
Abstract
Alterations in processing of emotionally salient information have been reported in individuals with major depressive disorder (MDD). Evidence suggests a role for noradrenaline in the regulation of a cortico-limbic-striatal circuit that has also been implicated in the pathophysiology of MDD. Herein, we studied the physiological consequences of a common coding polymorphism of the gene for the α2C-adrenoreceptor (AR) subtype—the deletion of four consecutive amino acids at codons 322–325 of the α2C-AR (α2CDel322–325-AR) in medication-free, remitted individuals with MDD (rMDD), and healthy control subjects. After injection of 10 mCi of H215O, positron emission tomography (PET) measures of neural activity were acquired while subjects were viewing unmasked sad, happy, and fearful faces. The neural responses to sad facial expressions were increased in the amygdala and decreased in the left ventral striatum in rMDD patients relative to healthy control subjects. Furthermore, we report that rMDD carriers of one or two copies of the α2CDel322–325-AR exhibit greater amygdala as well as pregenual and subgenual anterior cingulate gyrus neuronal activity in response to sad faces than healthy α2CDel322–325-AR carriers and rMDD noncarriers. These results suggest that the α2CDel322–325-AR confers a change in brain function implicating this α2-AR subtype into the pathophysiology of MDD.
Similar content being viewed by others

INTRODUCTION
Major depressive disorder (MDD) is a complex disorder and the neurobiological basis of MDD is not fully understood. There is increasing attention to the role of noradrenaline for both the pathogenesis and treatment of MDD. Noradrenergic mechanisms were the first to be studied intensively in MDD (Schildkraut, 1965). Early studies reported elevations in the plasma (Barnes et al, 1983; de Villiers et al, 1987; Louis et al, 1975; Roy et al, 1988, 1985; Rudorfer et al, 1985; Wyatt et al, 1971), urine (Maas et al, 1987), and cerebrospinal fluid (CSF) (Wong et al, 2000) noradrenaline levels. Noradrenaline kinetic analyses revealed an increased rate of noradrenaline appearance in the extravascular and vascular compartments in MDD patients, but similar rates of noradrenaline clearance in depressed patients and controls (Veith et al, 1994). This argues for increased peripheral sympathoneural activity in MDD and is consistent with the hypothesis that presynaptic control of noradrenaline release may be impaired in at least a subgroup of patients with MDD.
The hypothesis that central noradrenaline function is increased in a subgroup of MDD patients is supported by the clinical and biochemical resemblance between the symptom complex of MDD and consequences of increased central noradrenaline function. Both are characterized by arousal, fear-related behaviors, changes in feeding, grooming and sleeping, and changes in cognition. In addition, because stimulation of α1 and α2 adrenoreceptors (AR) plays major roles in modulating limbic–hypothalamic–pituitary–adrenal axis responses during stress (Calogero et al, 1988; Ma and Morilak, 2005), the hypercortisolism commonly found in MDD conceivably may be related to altered noradrenaline regulation in cortico-limbic circuits in MDD. Post-mortem studies in MDD, however (Ordway et al, 2003; Callado et al, 1998), have reported alterations in α2-ARs resulting in a deficiency of noradrenaline in MDD.
In MDD patients, functional imaging studies show increased activity of a distributed neural system involving prefrontal cortical, striatal, and limbic structures in currently depressed subjects at rest and during task performance (Drevets, 1998; Mayberg et al, 1999) and a positive correlation between depression severity and amygdala metabolism (Abercrombie et al, 1996; Drevets et al, 1992). Studies comparing neural responses to emotionally expressive faces found that the hemodynamic responses of the amygdala were increased when viewing sad faces vs neutral faces (Drevets et al, 2001) or vs fixation point baseline (Fu et al, 2004; Surguladze et al, 2005) in depressives relative to controls. In contrast, hemodynamic responses of the amygdala decreased to fearful faces vs neutral faces in depressed adults relative to controls (Drevets et al, 2001) and to fearful faces vs fixation point baseline in depressed children relative to controls (Thomas et al, 2001). However, left amygdala responses were reportedly increased in depressives vs controls when hemodynamic activity measured during exposure to fearful and happy faces presented using a backward masking technique (so that subjects were unaware of having seen the emotional faces) was compared with activity during fixation point baseline (Sheline et al, 2001). Notably, the abnormally increased amygdalar responsivity to negatively valenced faces in depressed subjects was attenuated by antidepressant drug treatment (Sheline et al, 2001; Fu et al, 2004).
Furthermore, during a spontaneous episode of MDD, enhanced responses to negative emotional stimuli were shown within the rostral anterior cingulate cortex and orbitofrontal cortex (Elliott et al, 2002; Phillips et al, 2003). There is evidence that these altered neural responses to emotional stimuli persist beyond the symptomatic phase of the illness, suggesting they may represent a trait-like characteristics for MDD (Liotti et al, 2002). A major limitation of previous investigations in MDD for identifying a primary noradrenergic neural circuit related to high risk for MDD was that in most studies patients were studied while symptomatically depressed and on antidepressant medication. The present study aimed to avoid these confounds by including medication-free, fully remitted patients with MDD who were exposed to sad, happy, and fearful facial expressions.
Based upon the compelling evidence that enhanced noradrenaline release may play an important role in the pathogenesis of MDD, and particularly that noradrenaline affects functions of a cortico-limbic circuit, which has been implicated in the pathophysiology of MDD, an obvious next step of investigation is to determine whether noradrenaline related genes that regulate brain noradrenaline function account for the very robust differential neural responses to emotional valenced stimuli in MDD patients relative to healthy controls. We have studied one potentially important mechanism, a genetic variant of the α2C-adrenoreceptor (AR) subtype, designated α2CDel322–325-AR, which leads to increased noradrenaline release in healthy people who carry this genetic variant (Neumeister et al, 2005). Reported frequencies of this genetic variant are 44% in African Americans, and 4% in Caucasian control populations (Feng et al, 2001). Two studies, one from the National Institute of Mental Health and the other from Yale University School of Medicine (unpublished data) show that European-American patients with MDD carry at least one copy of the α2CDel322–325-AR more often compared to healthy controls.
We predicted increased activity to sad and fearful, relative to happy facial expressions in a cortico-limbic-striatal circuit in patients with MDD relative to controls. Moreover, testing the hypothesis that the α2CDel322–325 polymorphism confers a change in brain function, we predicted that these differences will be most pronounced in MDD carriers of the α2CDel322–325 polymorphism.
PATIENTS AND METHODS
In total, 27 (18 women, age 39.7±12.8 years; 23 European Americans, four African Americans) remitted (Hamilton Depression Rating Scale (HDRS, 24-item) score: 0.7±0.9), unmedicated patients with a diagnosis of MDD on the basis of the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, nonpatient version (First et al, 1996), and 26 healthy controls (17 women, age 34.2±11.2 years; 15 European Americans, one Asian, nine African Americans, one Hispanic; HDRS score: 0.5±0.8) were included in the study. Durations of the depressive illness and number of episodes were estimated from the Past History of MDD addendum to the SCID. Remission was defined as a period of at least 3 months during which the subject did not take an antidepressant agent and with HDRS scores in the nondepressed range (<8) (Frank et al, 1991). Patients with MDD were remitted for 40.4±48.4 months, and had been off antidepressant medications for 39.1±44.3 months at the time of their study. Information about family history of mental illness (axis I diagnoses) was obtained from the study participants for all first degree relatives using the Family Interview of Genetic Studies (Maxwell, 1992). Controls had no personal or family (first-degree relatives) history of psychiatric disorders. No use of medication was allowed within the 3 weeks prior to scanning. Participants were free of medical illness on the basis of history and results of physical examination, electrocardiogram, and laboratory tests, including liver and kidney function tests, hematologic profile, thyroid function tests, urinanalysis, and toxicology. Pregnant and nursing women were excluded. Premenopausal women were studied during the follicular phase of the menstrual cycle. At the time of screening, written informed consent was obtained as approved by the NIMH Institutional Review Board from all subjects after full explanation of the purpose of the study and the study procedures.
Genotyping
On the screening day, a blood sample was collected for genotyping the α2C-AR subtype. The investigators were blinded regarding the genetic status of the subjects and results of genotyping were not shared with the study participants. α2CDel322–325-AR genotyping was performed by DNA fragment analysis on a capillary sequencer (ABI 3100) and genotypes were generated using Genotyper software on the device (ABI, Foster City, CA). Primer and probe sequences for the α2C-AR polymorphism are as follows: forward primer (HEX)= AGACGGACGAGAGCAGCGCA and reverse primer (ABD Tail)= AGGCCTCGCGGCAGATGCCGTACA . The α2CDel322–325-AR 20 μl reaction volume contained 100 ng genomic DNA, but 4 μl 5 × Buffer A (Invitrogen), 20 ng of each primer; 0.8 mM dNTPs (ABI); 0.5 μl Platinum Taq Polymerase (Invitrogen); and 2 μl DMSO. α2CDel322–325-AR was amplified by a 4 min hot start at 94°C followed by 35 cycles of 30 s at 94°C, 30 s at the optimal annealing temperature (65°C), 30 s at 72°C for elongation and a final 7 min elongation at 72°C. PCR was carried out with an ABI 9700. Error rate was <0.005 and genotype completion rate was 0.99.
Procedure
All subjects participated in one positron emission tomography (PET) scanning session. During this session, grey-scale, static face picture stimuli taken from a standard set of pictures of facial affect (Ekman and Friesen, 1976) were presented. Because we were only interested in determining the responses to a block of emotionally expressive faces that were of a single emotion, within an individual scan all face stimuli shown over a period of 70 s were of the same emotional valence and intensity. The order of presentation of sad, happy, and fearful faces was randomly chosen. Previous studies have shown that neural responses to emotional stimuli depend of the nature of the task performed. The task instructions were the same for all scans, as subjects were asked to indicate the gender of each face by pressing the left button on a two-button fiberoptic key pad for male and the right for female. The face stimuli were displayed at 1/s on a Macintosh computer monitor using Super Lab™ software. This frequency was selected because it permitted adequate time to assign gender, and the short stimulus duration minimized the likelihood of scanning eye movements. Eye movement was not evident during random checks during stimulus presentation, as at the 1/s rate of stimulus presentation the experimental subject's eyes remained fixed on the pictured subject's eyes and did not scan the faces. Performance accuracy for assigning the correct gender to the presented faces was obtained from a computer log file that recorded key pad responses. In the gender-classification task, subjects in all groups identified correctly 90–100% of the time.
Potential changes in emotional state in response to the face stimuli were assessed by comparing changes in the heart rate recorded with an electrocardiogram, and changes in subjective ratings of the intensity and quality of the emotional experience measured using 10 point analog scales to rate anxiety, sadness and happiness. The remitted MDD (rMDD) patients did not differ from healthy control subjects on either measure.
Image Acquisition and Analysis
Magnetic resonance images (MRI) were obtained for each subject using a GE Signa Scanner (3.0 T) and a 3D MPRAGE sequence (TE=2.982 ms, TR=7.5 ms, inversion time=725 ms, voxel size=0.9 × 0.9 × 1.2 mm3) to provide an anatomical framework for analysis of the PET image data and morphological characterization so that subjects with anatomical abnormalities could be excluded.
PET scans were acquired using a GE Advance (35 contiguous slices with 4.25 mm plane separation; 3D resolution=6–7 mm FWHM, 3D acquisition mode) PET scanner. A transmission scan was obtained to perform measured attenuation correction of the emission scans. Subsequently, four cerebral blood flow (CBF) scans were acquired at an 8 min inter-scan interval using bolus injection of 10 mCi of H215O. Stimulus presentation was initiated approximately 5 s after the start of the emission scan to minimize the amount of habituation that may occur prior to the arrival of the 15O bolus to the head (the fixation point CBF scan that precedes the experimental scans permitted estimation of the lag time between H215O injection and the rise in radioactive counts from the head). Stimulus exposure was about 5 s longer than the PET scan.
The data were analyzed using MRI-based region of interest (ROI) analysis using MEDx software (Sensor Systems, Sterling, VA). The global activity was measured using an MRI-based template. ROI selection was both theory and data-driven. The number of regions was intentionally limited to regions that have been commonly associated with MDD in functional imaging studies at rest and in response to emotive stimuli during both, a spontaneous episode of MDD and in remission. ROI included the amygdala, hippocampus, orbitofrontal cortex, subgenual, and pregenual anterior cingulate gyrus, and the ventral striatum. These regions were placed on each subject's registered MRI scan. A binary mask of the gray matter was then used to ensure that only gray matter pixels were included in the analysis. Regions were then transferred to the coregistered PET images, and rCBF was obtained for each ROI. The whole brain measure was used to normalize the regional measures.
Statistical Analysis
A full factorial repeated measures MANOVA was used to examine the whole brain normalized O-15 data for six ROIs—amygdala, hippocampus, subgenual anterior cingulate gyrus, pregenual anterior cingulate gyrus, orbital frontal cortex, and ventral striatum. The model included group (rMDD vs controls) and genotype (noncarriers vs homozygous and heterozygous carriers of the α2CDel322–325-AR) as between-subject factors and emotion (sad, happy, fear) and side (left vs right hemisphere) as within-subjects factors. Significant multivariate tests (ie Pillai's trace) were followed by separate ANOVAs for each ROI using the same factors as the MANOVA.
The Shapiro–Wilk's test was used to evaluate the normality of the distribution of each outcome variable and Mauchly's test was used to examine sphericity. When nonsphericity of the data was evident, the Greenhouse–Geisser adjustment was applied. Significant interactions and omnibus main effects were followed by Bonferroni corrected simple effects tests. Significance was interpreted at p<0.05, two-tailed.
RESULTS
Eight rMDD patients and nine healthy controls carried at least one copy of the α2CDel322–325 polymorphism, 19 rMDD patients, and 17 control subjects were noncarriers. The overall MANOVA showed a significant main effect of side (F(6,44)=9.18, p<0.001) and a trend towards significance for genotype (F(6,44)=2.05, p=0.079). Significant interactions were found for emotion × group (F(12,38)=3.41, p=0.002) and emotion × group × genotype (F(12,38)=2.90, p=0.046).
Group Effects
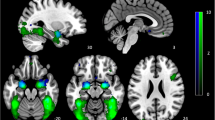
The ANOVAs showed that patients with rMDD differed in their neural responses to emotional stimuli compared to controls in the amygdala (emotion × group interaction: F(2,98)=4.40, p=0.015) and the subgenual anterior cingulate gyrus (emotion × group interaction: F(2,98)=6.50, p=0.002). An additional effect of side was found for the ventral striatum (emotion × group × side interaction: F(2,98)=3.20, p=0.045). In the amygdala (t=2.75, df=49, p=0.047), rMDD patients showed exaggerated responses to sad faces compared to healthy control subjects (Figure 1). In contrast, rMDD subjects compared to healthy controls showed blunted left ventral striatum (t=3.36, df=49, p=0.002) responses to sad faces (Figure 1). No between-group differences in neural responses to happy or fearful faces were found in these two regions. In the subgenual anterior cingulate gyrus, but not the amygdala or the ventral striatum healthy controls, showed higher activation to fearful vs sad faces (t=2.78, df=22, p=0.030) and fearful vs happy faces (t=3.00, df=22, p=0.016). No significant differences in activation in any of the aforementioned regions between any of the three emotional facial expressions were found in the MDD patients.

Regional cerebral blood flow (rCBF) values of individuals with remitted major depressive disorder (rMDD) and healthy control subjects. rCBF measurements were normalized to the whole brain measure (rCBF/gCBF). Data show between-group differences in neural responses to sad facial expressions in the amygdala and the left ventral striatum (VS). Values are presented as means±SEM. * indicates p<0.05 (two-tailed, unpaired t-test after Bonferroni correction).
Gene–Group Interactions
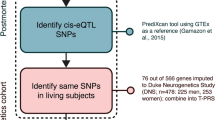
The evaluation of an effect of the α2CDel322–325-AR on processing of emotionally salient material in patients with MDD and healthy control subjects revealed a significant emotion × group × genotype interaction for the amygdala (F(2,98)=3.20, p=0.045) and for the subgenual anterior cingulate gyrus (F(2,98)=3.18, p=0.048). This suggests that in these two regions genetic variants of the α2C-AR directly affect the neural responses to emotional faces in MDD and healthy control subjects. No significant genotype × emotion × group interaction was found for any of the other a priori defined ROI. An additional significant group × genotype interaction was found for the pregenual anterior cingulate gyrus (F(1,49)=5.50, p=0.023). The effect in this region was generated from the neural responses to the sad faces. MDD carriers of the α2CDel322–325-AR compared to healthy control subject carriers of the α2CDel322–325-AR showed higher amygdala (t=3.79, df=49, p=0.029), subgenual (t=2.12, df=49, p=0.039), and pregenual anterior cingulate gyrus (t=2.69, df=49, p=0.010) activation in response to viewing sad faces. No difference in activation in any of these regions was found between MDD and healthy control noncarriers in response to sad faces (Figure 2). In response to happy and fearful faces, amygdala activation did not differ between MDD patients and controls in any genotype group.

Amygdala (top), subgenual anterior cingulated gyrus (SACG; middle), and pregenual anterior cingulate gyrus (PACG; bottom) activation to unmasked sad faces in major depressive disorder (MDD) carriers vs healthy control carriers of at least one copy of the α2CDel322-325-adrenoreceptor (AR), and noncarriers. Values reflect regional cerebral blood flow (rCBF) values normalized to the whole-brain measure (rCBF/gCBF). * indicates p<0.05 (two-tailed, unpaired t-test after Bonferroni correction). NS indicates not significant (two-tailed, unpaired t-test after Bonferroni correction).
Healthy α2CDel322–325-AR carriers (but not healthy noncarriers) and rMDD patients in any genotype group showed higher amygdala activation to sad faces relative to happy faces (t=2.80, df=22, p=0.024) and blunted amygdala activation in response to fearful faces relative to happy faces (t=2.88, df=22, p=0.020). Healthy noncarriers showed higher subgenual anterior cingulate gyrus activation in response to fearful faces than rMDD noncarriers (t=2.73, df=49, p=0.038).
DISCUSSION
The role of cortico-limbic-striatal circuits in the response to emotionally salient stimuli has been previously highlighted, with specific patterns of functional abnormalities within these regions reported in MDD patients during a spontaneous episode of depression (Phillips et al, 2003). We aimed to examine whether these abnormalities, which have been consistently reported in MDD in response to facial expressions of negative emotion, represent a state-dependent abnormality characteristic for MDD, or rather a trait characteristic. In addition, given the suggested role of noradrenaline in the regulation of this circuit, we were particularly interested whether a functional genetic variant of the α2C-AR, which was shown to affect noradrenaline function in humans and leads to increased and sustained noradrenaline release (Neumeister et al, 2005) modulates neural responses to emotionally salient information in MDD and healthy control subjects.
Our results provide evidence that a distinct pathway including the amygdala, the anterior cingulate gyrus, and the left ventral striatum is involved in the neural processing of emotional facial expressions in MDD. We found increased activation in response to sad faces in the amygdala, and a blunted response to sad faces in the left ventral striatum in remitted, unmedicated MDD patients relative to healthy control subjects. These findings of amygdala hyperresponsivity to sad faces agree with previous functional imaging studies in MDD patients studied during a spontaneous episode of MDD (Fu et al, 2004; Lawrence et al, 2004; Drevets et al, 2001). In contrast, the findings in the left ventral striatum in remitted MDD cases are opposite in direction to those reported in currently depressed MDD subjects by Fu et al (2004). Taken together with the results of previous studies of symptomatically depressed subjects with MDD, our results in rMDD cases address the question of whether abnormal neural responses during exposure to emotional salient information in MDD are related to current mood states or instead reflect an underlying trait abnormality in responsiveness to emotionally salient stimuli characteristic for MDD. These collective findings suggest that amygdala hyperresponsivity to sad faces may constitute a trait abnormality in a subgroup of patients with MDD, while the corresponding responses in the left ventral striatum are mood state dependent.
Notably, in the present study, the exaggerated hemodynamic responses to emotional face stimuli in cortico-limbic striatal circuits between rMDD patients and healthy controls were found only in response to sad, but not other negative stimuli, for example, fearful faces, or in response to happy faces. This highlights another potentially important aspect of the altered processing of emotionally salient information in MDD, namely that they appear ‘disorder-congruent’ with respect to showing specificity for sad faces. In contrast, the rMDD cases showed reduced blood flow in the amygdala during presentation of fearful faces vs happy faces. These data were compatible with previous reports that hemodynamic responses were decreased in the left amygdala to fearful faces vs neutral faces in depressed adults relative to healthy controls (Drevets et al, 2001) and to fearful faces vs fixation point in depressed children relative to anxious and healthy controls (Thomas et al, 2001). These data differ, however, from those of a previous report demonstrating increased amygdala activation in response to both fearful and happy faces relative to fixation point baseline among currently depressed MDD patients relative to controls (Sheline et al, 2001). This divergence in the results across these studies may be accounted for differences in stimulus presentation, as Sheline et al displayed their emotional face stimuli for 40 ms and then ‘masked’ them with a neutral face (so that subjects denied conscious awareness of having seen an emotional face), while the studies finding blunted amygdala responses to fearful faces displayed the emotional faces explicitly (ie for stimulus durations between 200 and 1000 ms) so that subjects were consciously aware of having viewed the emotionally expressive faces (see Patients and methods, and Thomas et al, 2001; Drevets et al, 2001). Previous research has shown that amygdala activation is not contingent upon explicit processing of facial expression (Morris et al, 1996; Whalen et al, 1998). Therefore, our study argues against unspecific hyper-responsiveness of the circuit in remitted MDD in response to negative facial expressions per se, but instead highlights the importance of disorder-congruent (ie sad) stimuli to elicit hyperresponsiveness of the circuit. We conclude that exaggerated responsiveness to or processing of sad faces is a trait characteristic for MDD. In addition, blunted amygdala activation in response to fearful faces in MDD patients also may constitute such a trait abnormality, but this finding may extend only to designs in which the face stimuli are presented above the level of conscious awareness and the hemodynamic responses to fearful faces are contrasted to those obtained when viewing happy faces.
Our results show hyper-responsiveness of the amygdala and the anterior cingulate gyrus in MDD in response to facial expressions of sadness. The finding that hyper-responsiveness to sad faces is found only in α2CDel322–325-AR MDD patients, but not in noncarriers implicates a genetically determined link between α2C-AR function and the response of brain regions critical for emotional processing in MDD, unconstrained of symptomatology. Notably, healthy α2CDel322–325-AR carriers also showed amygdala hyper-responsiveness. Genetic epidemiological studies are needed to determine whether altered neuronal responsiveness to emotionally salient information predicts the development of MDD. This genetically driven altered reactivity of the amygdala and the subgenual anterior cingulate gyrus adds to the existing literature of altered neuronal function in MDD, possibly related to altered noradrenaline function. Evidence suggests a role of this genetic variant for MDD because of pronounced and sustained hyper-noradrenergic function in at least subgroups of patients with MDD (Wong et al, 2000). It also has been hypothesized, however, that chronically increased noradrenaline release into the synaptic cleft that exceeds the capacity of the neuron to return noradrenaline into presynaptic vesicles; however, there can be net neuronal loss of noradrenaline (Eisenhofer et al, 1996; Meredith et al, 1993), which is considered a feature of chronic depression if untreated or unsuccessfully treated (Lambert et al, 2000).
We did not observe any between-group differences in performance (accuracy or reaction time) indicating that general attentional, perceptual, or cognitive phenomena did not contribute to the observed neuroimaging differences. Also, rMDD patients did not differ from healthy control subjects in behavioral assessments or electrophysiological measures. This highlights the strength of functional imaging using PET to directly link brain function with a phenotype related to a functional polymorphism of a gene critical for adaptive central and peripheral noradrenaline function (Rosin et al, 1996).
This study has limitations. First, recent work shows substantial divergence between certain α2C haplotypes and a partitioning of the α2CDel322–325 polymorphism into multiple haplotypes (Small et al, 2004). In addition, it was shown that these haplotypes influence cellular expression of the α2C-AR transcript and protein. Notably, the coding polymorphism α2CDel322–325 is present in two of three low expressing haplotypes and European Americans have much less haplotype diversity than other racial groups, for example, African Americans or Asians. Our groups of rMDD patients and healthy controls included European Americans, as well as African Americans, Hispanics and Asians. We did not perform a haplotype analysis on these data given the relatively small sample size of each ethnic group. To date, the relevance of the reported haplotypes for the pathophysiology of MDD is unclear and needs to be addressed in future studies specifically addressing this question in racially more homogenous populations.
Second, we report data on the neural responses to emotional salient information in genetically stratified individuals with MDD and healthy control subjects, and aimed to provide a biochemical explanation related to genetically determined alterations in noradrenaline function. Ideally, we would prefer direct measurements by using PET imaging to study an endogenous competition model related to noradrenaline release and uptake. Suitable PET radioligands are not yet available for this work, however. In this context, this study is a logical starting point, which aims to ultimately lead to the studies directly determining noradrenaline transporters and receptors in MDD.
Our results suggest that a genetic variant of the α2C-AR subtype confers a change in brain function playing a role in the pathogenesis of MDD. Whether this study and ongoing genetic analyses and imaging studies may suggest a pattern, which could predict the future course of MDD and could in the future help identify people at high risk for subsequent episodes vs people who may carry a lower risk remains to be determined.
References
Abercrombie HC, Larson CL, Ward RT (1996). Metabolic rate in the maygdala predicts negative affect and depression severity in depressed patients; an FDG-PET study. Neuroimage S217.
Barnes RF, Veith RC, Borson S, Verhey J, Raskind MA, Halter JB (1983). High levels of plasma catecholamines in dexamethasone-resistant depressed patients. Am J Psychiatry 140: 1623–1625.
Callado LF, Meana JJ, Grijalba B, Pazos A, Sastre M, Garcia-Sevilla JA (1998). Selective increase of alpha2A-adrenoceptor agonist binding sites in brains of depressed suicide victims. J Neurochem 70: 1114–1123.
Calogero AE, Gallucci WT, Chrousos GP, Gold PW (1988). Catecholamine effects upon rat hypothalamic corticotropin-releasing hormone secretion in vitro. J Clin Invest 82: 839–846.
de Villiers AS, Russell VA, Carstens ME, Aalbers C, Gagiano CA, Chalton DO et al (1987). Noradrenergic function and hypothalamic–pituitary–adrenal axis activity in primary unipolar major depressive disorder. Psychiatry Res 22: 127–140.
Drevets WC (1998). Functional neuroimaging studies of depression: the anatomy of melancholia. Annu Rev Med 49: 341–361.
Drevets WC, Gautier C, Lowry T, Bogers W, Greer P, Kupfer D (2001). Abnormal hemodynamic responses to facially expressed emotion in major depression. Soc Neurosci Abstr 31.
Drevets WC, Videen TO, Price JL, Preskorn SH, Carmichael ST, Raichle ME (1992). A functional anatomical study of unipolar depression. J Neurosci 12: 3628–3641.
Eisenhofer G, Friberg P, Rundqvist B, Quyyumi AA, Lambert G, Kaye DM et al (1996). Cardiac sympathetic nerve function in congestive heart failure. Circulation 93: 1667–1676.
Ekman P, Friesen WV (1976). Pictures of Facial Affect. Consulting Psychologists: Palo Alto.
Elliott R, Rubinsztein JS, Sahakian BJ, Dolan RJ (2002). The neural basis of mood-congruent processing biases in depression. Arch Gen Psychiatry 59: 597–604.
Feng J, Zheng J, Gelernter J, Kranzler H, Cook E, Goldman D et al (2001). An in-frame deletion in the alpha(2C) adrenergic receptor is common in African-Americans. Mol Psychiatry 6: 168–172.
First MB, Gibbon M, Spitzer RL, Williams JBW (1996). Structured Clinical Interview for DSM-IV Axis I Disorders: Nonpatient Edition (SCID-I/NP). Biometrics Department, New York State Psychiatric Institute: New York.
Frank E, Prien RF, Jarrett RB, Keller MB, Kupfer DJ, Lavori PW et al (1991). Conceptualization and rationale for consensus definitions of terms in major depressive disorder remission, recovery, relapse, and recurrence. Arch Gen Psychiatry 48: 851–855.
Fu CH, Williams SC, Cleare AJ, Brammer MJ, Walsh ND, Kim J et al (2004). Attenuation of the neural response to sad faces in major depression by antidepressant treatment: a prospective, event-related functional magnetic resonance imaging study. Arch Gen Psychiatry 61: 877–889.
Lambert G, Johansson M, Agren H, Friberg P (2000). Reduced brain norpienephrine and dopamine release in treatment-refractory depressive illness: Evidence in support of the catecholamine hypothesis of mood disorders. Arch Gen Psychiatry 57: 787–793.
Lawrence NS, Williams AM, Surguladze S, Giampietro V, Brammer MJ, Andrew C et al (2004). Subcortical and ventral prefrontal cortical neural responses to facial expressions distinguish patients with bipolar disorder and major depression. Biol Psychiatry 55: 578–587.
Liotti M, Mayberg HS, McGinnis S, Brannan SL, Jerabek P (2002). Unmasking disease-specific cerebral blood flow abnormalities: mood challenge in patients with remitted unipolar depression. Am J Psychiatry 159: 1830–1840.
Louis WJ, Doyle AE, Anavekar SN (1975). Plasma noradrenaline concentration and blood pressure in essential hypertension, phaeochromocytoma and depression. Clin Sci Mol Med Suppl 2: 239s–242s.
Ma S, Morilak DA (2005). Norepinephrine release in medial amygdala facilitates activation of the hypothalamic–pituitary–adrenal axis in response to acute immobilisation stress. J Neuroendocrinol 17: 22–28.
Maas JW, Koslow SH, Davis J, Katz M, Frazer A, Bowden CL et al (1987). Catecholamine metabolism and disposition in healthy and depressed subjects. Arch Gen Psychiatry 44: 337–344.
Maxwell ME (1992). Manual for the Family Interview for Genetic Studies (FIGS). Clinical Neurogenetics Branch, National Institute of Mental Health: Bethesda.
Mayberg HS, Liotti M, Brannan SK, McGinnis S, Mahurin RK, Jerabek PA et al (1999). Reciprocal limbic-cortical function and negative mood: converging PET findings in depression and normal sadness. Am J Psychiatry 156: 675–682.
Meredith IT, Eisenhofer G, Lambert GW, Dewar EM, Jennings GL, Esler MD (1993). Cardiac sympathetic nervous activity in congestive heart failure. Evidence for increased neuronal norepinephrine release and preserved neuronal uptake. Circulation 88: 136–145.
Morris JS, Frith CD, Perrett DI, Rowland D, Young AW, Calder AJ et al (1996). A differential neural response in the human amygdala to fearful and happy facial expressions. Nature 383: 812–815.
Neumeister A, Charney DS, Belfer I, Geraci M, Holmes C, Sharabi Y et al (2005). Sympathoneural and adrenomedullary functional effects of alpha2C-adrenoreceptor gene polymorphism in healthy humans. Pharmacogenet Genomics 15: 143–149.
Ordway GA, Schenk J, Stockmeier CA, May W, Klimek W (2003). Elevated agonist binding to alpha2-adrenoceptors in the locus coeruleus in major depression. Biol Psychiatry 53: 315–323.
Phillips ML, Drevets WC, Rauch SL, Lane R (2003). Neurobiology of emotion perception II: implications for major psychiatric disorders. Biol Psychiatry 54: 515–528.
Rosin DL, Talley EM, Lee A, Stornetta RL, Gaylinn BD, Guyenet PG et al (1996). Distribution of alpha 2C-adrenergic receptor-like immunoreactivity in the rat central nervous system. J Comp Neurol 372: 135–165.
Roy A, Pickar D, De Jong J, Karoum F, Linnoila M (1988). Norepinephrine and its metabolites in cerebrospinal fluid, plasma, and urine. Relationship to hypothalamic–pituitary–adrenal axis function in depression. Arch Gen Psychiatry 45: 849–857.
Roy A, Pickar D, Linnoila M, Potter WZ (1985). Plasma norepinephrine level in affective disorders. Relationship to melancholia. Arch Gen Psychiatry 42: 1181–1185.
Rudorfer MV, Ross RJ, Linnoila M, Sherer MA, Potter WZ (1985). Exaggerated orthostatic responsivity of plasma norepinephrine in depression. Arch Gen Psychiatry 42: 1186–1192.
Schildkraut JJ (1965). The catecholamine hypothesis of affective disorders: a review of supporting evidence. Am J Psychiatry 122: 509–522.
Sheline YI, Barch DM, Donnelly JM, Ollinger JM, Snyder AZ, Mintun MA (2001). Increased amygdala response to masked emotional faces in depressed subjects resolves with antidepressant treatment: an fMRI study. Biol Psychiatry 50: 651–658.
Small KM, Mialet-Perez J, Seman CA, Theiss CT, Brown KM, Liggett SB (2004). Polymorphisms of cardiac presynaptic alpha2C adrenergic receptors: diverse intragenic variability with haplotype-specific functional effects. Proc Natl Acad Sci USA 101: 13020–13025.
Surguladze S, Brammer MJ, Keedwell P, Giampietro V, Young AV, Travis MJ et al (2005). A differential pattern of neural response toward sad versus happy facial expressions in major depressive disorder. Biol Psychiatry 57: 201–209.
Thomas KM, Drevets WC, Whalen PJ, Eccard CH, Dahl RE, Ryan ND et al (2001). Abnormal amygdala response to faces in anxious and depressed children. Arch Gen Psychiatry 58: 1057–1063.
Veith RC, Lewis N, Linares OA, Barnes RF, Raskind MA, Villacres EC et al (1994). Sympathetic nervous system activity in major depression. Basal and desipramine-induced alterations in plasma norepinephrine kinetics. Arch Gen Psychiatry 51: 411–422.
Whalen PJ, Rauch SL, Etcoff NL, McInerney SC, Lee MB, Jenike MA (1998). Masked presentations of emotional facial expressions modulate amygdala activity without explicit knowledge. J Neurosci 18: 411–418.
Wong ML, Kling MA, Munson PJ, Listwak S, Licinio J, Prolo P et al (2000). Pronounced and sustained central hyper-noradrenergic function in major depression with melancholic features: relation to hypercortisolism and corticotropin-releasing hormone. Proc Natl Acad Sci USA 97: 325–330.
Wyatt RJ, Portnoy B, Kupfer DJ, Snyder F, Engelman K (1971). Resting plasma catecholamine concentrations in patients with depression and anxiety. Arch Gen Psychiatry 24: 65–70.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was presented in part in abstract form at the 60th Annual Meeting of the Society of Biological Psychiatry, May 19–21, 2005, Atlanta, Georgia, USA.
Rights and permissions
About this article
Cite this article
Neumeister, A., Drevets, W., Belfer, I. et al. Effects of a α2C-Adrenoreceptor Gene Polymorphism on Neural Responses to Facial Expressions in Depression. Neuropsychopharmacol 31, 1750–1756 (2006). https://doi.org/10.1038/sj.npp.1301010
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.npp.1301010
Keywords
This article is cited by
-
Neurotransmitter, Peptide, and Steroid Hormone Abnormalities in PTSD: Biological Endophenotypes Relevant to Treatment
Current Psychiatry Reports (2018)
-
Test–retest reliability of 11C-ORM-13070 in PET imaging of α2C-adrenoceptors in vivo in the human brain
European Journal of Nuclear Medicine and Molecular Imaging (2015)
-
Facial emotion processing in major depression: a systematic review of neuroimaging findings
Biology of Mood & Anxiety Disorders (2011)
-
Neurocircuitry of Mood Disorders
Neuropsychopharmacology (2010)
-
Brain structural and functional abnormalities in mood disorders: implications for neurocircuitry models of depression
Brain Structure and Function (2008)
