
Abstract
Background/Objectives:
Vitamin D insufficiency in cystic fibrosis is common. Vitamin D3 is currently preferred over D2. We aimed to study the efficacy of vitamin D2 and D3 at increasing serum 25-hydroxyvitamin D (s25OHD) concentrations and their effect on respiratory health in cystic fibrosis.
Subjects/Methods:
Sixteen CF patients were randomized to receive vitamin D2 or D3 or to serve as controls. The starting dose of 5000 IU (<16 years old) or 7143 IU/day (⩾16 years old) was further individually adjusted. Three months of intervention were followed by two of washout (ClinicalTrials.gov NCT01321905).
Results:
To increase s25OHD, the mean daily dose of vitamin D2 and D3 had to be increased up to 15650 and 8184 IU, respectively. The combined group of vitamin D2 and D3 treated patients decreased plasma IL-8 (P<0.05). Patients provided vitamin D3 improved FVC at the end of the trial (P<0.05). Change in s25OHD was positively correlated with changes in the adult Quality-of-Life respiratory score at the end of supplementation (P=0.006, r=0.90), and with changes in FEV1 (P=0.042, r=0.62) and FVC (P=0.036, r=0.63) at one month of washout.
Conclusions:
Vitamin D supplementation may contribute to reduced inflammation and improved lung function in CF.
Similar content being viewed by others


Introduction
In cystic fibrosis (CF), the major cause of morbidity and mortality is progressive lung disease driven by recurring acute airway infections and chronic bacterial lung colonization.1 Vitamin D insufficiency is common in CF despite vitamin D supplementation.2, 3 In addition to its importance for bone health, vitamin D acts as a potent immune modulatory agent with complex effects.4, 5 In CF, vitamin D concentrations have been associated with lung function,2, 6 annual number of pulmonary exacerbations7 and with total serum IgG levels.2
The current recommendations for vitamin D supplementation in CF were designed with focus on bone health. Because of its higher efficiency at increasing serum 25-hydroxyvitamin D (s25OHD), vitamin D3 (D3) is currently preferred over vitamin D2 (D2). Most of the recommendations are consensus-based due to lack of knowledge on benefit–safety ratio.8, 9
In the present pilot study, the primary goal was to establish an efficient once-daily dosing strategy and to investigate the efficacy of D2 and D3 at increasing s25OHD concentrations. The secondary goal was to explore the effect of the interventions on cytokine concentrations and respiratory health.
Subjects and methods
Trial design
The study was approved by the Regional Ethical Review Board in Stockholm, Sweden (2009/1723-31/1). Patients were enrolled between 9 April 9 2010 and 16 May 2011. The trial was conducted in accordance with the Helsinki Declaration of 1975 as revised in 1983. Sixteen CF patients were randomized to receive either D2 or D3 or to become a control (Supplementary Figure E1). Patients randomized to the intervention arms received a starting dose of 35 000 IU (if <16 years old) or 50 000 IU (if ⩾16 years old) D2 or D3 per week. The weekly dose was given as seven once-daily doses. The control group did not receive any extra vitamin D. All study patients continued their ordinary vitamin supplementation unchanged. The study was open-label and consisted of 3 months of supplementation followed by 2 months of washout. Thirteen patients completed the trial and were analyzed. The primary outcome of the trial was total s25OHD (tot-s25OHD) at 3 months visit. The goal of the supplementation was to reach tot-s25OHD>100 nmol/l (ClinicalTrials.gov Identifier: NCT01321905). More information is available in the online Supplementary Information.
Results
There were no significant differences in the baseline characteristics between the study arms (Supplementary Table E1). One patient in each study arm left the trial shortly after completing the baseline visit. The 13 patients completing the study were included in the analyses (Supplementary Table E2). For some analyses, patients randomized to receive D2 or D3 were pooled into one group (Supplementary Table E3). The adherence with vitamin D treatment was overall very good (median score 7/7; lowest score 5/7).
There were no differences in tot-s25OHD or free s25OHD (free-s25OHD) levels between the groups at baseline. The control group did neither change their tot-s25OHD nor free-s25OHD throughout the study. At the end of supplementation, the mean (s.d.) ingested total D2 and D3 dose was 771.173 (296.870) and 598.066 (132.126) IU, respectively. At this time point, the D3 group had higher tot-s25OHD than the controls had (P=0.019), which was not the case for the D2 group (Table 1, Figure 1a). In line with this, all patients in both intervention arms had tot-s25OHD>75 nmol/l at the end of supplementation. None of the patients allocated to the D2 group reached the goal of 100 nmol/l, whereas two out of five D3 group patients reached this goal. Posthoc power calculation showed that five patients are needed to find a difference of 25 units in tot-s25OHD (end of intervention compared with baseline) in 70% of cases. In the combined group of all patients receiving vitamin D, free-s25OHD dropped during washout, and was significantly lower than that at baseline (Figure 1b). Tot-s25OHD at the end of supplementation correlated closely with total vitamin D dose (Figure 1c).

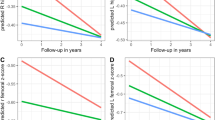
Immunological and clinical impact of vitamin D supplementation. (a) Tot-s25OHD levels in control group, D2 group and D3 group. There was no change in tot-s25OHD levels in control patients throughout the study, whereas there was a tendency for increase in tot-s25OHD in D2 group at the end of supplementation (P=0.106). D3 group had increased tot-s25OHD levels at 8 weeks of supplementation and at the end of supplementation (P<0.05). (b) Free-s25OHD levels in control group, D2 group and D3 group. There was no change in free-s25OHD levels in control and D2 patients throughout the study, whereas D3 group had increased free-s25OHD levels at 8 weeks of supplementation and at the end of supplementation (P<0.05). (c) Total vitamin D dose ingested at the end of supplementation versus tot-s25OHD in all patients (P=0.03; r=0.76). (d) The combined group of patients receiving D2 and D3 had decreased IL-8 concentration in circulation at the end of supplementation and at 1 month and 2 months of washout (P<0.05). (e) Change from baseline in free-s25OHD versus change from baseline in IL-1β at the end of the study in all patients (P=0.004; r=−0.95). (f) Change from baseline in free-s25OHD versus change from baseline in circulating neutrophil count at the end of supplementation in all patients (P=0.017; r=−0.80). (g) Change from baseline in free-s25OHD versus change from baseline in QoL-respiratory score at the end of supplementation (P=0.006, r=0.90). (h) Change from baseline in tot-s25OHD versus change from baseline in FEV1 at 1 month of washout (P=0.042, r=0.62). (i) Change from baseline in tot-s25OHD versus change from baseline in FVC at 1 month of washout (P=0.036, r=0.63).
Patients randomized to receive D2 or D3 showed decreased levels of IL-8 in plasma at the end of supplementation. Moreover, IL-8 remained decreased at both 1 month and 2 months of washout, as compared with baseline (Figure 1d). At the end of the study, the change in IL-1β from baseline was negatively correlated with the change in free-s25OHD (Figure 1e). At the end of supplementation, the change from baseline in free-s25OHD was inversely correlated with changes in neutrophil count (Figure 1f). At 1 month of washout, the change in neutrophil counts continued to be inversely correlated with the change in tot- and free-s25OHD. Notably, the changes in neutrophil counts followed the changes in free-s25OHD more closely than changes in tot-s25OHD (Supplementary Figures E2–E3).
At baseline, tot-s25OHD correlated positively with the adult quality-of-life (QoL)-respiratory score (Supplementary Figure E4). Moreover, the change from baseline in free-s25OHD at the end of supplementation correlated positively with change in the adult QoL-respiratory score (Figure 1g). At baseline, tot-s25OHD correlated positively with forced expiratory volume in 1 s (FEV1), FEV1 expressed as percentage FVC (FEV%) and forced expiratory flow at 75% of FVC (FEF75%) (Supplementary Figures E5–E7). Patients allocated to serve as controls had a tendency to decrease their forced expiratory flow at 25% of FVC (FEF25%) at the 2- and 5-month visits, compared with baseline (Table 1). Patients allocated to the D3 arm improved their forced vital capacity (FVC) at the last study visit compared with baseline, whereas those receiving D2 did not change their lung function throughout the study (Table 1). At 1 month of washout, the change in tot-s25OHD from baseline was positively correlated with changes in FEV1 and FVC (Figures 1h–i).
Summary
This pilot trial suggests that high doses are needed to improve vitamin D status in CF patients. Vitamin D supplementation may positively affect the immune system in patients with CF, which might eventually lead to better respiratory function. The results also suggest the possibility that free-s25OHD may be a better correlate of the clinical impact of vitamin D treatment, as compared with the currently used tot-s25OHD. Larger long-term placebo-controlled studies are needed to test the new hypotheses generated by this pilot trial.
References
Bush A, Bilton D, Hodson M (eds). Hodson and Geddes' Cystic Fibrosis, 4th edn. CRC Press: London, UK, 2015.
Pincikova T, Nilsson K, Moen IE, Karpati F, Fluge G, Hollsing A et al. Inverse relation between vitamin D and serum total immunoglobulin G in the Scandinavian Cystic Fibrosis Nutritional Study. Eur J Clin Nutr 2011; 65: 102–109.
Norton L, Page S, Sheehan M, Mazurak V, Brunet-Wood K, Larsen B . Prevalence of inadequate vitamin d status and associated factors in children with cystic fibrosis. Nutr Clin Pract 2015; 30: 111–116.
Bouillon R, Carmeliet G, Verlinden L, van Etten E, Verstuyf A, Luderer HF et al. Vitamin D and human health: lessons from vitamin D receptor null mice. Endocr Rev 2008; 29: 726–776.
Di Rosa M, Malaguarnera M, Nicoletti F, Malaguarnera L . Vitamin D3: a helpful immuno-modulator. Immunology 2011; 134: 123–139.
Sexauer WP, Hadeh A, Ohman-Strickland PA, Zanni RL, Varlotta L, Holsclaw D et al. Vitamin D deficiency is associated with pulmonary dysfunction in cystic fibrosis. J Cyst Fibros 2015; 14: 497–506.
Vanstone MB, Egan ME, Zhang JH, Carpenter TO . Association between serum 25-hydroxyvitamin D level and pulmonary exacerbations in cystic fibrosis. Pediatr Pulmonol 2015; 50: 441–446.
Sermet-Gaudelus I, Bianchi ML, Garabedian M, Aris RM, Morton A, Hardin DS et al. European cystic fibrosis bone mineralisation guidelines. J Cyst Fibros 2011; 10: S16–S23.
Tangpricha V, Kelly A, Stephenson A, Maguiness K, Enders J, Robinson KA et al. An update on the screening, diagnosis, management, and treatment of vitamin D deficiency in individuals with cystic fibrosis: evidence-based recommendations from the Cystic Fibrosis Foundation. J Clin Endocrinol Metab 2012; 97: 1082–1093.
Acknowledgements
This study was supported by the Karolinska Institutet, the Stockholm County Council, Stiftelsen Samariten, Erica Lederhausens Minnesstiftelse, the Swedish Cystic Fibrosis Association, Stiftelsen Frimurare Barnhuset i Stockholm, the Swedish Research Council, the Heart and Lung Foundation and the Swedish Cancer Society. DPP is the recipient of a postdoctoral fellowship from the Canadian Institutes of Health Research. The study was registered at ClinicalTrials.gov as NCT01321905.
Author contributions
TP and LH designed the study and delineated hypotheses. TP collected the data, analyzed and interpreted them, with contribution of LH, DPP, MFT and JS. TP wrote the article, with contributions from the LH, JS, DPP and MFT; TP and LH had primary responsibility for final content. All authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Data from the manuscript have been presented at a meeting: 36th European Cystic Fibrosis Conference, Lisbon, Portugal, 14 June 2013, Abstract WS16.3.
Supplementary Information accompanies this paper on European Journal of Clinical Nutrition website
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Pincikova, T., Paquin-Proulx, D., Sandberg, J. et al. Clinical impact of vitamin D treatment in cystic fibrosis: a pilot randomized, controlled trial. Eur J Clin Nutr 71, 203–205 (2017). https://doi.org/10.1038/ejcn.2016.259
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ejcn.2016.259
This article is cited by
-
Vitamin D deficiency in patients with cystic fibrosis: a systematic review and meta-analysis
Journal of Health, Population and Nutrition (2024)
-
Recent advances in vitamin D implications in chronic respiratory diseases
Respiratory Research (2022)
-
Targeting Vitamin D Deficiency to Limit Exacerbations in Respiratory Diseases: Utopia or Strategy With Potential?
Calcified Tissue International (2020)
-
Vitamin D inhibits pro-inflammatory cytokines in the airways of cystic fibrosis patients infected by Pseudomonas aeruginosa- pilot study
Italian Journal of Pediatrics (2019)
-
Ancestry-specific polygenic scores and SNP heritability of 25(OH)D in African- and European-ancestry populations
Human Genetics (2019)
