
Abstract
Major depressive disorder (MDD) is a common, disabling, and heterogeneous condition that responds unpredictably to current treatments. We previously showed an association between depressive symptoms and plasma concentrations of two cholesterol precursors, desmosterol and 7-dehydrocholesterol (7DHC). Here, we measured total cholesterol and sterol concentrations with mass spectrometry in postmortem brain samples from depressed and control subjects. Mean (±SEM) desmosterol concentration was 8.9 ± 0.97 ng/mg in the depressed versus 10.7 ± 0.72 ng/mg in the control group. The mean of the posterior probability distribution for the difference in desmosterol concentration between the two groups was 2.36 (95% highest density interval [HDI] 0.59–4.17). Mean 7DHC concentrations, 12.5 ± 4.1 ng/mg in the depressed versus 5.4 ± 0.74 ng/mg in the control group, were unlikely to be different (95% HDI, [−1.37–0.34]). We found that presence of trazodone in the peri-mortem toxicology screen accounted for the observed difference in desmosterol concentrations. We also observed extremely high 7DHC levels in all 4 subjects who had taken trazodone. Trazodone has been recently found to inhibit 7-dehydrocholesterol reductase and alter sterol concentrations in rodents, cell culture, human fibroblasts, and blood. In this study, we demonstrate for the first time that trazodone alters human brain sterol composition. Given congenital deficiency of 7-dehydrocholesterol reductase results in Smith-Lemli-Opitz syndrome, our findings support the hypothesis that this commonly used medication may have previously unappreciated risks.
Similar content being viewed by others


Introduction
Major depressive disorder (MDD) is one of the top two causes of disability in the world [1,2,3]. Lifetime prevalence in North America is estimated to be ~15% [4]. Current treatments are only partially effective; about one third of patients with MDD fail to achieve remission with first or second line treatments [5]. One hypothesis that potentially explains the unpredictable response to treatment is the biological heterogeneity of the diagnostic construct [6, 7]. A promising and topical approach to this problem is the discovery and validation of depression biomarkers.
Cholesterol is essential for brain function [8]. Additionally, a putative association between low plasma cholesterol and depression or suicide has been suggested by several lines of investigation [9,10,11,12,13,14]. In light of these findings, we previously investigated associations between plasma sterols and depressive symptoms in a large, population-based cohort, as potential biomarkers [15]. We found that lower concentrations of the cholesterol precursor desmosterol and higher concentrations of another precursor, 7-dehydrocholesterol (7DHC), were predictive of moderate to severe depressive symptoms.
Since the publication of our study, it has become increasingly apparent that several psychotropic medications interfere with cholesterol synthesis [16,17,18,19,20,21]. In the current study, we tested the hypothesis that desmosterol and 7DHC would be altered in postmortem brains from people with depression and these changes may be explained by psychotropic medication use.
This is, to our knowledge, the first study to investigate cholesterol precursors and other related sterols in a comprehensive manner in postmortem brains. We focused on two brain regions: the prefrontal cortex (PFC) and the cerebellum. PFC was chosen given the well-known implications in the neurobiology of MDD [22,23,24,25,26,27] and as the main target of emerging neuro-stimulation treatments. Cerebellum has also been implicated as a part of brain networks disrupted in MDD [28,29,30] but is anatomically distinct from the PFC.
Materials, subjects and methods
Study population
Frozen, pulverized postmortem human brain samples and de-identified clinical data were obtained from Dallas Brain Collection. The prefrontal cortex (PFC) samples were from Brodmann area 9 in the dorsolateral PFC. Cerebellar (CBL) samples were dissected from the cerebellar cortex, avoiding the vermis. MDD diagnoses were made using all available information, including review of medical records and phone calls to caregivers when necessary. These data were presented to at least two (usually 3–4) experienced clinicians and diagnoses were made according to Diagnostic and Statistical Manual criteria. Samples from subjects diagnosed with MDD were matched to samples from subjects with no diagnosis of depression based on age and postmortem interval. Medication use data was obtained from medical charts and also from peri-mortem toxicology reports. Subject characteristics are summarized in Table 1. Sample size was estimated based on the effect size we had observed in plasma samples in a previous study [15]. Collection of postmortem brains by the Dallas Brain Collection was approved by UT Southwestern Institutional Review Board. The investigators were blinded to sample group assignments during mass spectrometry and initial analysis steps. The Dallas Brain Collection kept the master file with sample group assignments. The blind was broken after primary analyses were completed and some secondary analyses done un-blinded.
Sterol concentration measurements from postmortem brain tissue
Samples were processed and analyzed as described in McDonald et al. [31]. Briefly, samples were rapidly thawed and hydrolyzed to generate a pool of free sterols, extracted with a modified Bligh/Dyer 2-phase extraction, and purified with solid-phase extraction. Sterols were analyzed using LC-MS as previously described [31]. In total, we measured concentrations of 19 sterols, including total cholesterol.
Statistical analyses
To examine whether healthy controls and depressed subjects differ on their mean sterol levels, independent samples t-tests with robust Bayesian estimation were conducted using the BEST package [32] in R version 3.6.3. Differences in mean sterol concentrations were tested for 7DHC and desmosterol using brain tissues from the prefrontal cortex (PFC) and cerebellum (CBL). As opposed to a frequentist t-test, the robust Bayesian estimation can accommodate the presence of outliers. Model results reveal the relative credibility for each possible parameter value in the form of a posterior probability distribution. The 95% highest density interval (HDI) was calculated using the default MCMC parameters with 1000 burn-in steps. Convergence was reached for all parameters as measured by pre-defined criteria of Brooks-Gelman-Rubin scale reduction factor <1.1.
In a Bayesian framework, hypothesis testing is comparative and the likelihood of observed data is considered under both the null and alternative. In contrast, frequentist statistics do not explicitly calculate the probabilities of the alternative hypothesis and numerous drawbacks of using frequentist statistics have been extensively discussed in the literature [33, 34].
The choice to use a Bayesian framework for the present study was two-fold. First, prior work has shown that blood sterol concentrations are significantly related to depressive symptoms [15]. The use of a Bayesian method enables incorporation of prior knowledge in our present analysis. Second, Bayesian estimation allows one to express the level of uncertainty in the results using a 95% credibility interval (CI) around the most likely parameter values.
Results and discussion
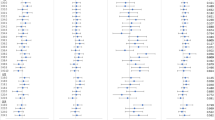
Demographic variables of subjects and postmortem tissue quality markers are summarized in Table 1. Controls were age matched to depressed samples. Tissue quality markers were similar in both groups. Concentrations of sterols were measured in PFC and cerebellum samples from 20 depressed subjects and 20 controls (80 samples in total). Total cholesterol was also measured in 79 of the samples (one cerebellum sample from the control group did not have enough material for this measurement). Concentrations of 19 sterols in depressed and control samples are summarized in Fig. 1. There was no significant association between gender and sterol levels.

The log10 of sterol concentrations for each individual is shown with the color scale. The samples were clustered and visualized using pheatmap package in R. CTRL control; DEP depressed.
Total cholesterol abundance was nominally lower in the depressed group both in the PFC and the cerebellum but unlikely to be different (95% highest density interval [HDI] of mean difference, −0.75–2.24 μg/mg) (Fig. 2A; Table 2). Measurements from PFC and cerebellum samples had similar mean values for cholesterol, desmosterol, and 7DHC in both groups (Fig. 2B, C; Table 2). Incidentally, we found lower 24S-hydroxycholesterol concentrations in the cerebellum (Fig. S4). Desmosterol and 7DHC abundance correlated weakly at the level of individual subjects between the two brain regions (Fig. S1; biweight midcorrelation coefficient 0.19 and 0.35, respectively). Therefore, we pooled PFC and cerebellum measurements for further analysis.

A Cholesterol (μg per mg tissue), (B) desmosterol (ng per mg tissue), and (C) 7-dehydrocholesterol (ng per mg tissue) measurements were made in two brain regions: cerebellum (CBL) and pre-frontal cortex (PFC), from control (CTRL) and depressed (DEP) subjects. The thick lines correspond to the group and brain region specific mean sterol concentrations. D Posterior probability distribution of the difference in mean desmosterol concentrations between control (μctrl) and depressed (μdep) groups are plotted; the values are in ng/mg tissue. The mean of the distribution is 2.4 ng/mg. Dark horizontal line above the axis indicates the 95% Highest Density Interval (0.59–4.17 ng/mg). Green dotted line indicates the probability that the difference in the means is less than or equal to zero (0.006). E Posterior probability distribution of the difference in mean 7DHC concentrations between control and depressed groups is plotted as in (A). The mean of the distribution is 0.52 ng/mg (95% Highest Density Interval −0.34–1.38 ng/mg). The probability that the difference in the means is less than or equal to zero is 0.116.
We hypothesized that desmosterol concentrations would be lower in depressed samples compared to controls based on our previous finding of lower plasma desmosterol levels in depressed subjects in an independent sample. Here, we found a mean (±SEM) desmosterol concentration of 8.9 ± 0.97 ng/mg in the depressed versus 10.7 ± 0.72 ng/mg in the control group (Table 2). We used an independent samples t-test with robust Bayesian estimation and found that the mean of the posterior probability distribution for the difference in desmosterol concentration between the two groups was 2.36 ng/mg (95% highest density interval [HDI] 0.59–4.17 ng/mg) (Fig. 2D). The probability that the difference in the means is less than or equal to zero was 0.006 (Fig. 2D). Sensitivity analyses using only PFC or only cerebellum measurements revealed similar results (Fig. S2). We also found the six highest brain 7DHC levels (from 4 individual subjects) in the depressed group (Fig. 2C). This results in a higher mean 7DHC concentration in the depressed group with a large variance (12.5 ± 4.1 ng/mg in the depressed versus 5.4 ± 0.74 ng/mg in the control group; Table 2). However, using independent samples t-tests with robust Bayesian estimation we found that the mean 7DHC concentrations between the two groups (depressed minus control) is unlikely to be different (95% HDI, [−1.37–0.34]) (Figs. 2E; S3).
Next, we investigated whether the differences in brain sterol concentrations could be explained by medication use, based on recent reports of inhibition of key cholesterol synthesis enzymes by psychotropic medications [17,18,19, 35, 36]. We considered data from both medication use history and toxicology reports, and identified morphine, ethanol, trazodone, escitalopram, alprazolam, diphenhydramine, hydrocodone, aspirin, atropine, insulin, and lisinopril as the only medications used by or found in >2 subjects. Only trazodone was significantly correlated with low desmosterol and high 7DHC concentrations (Spearman rho −0.38, and 0.51 with corresponding p values of 0.0005 and 0.0000012, respectively). As shown in Fig. 3, trazodone use explains all the difference in desmosterol and 7DHC levels between the groups. Specifically, all 4 subjects with extremely high 7DHC levels had taken trazodone; desmosterol levels in depressed subjects who did not take trazodone were indistinguishable from levels in the control group (Wilcoxon rank sum test p = 0.122); depressed subjects who took trazodone had significantly lower desmosterol levels compared to others (Wilcoxon rank sum test p = 0.009). Last, we found trazodone use also correlated with increased 7-dehydrodesmosterol and 8(9)-dehydrocholesterol concentrations (Spearman rho 0.48, and 0.43 with corresponding p values of 0.0000063 and 0.00007, respectively). Taken together, trazodone alters brain sterol composition.

Subjects are separated into two groups based on detection of trazodone in a peri-mortem toxicology screen. The distribution of (A) 7-dehydrocholesterol (7-DHC) and (B) desmosterol is depicted as a boxplot. The median is indicated with the thick horizontal black line and the box correspond to the interquartile range. Individual measurements that are outside 1.5 times the interquartile range are depicted with separate dots.
Our prior work has shown that plasma levels of two cholesterol precursors, desmosterol and 7DHC, can be used to predict depressive symptoms in a population. This finding suggested plasma sterol levels may be depression biomarkers. One of the major limitations of our previous study was that the correlation between plasma and brain levels of these sterols was unknown. Additionally, we were not able to analyze potential confounding by medication use. The current study addresses both limitations. Here, we show that desmosterol and 7DHC abundances have the same direction of difference in brains from clinically depressed subjects as they had in the plasma of subjects with moderate to severe depressive symptoms in a different cohort. However, this difference seems to be wholly explained by the use of trazodone, a sedating antidepressant.
Cholesterol is indispensable for brain development and function [37]. Changes in brain cholesterol concentrations have long been associated with suicide and depression. More recently, four psychotropic medications, aripiprazole, cariprazine, haloperidol, and trazodone have been shown to be inhibitors of 7-dehydrocholesterol reductase, leading to increased 7DHC and reduced desmosterol levels in cell culture, rodents (including in utero models), human dermal fibroblasts, and human blood [17, 19, 20, 35, 36, 38]. In these models, the magnitude of 7-DHC elevation was comparable to levels seen in Smith-Lemli-Opitz syndrome, a severe congenital syndrome caused by mutations in the DHCR7 gene encoding 7-dehydrocholesterol reductase. Recent reviews have raised caution about the use of these medications in pregnancy and in carriers of DHCR7 mutations [17]. Our study, to the best of our knowledge, is the first demonstration of sterol abnormalities in human brains due to trazodone use. This is a previously unappreciated potential risk of this commonly used medication. The current package label for trazodone (Desyrel®) (https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/071196s062lbl.pdf) contains sparse information about pregnancy implications and no warnings about potential effects on cholesterol synthesis in utero, highlighting the need for increased pharmacovigilance in this area.
References
Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B. Depression, chronic diseases, and decrements in health: results from the World Health Surveys. Lancet. 2007;370:851–8.
Ferrari AJ, Charlson FJ, Norman RE, Flaxman AD, Patten SB, Vos T, et al. The epidemiological modelling of major depressive disorder: application for the Global Burden of Disease Study 2010. PLoS ONE. 2013;8:e69637.
Vos T, Barber RM, Bell B, Bertozzi-Villa A, Biryukov S, Bolliger I, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386:743–800.
Kessler RC. The costs of depression. Psychiatr Clin North Am. 2012;35:1–14.
Rush AJ, Trivedi MH, Wisniewski SR, Stewart JW, Nierenberg AA, Thase ME, et al. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression. N. Engl J Med. 2006;354:1231–42.
Hasler G. Pathophysiology of depression: do we have any solid evidence of interest to clinicians? World Psychiatry. 2010;9:155–61.
Pinto JV, Moulin TC, Amaral OB. On the transdiagnostic nature of peripheral biomarkers in major psychiatric disorders: a systematic review. Neurosci Biobehav Rev. 2017;83:97–108.
Korade Z, Kenworthy AK. Lipid rafts, cholesterol, and the brain. Neuropharmacology. 2008;55:1265–73.
Boscarino JA, Erlich PM, Hoffman SN. Low serum cholesterol and external-cause mortality: potential implications for research and surveillance. J Psychiatr Res. 2009;43:848–54.
Fiedorowicz JG, Coryell WH. Cholesterol and suicide attempts: a prospective study of depressed inpatients. Psychiatry Res. 2007;152:11–20.
Morgan RE, Palinkas LA, Barrett-Connor EL, Wingard DL. Plasma cholesterol and depressive symptoms in older men. Lancet. 1993;341:75–9.
Partonen T, Haukka J, Virtamo J, Taylor PR, Lönnqvist J. Association of low serum total cholesterol with major depression and suicide. Br J Psychiatry. 1999;175:259–62.
Steegmans PH, Hoes AW, Bak AA, van der Does E, Grobbee DE. Higher prevalence of depressive symptoms in middle-aged men with low serum cholesterol levels. Psychosom Med. 2000;62:205–11.
Lalovic A, Levy E, Luheshi G, Canetti L, Grenier E, Sequeira A, et al. Cholesterol content in brains of suicide completers. Int J Neuropsychopharmacol. 2007;10:159–66.
Cenik B, Cenik C, Snyder MP, Brown ES. Plasma sterols and depressive symptom severity in a population-based cohort. PLoS ONE. 2017;12:e0184382.
Genaro-Mattos TC, Klingelsmith KB, Allen LB, Anderson A, Tallman KA, Porter NA, et al. Sterol Biosynthesis Inhibition in pregnant women taking prescription medications. ACS Pharm Transl Sci. 2021;4:848–57.
Korade Z, Heffer M, Mirnics K. Medication effects on developmental sterol biosynthesis. Mol Psychiat. 2021. https://doi.org/10.1038/s41380-021-01074-5.
Tallman KA, Allen LB, Klingelsmith KB, Anderson A, Genaro-Mattos TC, Mirnics K, et al. Prescription medications alter neuronal and glial cholesterol synthesis. ACS Chem Neurosci. 2021;12:735–45.
Korade Z, Allen LB, Anderson A, Tallman KA, Genaro-Mattos TC, Porter NA, et al. Trazodone effects on developing brain. Transl Psychiatry. 2021;11:85.
Genaro-Mattos TC, Anderson A, Allen LB, Tallman KA, Porter NA, Korade Z, et al. Maternal cariprazine exposure inhibits embryonic and postnatal brain cholesterol biosynthesis. Mol Psychiatry. 2020;25:2685–94.
Genaro-Mattos TC, Anderson A, Allen LB, Korade Z, Mirnics K. Cholesterol biosynthesis and uptake in developing neurons. ACS Chem Neurosci. 2019;10:3671–81.
Light SN, Heller AS, Johnstone T, Kolden GG, Peterson MJ, Kalin NH, et al. Reduced right ventrolateral prefrontal cortex activity while inhibiting positive affect is associated with improvement in hedonic capacity after 8 weeks of antidepressant treatment in major depressive disorder. Biol Psychiatry. 2011;70:962–8.
Merkl A, Schubert F, Quante A, Luborzewski A, Brakemeier E-L, Grimm S, et al. Abnormal cingulate and prefrontal cortical neurochemistry in major depression after electroconvulsive therapy. Biol Psychiatry. 2011;69:772–9.
Kang HJ, Adams DH, Simen A, Simen BB, Rajkowska G, Stockmeier CA, et al. Gene expression profiling in postmortem prefrontal cortex of major depressive disorder. J Neurosci. 2007;27:13329–40.
Grimm S, Beck J, Schuepbach D, Hell D, Boesiger P, Bermpohl F, et al. Imbalance between left and right dorsolateral prefrontal cortex in major depression is linked to negative emotional judgment: An fMRI Study in Severe Major Depressive Disorder. Biol Psychiatry. 2008;63:369–76.
Kaiser RH, Whitfield-Gabrieli S, Dillon DG, Goer F, Beltzer M, Minkel J, et al. Dynamic Resting-State Functional Connectivity in Major Depression. Neuropsychopharmacology. 2016;41:1822–30.
Hamilton JP, Etkin A, Furman DJ, Lemus MG, Johnson RF, Gotlib IH. Functional neuroimaging of major depressive disorder: a meta-analysis and new integration of baseline activation and neural response data. AJP. 2012;169:693–703.
Phillips JR, Hewedi DH, Eissa AM, Moustafa AA. The cerebellum and psychiatric disorders. Front Public Health. 2015;3:66.
Schutter DJLG. A cerebellar framework for predictive coding and homeostatic regulation in depressive disorder. Cerebellum. 2016;15:30–3.
Depping MS, Wolf ND, Vasic N, Sambataro F, Hirjak D, Thomann PA, et al. Abnormal cerebellar volume in acute and remitted major depression. Prog Neuropsychopharmacol Biol Psychiatry. 2016;71:97–102.
McDonald JG, Smith DD, Stiles AR, Russell DW. A comprehensive method for extraction and quantitative analysis of sterols and secosteroids from human plasma. J Lipid Res. 2012;53:1399–409.
Kruschke JK. Bayesian estimation supersedes the t test. J Exp Psychol Gen. 2013;142:573–603.
Rouder JN, Speckman PL, Sun D, Morey RD, Iverson G. Bayesian t tests for accepting and rejecting the null hypothesis. Psychon Bull Rev. 2009;16:225–37.
Wagenmakers E-J, Marsman M, Jamil T, Ly A, Verhagen J, Love J, et al. Bayesian inference for psychology. Part I: Theoretical advantages and practical ramifications. Psychon Bull Rev. 2018;25:35–57.
Genaro-Mattos TC, Allen LB, Anderson A, Tallman KA, Porter NA, Korade Z, et al. Maternal aripiprazole exposure interacts with 7-dehydrocholesterol reductase mutations and alters embryonic neurodevelopment. Mol Psychiatry. 2019;24:491–500.
Korade Ž, Liu W, Warren EB, Armstrong K, Porter NA, Konradi C. Effect of psychotropic drug treatment on sterol metabolism. Schizophr Res. 2017;187:74–81.
Dietschy JM, Turley SD. Thematic review series: brain Lipids. Cholesterol metabolism in the central nervous system during early development and in the mature animal. J Lipid Res. 2004;45:1375–97.
Hall P, Michels V, Gavrilov D, Matern D, Oglesbee D, Raymond K, et al. Aripiprazole and trazodone cause elevations of 7-dehydrocholesterol in the absence of Smith–Lemli–Opitz Syndrome. Mol Genet Metab. 2013;110:176–8.
Acknowledgements
We are grateful to Bercin K. Cenik and Joyce Repa for help with sample preparation and Kelly Gleason for dissection of the brains.
Funding
BC is supported by NARSAD Young Investigator Grant (Grant ID: 26099) from Brain & Behavior Research Foundation; JGM is supported in part by NIH program Project Grant to Molecular Genetics (HL20948); CC is supported in part by the National Institutes of Health (CA204522), Cancer Prevention and Research Institute of Texas (RR180042), and Welch Foundation (F-2027-20200401). ESB is supported in part by the NIH and the Stanley Medical Research Institute. The funding bodies had no role in the design of the study or collection, analysis, and interpretation of data, or in writing the manuscript.
Author information
Authors and Affiliations
Contributions
BC and ESB conceptualized the study. BMT and JGM performed mass spectrometry experiments. BC helped with sample preparation. BC, JMP, and CC analyzed data. CAT provided human brain samples. CC and ESB supervised data analysis. BC and CC wrote the manuscript. All authors read the manuscript and made comments.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cenik, B., Palka, J.M., Thompson, B.M. et al. Desmosterol and 7-dehydrocholesterol concentrations in post mortem brains of depressed people: The role of trazodone. Transl Psychiatry 12, 139 (2022). https://doi.org/10.1038/s41398-022-01903-3
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41398-022-01903-3
