBP.
Although all clinic sites sufficiently followed the definition of AOBP [13, 14] for the measurement of unattended office BP, the environment of each room differed. For instance, unattended BP was measured in a treatment room for an intravenous drip partitioned by a curtain, in a bedroom for echocardiography with relaxing music, and in a fully isolated X-ray room at Miyakawa Clinic, Katsuya Clinic, and Yokohama Sotetsu bldg. Clinic, respectively. It is unclear how these different conditions directly affected the BP differences; nevertheless, it is likely that environmental factors play a major role in the differences, more so than the classic confounding factors shown in Tables 3 and 4. In addition to the aforementioned clinic effect, we should pay attention to differences in the measurement environment among clinics, even for the unattended measurement of office BP using automated devices.
The present study must be interpreted within the context of potential limitations. First, the cross-sectional design of the analysis limits causal inferences for the associations found. We were unable to assess the long-term trends or reproducibility in the differences between the various types of BP information. Second, the study patients used their own oscillometric devices that used different algorithms to compute systolic and diastolic BP. However, all devices for HBP measurements available in Japan have been manufactured in accordance with the JIS (Japanese Industrial Standard) and marketed under the certification of private third-party organizations commissioned by the Pharmaceutical and Medical Device Agency (PMDA). The current protocols for testing of the BP measurement accuracy of automated sphygmomanometers, used upon certification, include the International Protocol of the European Society of Hypertension (ESH-IP) 2010 [35] and the ISO81060-2 (2013) provided by the International Standardization Organization (ISO) [36]. Moreover, we included patients who measured their HBP regularly before the study, and all clinic staff took part in the Hypertension Objective Treatment Based on Measurement by Electrical Devices of Blood Pressure (HOMED-BP) trial that proved the feasibility of long-term antihypertensive treatment guided by HBP [37]. Instruction concerning the self-measurement of HBP and HBP-based clinical practice were therefore reliably performed in accordance with the recommendation by the JSH 2014 Guidelines [7]. Nevertheless, the diverse range of available HBP devices may introduce some imprecision to BP measurement at home, and the self-reporting of HBP measurement may increase the imprecision of data, though double-checked at the clinic sites and data management center. Third, the time periods of the three BP measurements were not consistent. As morning HBP was measured within one hour of waking and as evening HBP was measured just before going to bed, the actual measurement time of HBPs depended on the lifestyle of each patient. Office BPs were also measured in various time zones, although attended and unattended office BPs were sequentially captured. Finally, we did not collect data on the socioeconomic status of patients in the present study, which calls for further investigation.
In conclusion, although the average HBP and unattended office BP values were similar, the difference in the BP of each patient varied markedly. Indeed, the systolic home and unattended office BP showed almost no correlation, whereas the unattended office BP and conventional attended office BP were moderately to highly correlated, suggesting that the unattended BP can be interpreted to resemble the attended BP value but with more stable information [13, 28]; nevertheless, unattended office BP cannot replace HBP measurement. This latter finding is comparable to those in other studies reporting a low within-participant agreement between unattended office BP and ambulatory BP monitoring [13, 28, 38]. Furthermore, a recent meta-analysis [39] demonstrated significant heterogeneity (P < 0.001) between AOBP (in some studies, medical staff supervised patients during rest or BP recordings) and ambulatory BP monitoring among 19 studies. Even if the utility of AOBP is confirmed and its definition is established, some degree of white-coat effect, such as a clinic effect, will still affect such in-office readings, regardless of the direct presence of staff. HBP should therefore be prioritized, at least to a similar degree as ambulatory monitoring, in the diagnosis and treatment of hypertension [7, 40].
References
Asayama K, Satoh M, Kikuya M. Diurnal blood pressure changes. Hypertens Res. 2018;41:669–78.
Bobrie G, Chatellier G, Genes N, Clerson P, Vaur L, Vaisse B, et al. Cardiovascular prognosis of “masked hypertension” detected by blood pressure self-measurement in elderly treated hypertensive patients. J Am Med Assoc. 2004;291:1342–9.
Ohkubo T, Imai Y, Tsuji I, Nagai K, Kato J, Kikuchi N, et al. Home blood pressure measurement has a stronger predictive power for mortality than does screening blood pressure measurement: a population-based observation in Ohasama, Japan. J Hypertens. 1998;16:971–5.
Asayama K, Thijs L, Brguljan-Hitij J, Niiranen TJ, Hozawa A, Boggia J, et al. International Database of Home Blood Pressure in Relation to Cardiovascular Outcome investigators. Risk stratification by self-measured home blood pressure across categories of conventional blood pressure: a participant-level meta-analysis. PLoS Med. 2014;11:e1001591.
Kario K, Saito I, Kushiro T, Teramukai S, Ishikawa Y, Mori Y, et al. Home blood pressure and cardiovascular outcomes in patients during antihypertensive therapy: primary results of HONEST, a large-scale prospective, real-world observational study. Hypertension. 2014;64:989–96.
Head GA. The importance and prognostic value of nocturnal blood pressure assessments using inexpensive domestic devices. J Hypertens. 2017;35:463–5.
Shimamoto K, Ando K, Fujita T, Hasebe N, Higaki J, Horiuchi M, et al. Japanese Society of Hypertension Committee for Guidelines for the Management of Hypertension. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2014). Hypertens Res. 2014;37:253–390.
Myers MG. Automated office blood pressure-incorporating SPRINT into clinical practice. Am J Hypertens. 2017;30:8–11.
Myers MG, Kaczorowski J, Dolovich L, Tu K, Paterson JM. Cardiovascular risk in hypertension in relation to achieved blood pressure using automated office blood pressure measurement. Hypertension. 2016;68:866–72.
Ambrosius WT, Sink KM, Foy CG, Berlowitz DR, Cheung AK, Cushman WC, et al. The design and rationale of a multicenter clinical trial comparing two strategies for control of systolic blood pressure: the Systolic Blood Pressure Intervention Trial (SPRINT). Clin Trials. 2014;11:532–46. Group SSR
Wright JT Jr., Williamson JD, Whelton PK, Snyder JK, Sink KM, Rocco MV, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373:2103–16. SPRINT Research Group
Johnson KC, Whelton PK, Cushman WC, Cutler JA, Evans GW, Snyder JK, et al. Blood pressure measurement in SPRINT (Systolic Blood Pressure Intervention Trial). Hypertension. 2018;71:848–57. Group SR
Myers MG, Godwin M, Dawes M, Kiss A, Tobe SW, Grant FC, et al. Conventional versus automated measurement of blood pressure in primary care patients with systolic hypertension: randomised parallel design controlled trial. Br Med J. 2011;342:d286.
Stergiou GS, Doumas M, Kollias A, Papademetriou V. Important practice lessons from the SPRINT study beyond the blood pressure goal: all well known and now confirmed. J Am Soc Hypertens. 2016;10:613–7.
Colella TJF, Tahsinul A, Gatto H, Oh P, Myers MG. Antecedent rest may not be necessary for automated office blood pressure at lower treatment targets. J Clin Hypertens.;https://doi.org/10.1111/jch.13319. 2018
Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39:3021–104. ESC Scientific Document Group
Whelton PK, Carey RM, Aronow WS, Casey DE Jr., Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71:e13–e115.
Kobayashi M, Obara T, Ohkubo T, Fukunaga H, Satoh M, Metoki H, et al. Practice and awareness of physicians regarding casual-clinic blood pressure measurement in Japan. Hypertens Res. 2010;33:960–4.
Bauer F, Seibert FS, Rohn B, Bauer KAR, Rolshoven E, Babel N, et al. Attended versus unattended blood pressure measurement in a real life setting. Hypertension. 2018;71:243–9.
Filipovský J, Seidlerova J, Kratochvil Z, Karnosova P, Hronova M, Mayer O, et al. Automated compared to manual office blood pressure and to home blood pressure in hypertensive patients. Blood Press. 2016;25:228–34.
World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. J Am Med Assoc. 2013;310:2191–4.
White WB, Anwar YA. Evaluation of the overall efficacy of the Omron office digital blood pressure HEM-907 monitor in adults. Blood Press Monit. 2001;6:107–10.
World Health Organization. World Health Organization Collaborating Centre for Drug Statistics Methodology System of Defined Daily Doses. http://www.whocc.no/atc_ddd_index/; 2018. Accessed September 14, 2018.
Asayama K, Kikuya M, Schutte R, Thijs L, Hosaka M, Satoh M, et al. Home blood pressure variability as cardiovascular risk factor in the population of Ohasama. Hypertension. 2013;61:61–69.
Asayama K, Ohkubo T, Kikuya M, Obara T, Metoki H, Inoue R, et al. Prediction of stroke by home “morning” versus “evening” blood pressure values: the Ohasama study. Hypertension. 2006;48:737–43.
Verdecchia P, Palatini P, Schillaci G, Mormino P, Porcellati C, Pessina AC. Independent predictors of isolated clinic (‘white-coat’) hypertension. J Hypertens. 2001;19:1015–20.
Asayama K, Li Y, Franklin SS, Thijs L, O’Brien E, Staessen JA. Cardiovascular risk associated with white-coat hypertension: con side of the argument. Hypertension. 2017;70:676–82.
D’Sa L, Senaratne N, Woodcock-Smith J, Miles KM, Wilkinson IB, McEniery CM. Evaluation of the Omron HEM-907 automated blood pressure device: comparison with office and ambulatory blood pressure readings. Hypertens Res. 2019;42:52–58.
Yasui D, Asayama K, Takada N, Ohkubo T, Kikuya M, Hara A, et al. Evaluating home blood pressure in treated hypertensives in comparison with the referential value of casual screening of blood pressure: the Ohasama study. Blood Press Monit. 2012;17:89–95.
Niiranen TJ, Asayama K, Thijs L, Johansson JK, Ohkubo T, Kikuya M, et al. International Database of Home blood pressure in relation to Cardiovascular Outcome Investigators. Outcome-driven thresholds for home blood pressure measurement: international database of home blood pressure in relation to cardiovascular outcome. Hypertension. 2013;61:27–34.
Mattu GS, Heran BS, Wright JM. Overall accuracy of the BpTRU–an automated electronic blood pressure device. Blood Press Monit. 2004;9:47–52.
Myers MG, Colella TJF. Response to: Does AOBP require a 5-minute rest period to screen for hypertension? J Clin Hypertens (Greenwich). 2019;21:137.
Deveugele M, Derese A, van den Brink-Muinen A, Bensing J, De Maeseneer J. Consultation length in general practice: cross sectional study in six European countries. Br Med J. 2002;325:472.
Kabeya Y, Uchida J, Toyoda M, Katsuki T, Oikawa Y, Kato K, et al. Factors affecting consultation length in a Japanese diabetes practice. Diabetes Res Clin Pract. 2017;126:54–59.
O’Brien E, Atkins N, Stergiou G, Karpettas N, Parati G, Asmar R, et al. Working Group on Blood Pressure Monitoring of the European Society of Hypertension. European Society of Hypertension International Protocol revision 2010 for the validation of blood pressure measuring devices in adults. Blood Press Monit. 2010;15:23–38.
International Organization for Standardization. ISO 81060-2:2013, Non-invasive Sphygmomanometers—Part 2: Clinical Investigation of Automated Measurement Type. https://www.iso.org/standard/57977.html; 2013. Accessed April 17, 2018.
Asayama K, Ohkubo T, Metoki H, Obara T, Inoue R, Kikuya M, et al. Hypertension Objective Treatment Based on Measurement by Electrical Devices of Blood Pressure investigators. Cardiovascular outcomes in the first trial of antihypertensive therapy guided by self-measured home blood pressure. Hypertens Res. 2012;35:1102–10.
Drawz PE, Pajewski NM, Bates JT, Bello NA, Cushman WC, Dwyer JP, et al. Effect of intensive versus standard clinic-based hypertension management on ambulatory blood pressure: results from the SPRINT (Systolic Blood Pressure Intervention Trial) Ambulatory Blood Pressure Study. Hypertension. 2017;69:42–50.
Jegatheswaran J, Ruzicka M, Hiremath S, Edwards C. Are automated blood pressure monitors comparable to ambulatory blood pressure monitors? a systematic review and meta-analysis. Can J Cardiol. 2017;33:644–52.
Asayama K. Observational study and participant-level meta-analysis on antihypertensive drug treatment-related cardiovascular risk. Hypertens Res. 2017;40:856–60.
Acknowledgements
This study is supported solely by the Japanese Society of Hypertension.
COSAC study coordination and management
The COmparison of Self-measured home, Automated unattended office and Conventional attended office blood pressure (COSAC) study working group: T Ohkubo (Chair; Teikyo University), H Rakugi (Vice Chair; Osaka University), K Asayama (Teikyo University), S Ito (Tohoku University), S Ueda (University of Ryukyus), S Umemura (Yokohama Rosai Hospital), Y Ohya (University of Ryukyus), T Tsuchihashi (Yawata Hospital), K Kario (Jichi Medical University), K Miura (Shiga University of Medical Science). Clinical Investigators: H Mori (Yokohama Sotetsu bldg. Clinic), M Miyakawa (Miyakawa Clinic), T Katsuya (Katsuya Clinic). Secretariat and Data Management Committee: S Ueda (chair; University of Ryukyus), Y Ikehara (University of Ryukyus), K Une (University of Ryukyus). Statistical Analysis Committee: K Miura (chair; Shiga University), K Asayama. (Teikyo University).
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
KA, TO, and KK received the research support from Omron Healthcare. NH received honoraria and/or fees for the promotional materials from Astellas Pharma, Bayer Yakuhin, Mochida Pharmaceutical, Bristol-Myers Squibb, Nippon Boehringer Ingelheim, Takeda Pharmaceutical, Daiichi Sankyo, and Sumitomo Dainippon Pharma, and received research funding from Teijin Pharma, Mitsubishi Tanabe Pharma, Daiichi Sankyo, Sumitomo Dainippon Pharma, Shionogi, Astellas Pharma, Takeda Pharmaceutical, Otsuka Pharmaceutical, Asahikawa Rehabilitation Hospital, Genseikai Group, Kyokuhoukai Asahikawa Sanai Hospital, Enzankai Group, Kitasaito Hospital, Medical Corporation Kaiseikai Onishi Hospital, and Hokkaido Welfare Federation of Agricultural Cooperatives. Remaining authors declare no conflicts of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Asayama, K., Ohkubo, T., Rakugi, H. et al. Comparison of blood pressure values—self-measured at home, measured at an unattended office, and measured at a conventional attended office. Hypertens Res 42, 1726–1737 (2019). https://doi.org/10.1038/s41440-019-0287-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41440-019-0287-6
Keywords
This article is cited by
-
Quality is not an act, it is a habit—Aristotle
Hypertension Research (2023)
-
Improving measurement accuracy and feasibility to support long-term blood pressure management
Hypertension Research (2022)
-
Intensive blood pressure treatment in coronary artery disease: implications from the Systolic Blood Pressure Intervention Trial (SPRINT)
Journal of Human Hypertension (2022)
-
Home and office blood pressure: time to look at the individual patient
Hypertension Research (2021)
-
Comparison of Brachial Blood Pressure and Central Blood Pressure in Attended, Unattended, and Unattended Standing Situations
Hypertension Research (2021)
