
Abstract
Study design: Comparison of five different exercise testing protocols with different speeds on a treadmill with seven wheelchair athletes.
Objective: To determine which speed and duration in an exercise protocol is best to test wheelchair athletes performing sprint races on a track.
Setting: Swiss Paraplegic Centre, Nottwil, Switzerland.
Methods: Three elite and four junior wheelchair athletes (18.7±6.8 years, 52.1±9.7 kg and 165.3±19.3 cm) performed five different exercise testing protocols at different speeds on a treadmill until exhaustion. Maximal effort treadmill (0.7% incline) testing protocols were performed using three timeframes. The first was focussing on short duration tests (S1 and S2) where incremental increases in velocity (0.42 and 0.1 m.s−1) were required from a stationary start. The second were medium duration tests (M1 and M2) where the athlete started at their 200 m and 800 m personal best time (mean velocities) and then had the velocity increased 1 km.h−1 by every 10 and 60 s respectively. The long duration test (L) started at 14 km.h−1 and velocity was increased by 2 km.h−1 every 120 s. Maximal heart rate, maximal concentration of lactate, maximal speed, and maximal duration of the test were measured.
Results: The highest concentration of lactate and the highest heart rates were measured in the longest tests.
Conclusion: During maximal effort testing wheelchair athletes are able to produce higher lactate concentrations when tested for longer duration. Post test lactate assessments provide little information in short duration testing protocols. Sequential lactate assessments post-test may provide additional information on the rate of recovery for middle distance wheelchair athletes and warrants further investigation.
Similar content being viewed by others

Introduction
In exercise physiology, the determination of maximum oxygen uptake (VO2max) is generally used as an indicator of the cardiorespiratory fitness of an individual.1 The correct determination of VO2peak requires an incremental test of several minutes to reach a maximum degree of exertion. Incremental tests are generally used to test endurance athletes.
For athletes performing sprint performances, special exercise testing protocols for measuring anaerobic capacity exist. Anaerobic exercise testing has been established for several years as a procedure for estimating the capacity of energy metabolism in short term exercise.2 In able-bodied persons, the Wingate Anaerobic Test (WAT) is well known.2 Compared with lower-body anaerobic exercise, upper-body anaerobic exercise testing is relatively new and less fully investigated.3 The WAT protocol is particularly suited for anaerobic assessment of individuals with lower limb disabilities, since it has been conceptualised for leg and arm cycling.2 Apart from the WAT, other protocols like the maximal velocity test (MVT) are known for paraplegics.4
The WAT is an all-out test lasting 30 s in comparison to the MVT lasting only 7–10 s. In these protocols power output or velocity are measured. Anaerobic exercise leads to an excessive production of lactate which can be measured in the capillary blood.5 The concentration of lactate can give an indication on the capacity of production and removal of lactate in the exercising body. The lower lactate concentrations, seen in trained athletes during exercise than in untrained subjects producing the same power output, are due to a diminished rate of appearance of lactate.5
Many wheelchair athletes perform races over short (100 m and 200 m), medium (400 m, 800 m and 1500 m) and long distances (10 km, half or complete marathon). At our institution only two exercise tests exist for athletes covering all these distances. For sprinter athletes, a sprint test on the treadmill was used. For endurance athletes, a VO2max on the treadmill was used.
The question we have asked ourselves is what test would be best suited for wheelchair athletes performing races of short and medium distances. A WAT or MVT may be too short and is not possible with our equipment of treadmill and wheelchair. And an incremental test determining the maximum concentration of lactate and VO2peak is probably too long. Therefore, we compared five different exercise protocols with different velocities and different durations on a treadmill. These were performed in order to find a suitable testing protocol for wheelchair athletes racing at short or medium distances. We expected that at short and intense bouts, higher maximal values for heart rate and lactate concentrations were reached, compared to rather long exercises.
Subjects and methods
Subjects
A total of seven wheelchair athletes participated in the study (Table 1). The protocol of the study was approved by the local ethics committee. Each athlete provided written informed consent.
Description of the exercise protocols
Every athlete reported to the laboratory to perform five different exercise protocols within the duration of 3 h. After arriving, heart rate at rest was measured with a heart rate monitor (Polar 4000, Polar Electro, Kempele, Finland). Concentration of lactate was also measured at rest (Super GL Ambulance, Ruhrtal Labor Technik, Möhnesee, Germany). The athletes performed the tests in their own racing wheelchairs. The wheelchairs were fixed to the treadmill (Saturn HP Cosmos, München, Germany) with a lever arm which could move along the treadmill between two retainers and had a range of movement of 0.6 m.
Before starting the exercise protocol, athletes had an individual warm up of 10 min. For all five protocols inclination was fixed at 0.7%. At termination of each test, maximal heart rate, concentration of lactate and velocity were recorded. After the test, the athletes took a rest of at least 15 min until they reached previously measured resting heart rate and felt recovered enough to complete the next test.
The five exercise testing protocols included two tests of short (S1 and S2) duration, two tests of median (M1 and M2) duration, and one test of long (L) duration. Maximal effort treadmill (0.7% incline) testing protocols were performed using three timeframes. The first was focussing on short duration tests (S1 and S2) where incremental increases in velocity (0.42 and 0.1 m.s−1) were required from a stationary start. The second were medium duration tests (M1 and M2) where the athlete started at their 200 m and 800 m personal best time (mean velocities) and then had the velocity increased 1 km.h−1 by every 10 and 60 s respectively. The long duration test (L) started at 14 km.h−1 and velocity was increased by 2 km.h−1 every 120 s.
They were allowed to touch the back retainer three times, at the fourth touch the test was stopped immediately. This procedure was chosen to allow for some degree of misplaced hand stroke. All tests were terminated when the mobile lever arm touched the back retainer for the fourth time.
Statistical analysis
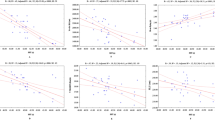
Correlations between maximal heart rate and duration of test, maximal lactate and duration of test, maximal velocity and duration of test, heart rate and maximal velocity, and for maximal heart rate and maximal lactate were determined. For parameters with a linear relationship, linear regressions were calculated. For parameters with an exponential relationship, curves are shown in the graphs but equations not given as this study is of descriptive rather than analytical nature.
Results
Heart rate
The exponential increase of heart rate with test duration is shown in Figure 1. Up to a test duration of approximately 4 min heart rate increases sharply, while heart rates of test durations between 5 and 15 min (L) are only slightly higher than in the tests of medium duration (M1 and M2) (Table 3).

Exponential relationship between heart rate at the end of each test and duration of the test (mean±STD). Curve is only for illustrative purposes and equation of the curve is not given
Lactate concentration
Lactate increased linearly (r=0.99, P=0.008) with test duration for tests up to approximately 300 s (S1, S2, M1, M2) (Figure 2). No further increase in lactate can be found between test M2 and L (Table 3). A significant linear correlation (r=0.95, P=0.01) was found between maximal heart rate and maximal lactate.

Linear correlation (S1, S2, M1, M2) between the concentration of lactate at the end of the test and duration of the test (mean±STD)
Speed
Maximum speed decreased exponentially with increasing test duration (Figure 3). The highest maximum speed (group mean) reached was 42.8 km.h−1 in S1 (Table 3). At test durations of between 3 and 15 min, maximum speeds no longer declined and were between 22 and 25 km.h−1 (group means).

Exponential relationship between maximum speed at the end of each test and duration of the test (mean±STD). Curve is only for illustrative purposes and equation of the curve is not given
Duration of exercise
The higher the acceleration and consequently the speed of the exercise test, the shorter the duration (Table 3). Test duration was positively related to heart rate (Figure 1), lactate production (Figure 2), and negatively to maximum speed.
Discussion
We expected the highest lactate concentrations and the highest heart rates at the shortest and most intense exercise with the highest speed. However, the opposite was found in our study: lactate concentrations and heart rate increased with increasing exercise test duration. This could be due to the kind of exercise test or the limited muscle mass of wheelchair athletes compared to able bodied athletes.
Kind of exercise
According to the WAT, exercise duration of an anaerobic test should not be longer than 30 s.2 In able-bodied athletes, the highest lactate concentrations are measured after 30 s of anaerobic exercise. Comparable to this with regard to test duration was S1 with a mean duration of 34.4±9.2 s, however, this test showed the lowest concentrations of lactate (Figure 3). Our tests are not directly comparable to the WAT because power output was maximal only at the end of the tests, while in the WAT power output is maximal throughout the whole test. Therefore, for a ramp test, a test duration of around 30 s may be too short to activate anaerobic glycolysis. Performance may be done anaerobically without accumulation of lactate utilising the creatine phosphate stores for up to 20 or 30 s.6
Time of exercise
When we compare the personal best times for 200 m and 800 m with the average time reached in the tests, we find important differences. The personal best time for 200 m with 32.4±2.7 s for the seven athletes (Table 2a) was near to the time in S1 (Table 2b). However in this exercise, lowest lactate levels were reached (Table 3). Personal best time for 800 m with 127.9±13.0 was between the time in M1 and M2 (Table 2b). Lactate concentration was higher in M2 than in M1, but in both tests they did not reach the highest lactate concentration (Table 3). To have information about performance for sprint athletes, it would be best to measure time in S1 without measuring lactate. The concentration of lactate does not give a further information. For middle distance athletes, measurement of lactate in a longer exercise test would give a good information about performance.
Limited muscle mass
Wheelchair athletes involve less muscle mass during exercise than able bodied persons. It may be applicable to consider that lactate levels in the blood correlate well with muscle mass activity. When small muscle masses are activated, the localised fatigue is probably the dominant factor to fail in the exercise. The high intensity in the short exercise tests combined with the small muscle mass involved may cause a localised peripheral fatigue that leads to cessation of the exercise. Therefore the lactate levels are lower.
Cardiovascular system in SCI
Besides the aspects of muscle morphology, the impairment of the cardiovascular system in SCI could be a reason for altered metabolic mechanisms in exercise of short duration. A lesion above T6 of the spinal cord leads to the loss of the sympathetic nervous system. This leads to a dysregulation of the cardiovascular system with a reduced mean blood pressure and a reduced cardiac output.7 However, of our seven subjects only one athlete had a lesion above T6 (Table 1), and this subject had heart rates comparable to the other subjects.
Measurement of lactate at the end of test
Also the samples of lactate analysis could give more evidence if additional samples were taken 2 and 4 min after exercise termination. It is well known, that lactate distribution needs some time to reach maximal concentration when measuring at the earlobe.8,9,10 In these short tests lactate samples should be taken at termination, 2, 4 and maybe also 6 min after interruption of the test to receive more information about the anaerobic metabolism above all in elite athletes. The recovery period of about 15 min between the five tests were arranged individually to reach maximal regeneration. Some athletes preferred to move on some minutes at low intensity, others to rest totally. Baker and King11 showed that between low intensity arm exercise and rest, there was no significant difference in lactate clearance to base level in all athletes. Especially in the M1 and M2 test recovery period should have been longer for some less trained athletes.
This could be another influence of higher lactate concentrations at the end of the longer tests. Another explanation for our lactate concentrations could be the age of the four junior athletes. It is known, that in prepubertal athletes the immaturity of anaerobic metabolism limits the production of muscle lactate relative to adults.12
Conclusion
During maximal effort testing wheelchair athletes are able to produce higher lactate concentrations when tested for longer duration. Post test lactate assessments provide little information in short duration testing protocols. Sequential lactate assessments post-test may provide additional information on the rate of recovery for middle distance wheelchair athletes and warrants further investigation.
References
Bassett DR & Howley ET . Limiting factors for maximum oxygen uptake and determinants of endurance performance. Med Sci Sports Exerc 2000; 33: 70–84.
Bar-Or O . The Wingate anaerobic test: an update on methodology, reliability and validity. Sports Med 1987; 4: 381–397.
Hutzler Y . Anaerobic fitness testing of wheelchair users. Sports Med 1998; 25: 101–113.
Lees A . Performance characteristics of two wheelchair sprint tests. In: van der Woude LHV, Meijs PJM, de Boer YA (ed). Ergonomics of Manual Wheelchair Propulsion, State of the Art, Amsterdam: IOS Press, 1993; pp 85–91.
MacRae HSH, Dennis SC, Bosch AN & Noakes TD . Effects of training on lactate production and removal during progressive exercise in humans. J Appl Physiol 1992; 72: 1649–1656.
McGilvery RW . The use of fuels for muscular work. In: Metabolic adaptation to prolonged physical exercise. Proceedings of the Second International Symposium on Biochemistry of Exercise Magglingen 1973, Howald H, Portmans JR (ed). Basel: Birkhäuser Verlag, 1975; pp 12–30.
Kessler KM et al. Cardiovascular findings in quadriplegic and paraplegic patients and in normal subjects. Am J Cardiol 1986; 58: 525–530.
Taoutaou Z et al. Lactate kinetics during passive and partially active recovery in endurance and sprint athletes. Eur J Appl Physiol 1996; 73: 465–470.
Koziris LP & Montgomery DL . Blood lactate concentration following intermittent and continuous cycling tests of anaerobic capacity. Eur J Appl Physiol 1991; 63: 273–277.
Gupta S, Goswami A, Sadhukhan AK & Mathur DN . Comparative study of lactate removal in short term massage of extremities, active recovery and a passive recovery period after supramaximal exercise sessions. Int J Sports Med 1996; 17: 106–110.
Baker SJ & King N . Lactic acid recovery profiles following exhaustive arm exercise on a canoeing ergometer. Br J Sports Med 1991; 25: 165–167.
Boisseau N & Delamarche P . Metabolic and hormonal responses to exercise in children and adolescents. Sports Med 2000; 30: 405–422.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Knechtle, B., Hardegger, K., Müller, G. et al. Evaluation of sprint exercise testing protocols in wheelchair athletes. Spinal Cord 41, 182–186 (2003). https://doi.org/10.1038/sj.sc.3101416
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101416
