
Abstract
This study aims to quantify changes in outdoor (ambient) air pollution exposure from different migration patterns within Peru and quantify its effect on premature mortality. Data on ambient fine particulate matter (PM2.5) was obtained from the National Aeronautics and Space Administration (NASA). Census data was used to calculate rates of within-country migration at the district level. We calculated differences in PM2.5 exposure between “current” (2016–2017) and “origin” (2012) districts for each migration patterns. Using an exposure-response relationship for PM2.5 extracted from a meta-analysis, and mortality rates from the Peruvian Ministry of Health, we quantified premature mortality attributable to each migration pattern. Changes in outdoor PM2.5 exposure were observed between 2012 and 2016 with highest levels of PM2.5 in the Department of Lima. A strong spatial autocorrelation of outdoor PM2.5 values (Moran’s I = 0.847, p-value=0.001) was observed. In Greater Lima, rural-to-urban and urban-to-urban migrants experienced 10-fold increases in outdoor PM2.5 exposure in comparison with non-migrants. Changes in outdoor PM2.5 exposure due to migration drove 185 (95% CI: 2.7, 360) premature deaths related to air pollution, with rural-urban producing the highest risk of mortality from exposure to higher levels of ambient air pollution. Our results demonstrate that the rural-urban and urban-urban migrant groups have higher rates of air pollution-related deaths.
Similar content being viewed by others
Introduction
Migration is increasingly recognized as an important determinant for population health1,2,3,4. Nowadays, more than 244 million international migrants are estimated globally5 with considerable gaps in health care services. Furthermore, a significantly larger number of internal migrants − people moving within their country of birth − has been documented4, with a particular health burden despite being nationals. Migrants are commonly exposed to a range of challenges such as low quality of labor conditions, massive vehicular traffic, sedentarism (low level of physical activity), lack of social support, limited access to healthy food choices6, and stress7,8. Social vulnerability from economic instability, social isolation, poor access to healthcare services, increased exposure to infectious diseases, and traumatic events related to the migration itself have also been known to affect migrants’ health9,10,11,12,13,14.
In addition to these stressors, migrants are exposed to new environments, which may have further impacts. Environmental changes and exposures have been studied as drivers of migration15,16,17, including how exposure to hazards or availability of ecosystem services can lead residents’ to migrate away from these harmful environments. Although there is abundant literature studying how environmental hazards can drive emigration, only one study conducted in the United States (U.S.) has investigated how migrants may also be at a differential risk for environmental exposures. Interestingly, this study found that international immigrants in the U.S. are generally less exposed to chemical toxins, while specific groups such as Mexican immigrants in high income areas have a disproportionate exposure18. To our knowledge, no study has considered exposure to outdoor (ambient) air pollution as an environmental health risk of concern for migrant populations.
Exposure to outdoor air pollution is one of the leading environmental causes of mortality globally19. The burden of air pollutants is 6.4 million years of life lost20. Most health effects of air pollution have been documented in respiratory diseases, cardiovascular diseases, allergenic diseases, and diabetes, affecting individuals throughout the life course from developing fetuses to elderly populations21. Particulate matter under 2.5 micrometers (PM2.5) is known to be one of the more harmful pollutants due to its ability to penetrate deep into the lungs and enter the bloodstream22. With major increases in urbanization and migration to urban centers worldwide, which have higher levels of air pollution and other environmental exposures, the potential health implications of these changes and burden of migrant populations merits attention23. The study of health exposures among migrants also needs to further characterize the different profiles of within country migrants, as recently exemplified in the case of obesity24.
As a country with a high rate of internal migration and high levels of particulate matter in some regions, Peru is a unique context to study this topic. After a period of the political violence (armed internal conflict during the 1970–1990’s)25 with approximately 120,000 displaced families from the Andes to the Capital city of Lima26, nowadays most rural-to-urban migration has been largely driven by economic reasons, to seek access to better services. However, slow process of formal land titles and rising property prices in Lima have led some recent migrants to poor housing conditions in shantytowns with lack of water or electricity supply27. These harmful conditions expose migrants to environmental determinants that can lead to health disparities, such as increasing labor hours and unexpected health seeking costs that greatly affect low-income populations and reinforce the poverty cycle and negative health outcomes.
Previous studies have reported the air pollution status in Peru and highlighted the important geographical variability of air contaminants28,29,30,31. In addition, several studies have shown the impact of rural-to-urban migration in Peru on infectious and non-communicable diseases32,33,34,35,36,37,38,39,40,41,42,43 driven by changes in diet and physical activity patterns, increased poverty, and restricted access to health care. However, limited literature addresses outdoor air pollution effects in the migrant population, and to our knowledge, no study has quantified the health burden associated with changes in exposure to ambient air pollution due to migration between different locations.
In this study, we aimed to quantify changes in outdoor air pollution exposure related to different internal migration patterns (rural-to-rural, rural-to-urban, urban-to-rural, and urban-to-urban) in Peru, identify spatial clusters where high rates of migrants and high levels of PM2.5 collide, and finally quantify the associated changes in premature mortality using a health impact assessment methodology.
Methods
Study area and population
This study was conducted in Peru for the 2012–2017 period. Administrative units in Peru are organized in 25 Departments (level 1), 196 provinces (level 2), and 1873 districts (level 3). Data encompasses information about 29,381,884 inhabitants in an area of 1,285,216 km2. Major ecological areas in the country were divided into the Coast, Andes, and Jungle (Fig. 1). This study used data at the smallest administrative level (districts), which were further classified as: districts of the capital (Greater Lima), big cities (population > 150,000), intermediate cities (pop. between 20,000–150,000), and small cities (pop. between <20,000).

Study area. Contrasting ecological areas (Coast, Andes, and Jungle) in Peru. Solid lines represent the 25 Departments (administrative level 1). Map was produced using QGIS 3.6.3 (QGIS Development Team, 2019. QGIS Geographic Information System. Open Source Geospatial Foundation Project. http://www.qgis.osgeo.org/). Map tiles by OpenTopoMap (Kartendaten: © OpenStreetMap-Mitwirkende, SRTM | Kartendarstellung: © OpenTopoMap; http://www.opentopomap.org) under creative common licence CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0/).
Data sources
Migration rate
Census data was provided by the National Institute of Statistics and Informatics (INEI in Spanish) via the REDATAM platform. Information from the 2017 Census was used to calculate within-country migration rates. In the census, all inhabitants were asked to report the district where they are currently living (2016–2017), henceforth referred to as “current district” and the district where they lived 5 years ago (2012), henceforth referred to as “origin district”. Children under 5 were excluded from this question. In addition, international migrants − people with a country of birth different than Peru − were excluded to analyze only within-country migration. After exclusion criteria, the information of 26,779,984 (91%) inhabitants was analyzed.
For this study, non-migrants were defined as population that reported the same origin and current district and migrants were defined as population for which the origin and current district differed. Origin and current districts were labeled as rural or urban according to the INEI National registry classification and rural-to-rural, rural-to-urban, urban-to-rural, and urban-to-urban migration status were constructed. The distribution of districts relative to rural/urban category and city type is presented in Supplementary Table 1.
For each of the 1873 districts the number of non-migrants, immigrants (with details on origin districts) and out-migrants (with details on destination districts) were computed. The migration rate was calculated as the number of migrants (immigrants or out-migrants independently) in each district divided by the total population in the same district. Standardized migration rates were calculated by multiplying the migration rate by the proportion of population in each district in 2017 (district population/country population). REDATAM exported data were formatted and processed using R software v.3.6.2 (R Core Team (2019). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org).
Air quality
Particulate matter with a diameter less than 2.5 micrometers, PM2.5, was used a measure of outdoor air pollution in this study given the strong evidence of its effects on adverse health outcomes44,45. Air quality data from the NASA - Socioeconomic Data and Applications Center (SEDAC) was used46. SEDAC provided an annual global surface of concentrations (micrograms per cubic meter - µg/m3) of mineral dust and sea-salt filtered PM2.546,47. Although PM2.5 predictions using ground measurements and chemical transport models in addition to satellite data have been reported recently for Peru that are likely more accurate48, this data was only available for Lima (the capital) preventing comparisons between rural and urban settings. Previous studies47 demonstrated that SEDAC-NASA data were highly consistent (R2 = 0.81) with out-of-sample cross-validated PM2.5 concentrations from ground stations in the Global Burden of Disease (GBD) network49.
As a result, PM2.5 gridded data sets were provided at a spatial resolution of 0.01 degrees46. Most proximate datasets to the study period were used for the analysis, 2012 and 2016. We harmonized migration and air quality data at the same spatial scale, by estimating the median PM2.5 (SEDAC gridded data) at each district. Spatial boundaries of the 1873 districts were obtained from the National Institute of Geography (IGN in Spanish). Data was provided in shapefile format with tolerances of 1,000 m and 1,000,000 m2.
Data processing was conducted in Google Earth Engine (GEE)50. SEDAC dataset and IGN shapefiles were uploaded to GEE as assets. For data visualization purposes, districts were classified in 6 categories according the levels of PM2.5 in micrograms per cubic meter (<10, 10–15, 15–20, 20–25, 25–30, >30) relative to the WHO air quality guideline51.
Baseline mortality and exposure-response data
Mortality data (all causes) was collected at the departmental-level from the national center of epidemiology, prevention and control of disease of the Ministry of Health of Peru52. Each district was assigned the mortality rate for the department which it is nested.
The exposure-response relationship for PM2.5 was extracted from a review conducted by Hoek et al. (2013) which conducted a meta-analysis on cardio-respiratory mortality from air pollution exposure from epidemiological studies around the globe53. The overall estimate for all-cause mortality of 1.06 (95% CI: 1.04, 1.08) per 10 μg/m3 increase in PM2.5 exposure was used.
Spatial analysis between PM2.5and migration
To determine the spatial dependence of PM2.5 concentration and its association with migration status, spatial autocorrelation analyses and a spatial Bayesian regression were conducted. First, to determine the spatial autocorrelation of PM2.5, meaning that the values of PM2.5 in each district is influenced by the values of PM2.5 on their neighborhood districts, a Global Moran’s I and Local Getis-Ord Gi* statistics were calculated using a first-order queen contiguity-based weighted neighborhood. The statistic under the null hypothesis of spatial randomness was calculated by randomly permuting the observed values over the locations. The z-distribution was computed based on spatial random data sets (the permuted data sets). No statistical testing was applied over the Gi* statistic to prevent bias due to multiple and dependent tests54,55. Clusters were categorized based on the Gi* statistic sign in high- (hotspot) or low- (coldspot) concentration areas and percentile (90%, 95%, 99%) of the z-distribution. Then the migration rates in each PM2.5 cluster were analyzed.
To assess the relation between migration status (independent variable) and ‘change in PM2.5 exposure’ defined as the difference in PM2.5 between 2012 and 2016 (dependent variable) accounting for the spatial structure of the districts in Peru, a Bayesian linear model was fitted using Integrated Nested Laplace Approximation (INLA, www.r-inla.org)56 for all districts in Peru (1873). A spatial model was formulated by including a spatial structure using a convolution prior that combined area-specific overdispersion and a neighborhood dependency structure57,58. See S1 supplementary methods for specification of prior and hyper-prior distributions.
Quantifying attributable mortality
We used a Health Impact Assessment (HIA) methodology to quantify mortality attributable to change in PM2.5 caused by internal migration. HIAs have been used to quantify the mortality or morbidity associated with air pollution in various regions59,60 and are a standard tool to quantify the global burden of disease. These are based on exposure-response functions (ERF) for particulate matter obtained from epidemiological studies and can be extrapolated to a population to understand the burden and inform environmental policies61.
We first estimated changes in outdoor air pollution exposure due to migration by calculating the difference for each district to district migration (“current” and “origin”) in the year 2016 after truncating the PM2.5 estimates for the “current” and “origin” districts at the 5th/95th percentile. This represents the counterfactual scenario in which a migrant had not migrated and remained in the same district and therefore exposed to PM2.5 in the origin district.
We calculated a relative risk of the exposure by multiplying the change in PM2.5 between “current” and “origin” district by the ln(ERF) and exponentiating this product. An attributable fraction (AF) was then estimated applying the following equation to the relative risk of the exposure [RR-1/RR]. This AF was then multiplied by the all-cause mortality rate for each department in which the “current” district was nested to calculate the mortality rate attributable to change in PM2.5 exposure. The “current” department mortality rate was used for analysis to account for potential changes in baseline mortality between departments, to focus only on changes in outdoor air pollution exposure. For example, for those migrants that lived in Chachapoyas, Amazonas in 2012 and moved to Chorrillos, Lima in 2016, an ambient air pollution difference was considered at the district-level by considering the change in exposure between Chachapoyas and Chorrillos. This difference in ambient air pollution exposure was then used to calculate attributable fraction which was multiplied by the mortality rate for the department of Lima which was considered homogenous and therefore assigned to the district of Chorrillos. This was considered the excess mortality for this migrant group, and differences were calculated for each migration pattern and weighted by the number of individuals that undertook this migration route to calculate average mortality rates from air pollution exposure attributable to migration. Finally, overall number of attributable deaths were calculated by taking into account the number of migrants that undertook each district-district route. 95% Confidence intervals were computed by calculating the attributable mortality based on variability of the PM2.5 ERF. All analyses were stratified by urbanicity of the origin and current district (rural-rural, urban-urban, rural-urban, urban-rural) and by department (using the migrants’ “current” department) to consider variation in risk spatially and by migration pattern.
Results
Spatial distribution of PM2.5
Important changes in PM2.5 were observed between 2012 and 2016 in the entire country (Fig. 2). Higher levels of PM2.5 were observed in the Department of Lima, southern coast, and in the Amazon Region (Fig. 2). The average PM2.5 levels were highly heterogeneous across city categories (Greater Lima, big, intermediate, and small cities, and rural areas). The highest average PM2.5 was located in Greater Lima with more than 4-folds higher in comparison with rural areas (Table 1).

Country-wide spatial distribution of PM2.5 (μg/m3) at 0.01 degrees (~1.11 km). Estimates provided by NASA-SEDAC for 2012 (left) and 2016 (right). Maps were produced using R software v.3.6.2 (R Core Team (2019). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/). based on NASA-SEDAC data (https://sedac.ciesin.columbia.edu/data/set/sdei-global-annual-gwr-pm2–5-modis-misr-seawifs-aod).
Spatial distribution of migration rates
The district-level migration rate showed a scattered spatial pattern, however most migrants arrived to Greater Lima (Province of Lima) (Fig. 3 - left), which is also the city with the lowest out-migration in the country (Fig. 3 - right). The jungle and Andes are areas with low immigration and high out-migration rates, as opposed to what is observed in the coastal areas (Fig. 3). Interestingly, the 43 districts that make up Greater Lima received two-fold the migrant population (1,242,834 migrants) than small cities that make up 1,633 districts (581,738 migrants). The detailed distribution relative to the type of migration and city category is shown in Table 1. For rural-to-urban migrants, Greater Lima and Intermediate cities were the most important harboring places, and for urban-to-urban migrants as well.

Spatial distribution of migration rates (2012–2016 period) at district-level in Peru. Standardized migration rates per 100,000 habitants for immigrants (left) and out-migrants (right). Maps were produced using R software v.3.6.2 (R Core Team (2019). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/).
Change in PM2.5 exposure by migration status
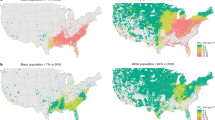
Larger changes in the PM2.5 exposure were observed in migration in comparison to non-migrants which only experienced a change in PM2.5 exposure due to environmental and social changes within the same district over time (Fig. 4A). Most (68%) of those exposed to high outdoor air pollution (PM2.5 > 30 μg/m3) were migrants from districts with a lower PM2.5 concentration. In Greater Lima, rural-to-urban and urban-to-urban migrants experienced 10-fold increases in PM2.5 exposure in comparison to non-migrants (Fig. 4B). Conversely, urban-to-rural and urban-to-urban migrants in small and intermediate cities were exposed to lower levels of PM2.5 in their receiving districts.

Exposure to PM2.5 in migrants and non-migrants in Peru. (A) Change in exposure to PM2.5 between origin and current districts of migrants, and between exposure in 2012 and 2016 in non-migrants. Districts were classified at 6 levels of exposure in micrograms per cubic meter (μg/m3) (dark blue: <10, blue: 10–15, light blue: 15–20, light orange: 20–25, orange: 25–30, red:>30). (B) Net difference in exposure to PM2.5 relative to type of migration (no migration, rural-to-rural, rural-to-urban, urban-to-rural, and urban-to-urban) and category of city (Greater Lima, big, intermediate and small cities). Figures were produced using R software v.3.6.2 (R Core Team (2019). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/).
Spatial analysis between PM2.5 and migration
An overall strong spatial autocorrelation of PM2.5 values (Moran’s I = 0.847, p-value=0.001) was observed in the study area (Fig. 5A). All detected hotspots clusters were located in the coastal areas of the country. As expected, the largest hotspot was located in the Province of Lima, however scattered hotspots in the southern and northern coast were also detected. Major coldspot clusters were located in the Andean Region (Fig. 5B). Overall, the average rural-to-urban and urban-to-urban migration rates was higher in PM2.5 hotspots than coldspots (Fig. 5C). Conversely, the average rural-to-rural and urban-to-rural migration rates was lower in PM2.5 hotspots than coldspots (Fig. 5C).

Spatial autocorrelation of PM2.5. (A) Global Moran’s I and. (B) Local Getis-Ord Gi* (right). (C) Standardized migration rates in clusters of PM2.5 relative to type of migration (no migration, rural-to-rural, rural-to-urban, urban-to-rural, and urban-to-urban). Clusters of PM2.5 were categorized based on the Gi* statistic sign in high- (hotspot) or low- (coldspot) concentration areas and percentile (90%, 95%, 99%) of the z-distribution. Maps and figures were produced using R software v.3.6.2 (R Core Team (2019). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/).
Using a Bayesian spatial model, we found that rural-to-urban migration patterns were associated with an increase in 9.88 µg/m3 (Credible Interval = 9.26, 10.51) of PM2.5 exposure when comparing exposure in the current to the origin district (Table 2). Conversely, notable reduction in PM2.5 exposure was observed for urban-to-rural migrants (Median = −8.36; 95% CI = −8.99: −7.74). Finally, moderate changes were observed for rural-to-rural and urban-to-urban migrants (Table 2).
Change in PM2.5 exposure and burden by migration status
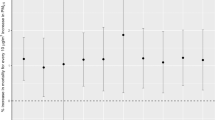
Overall, we found that migration drove an additional 185 (95% CI: 2.7, 360) deaths related to outdoor air pollution exposure across Peru from 2012 to 2016. When considering only those that migrate from a rural-to-urban setting, there is an increase in 87 (95% CI: 59, 114) deaths related to outdoor air pollution. The largest migrant group, urban-to-urban, resulted in an increase in 120 (95% CI: -24, 259) ambient air pollution-related deaths, the smallest migrant group, rural to rural, results in 0.56 (0.01, 1.1) additional deaths. There is a decrease in number of deaths for migrants going from an urban to rural setting, with -23 (95% CI: -32, -14) fewer deaths; this is one of the smaller groups, along with rural-rural migration. Mortality rates show similar results, with rural-urban revealing the greatest change in mortality rate and rural-rural migrants showing little change (Fig. 6). When considering the attributable deaths by migrants’ “current” department in 2016, it is apparent that migration to Lima is the main driver of outdoor air pollution related mortality from migration, where 229 deaths (95% CI: 143, 311) occur, while the majority of the other departments show decreases in outdoor air pollution-related mortality for migrants (Supplementary Table 2).

Graph showing difference in mortality rate (per million) and 95% confidence intervals related to air pollution exposure change from migration by migrant type.
Discussion
The substantial growth of internal human population mobility in low and middle income countries is changing population distributions across geographical areas, with subsequent changes in environmental exposures including air pollution, which fosters a need to study potential health implications in this setting. Migrants are a particularly vulnerable group in this context as they are moving to areas with higher or worse environmental risk profiles, often driven by economic, socio-political or geographical motives62. Besides changes in customs and risk behaviors, migrants also experience a change in environment. This study showed the first evidence of the relationship between changes in outdoor air pollution (PM2.5) exposure and burden related to migration status. Remarkable clustering patterns were observed in the spatial distribution of PM2.5 and migration rates. These distributions are spatially correlated in densely urban areas. This study highlights that rural-to-urban migrants experience a transition to environments with more deleterious ambient air pollution levels with a higher mortality burden, which adds to other previously reported socio-economic disadvantages. This demonstrates that even a slight increase in outdoor air pollution exposure associated with migration can have large impacts on population health, particularly when large groups are moving to environments with higher outdoor air pollution concentrations. The results of this study are important, because 1) it is the first study to quantify the effect of outdoor air pollution exposure on migrants health, and 2) it allows an understanding mobility and exposure patterns in Peru that can be integrated into urban planning policies to protect vulnerable populations.
Previous studies in China63 and the United States64 have argued that environmental inequalities may be shaped by social mechanisms such as residential segregation and racial income inequality. These same mechanisms were hypothesized in this study. In Greater Lima, the city that harbor most internal immigrants, the highest levels of PM2.5 are located in districts with the lowest average income. Albeit less marked than observed with PM2.5, districts with the highest migration rates are concurrently the most impoverished areas. Recent studies characterized the Peruvian internal migrants as primarily low-income population24,65, similar to other studies worldwide66,67. Taken together, the evidence points to the fact that the main mechanisms that drive migration and consequently higher PM2.5 exposure levels and burden are poverty and seeking of economic and educational opportunities. Many low-income rural populations are migrating to deleterious urban environments seeking better economic and educational opportunities but are exposed to much higher levels of PM2.5 and increased mortality risk. By identifying Lima as the department in Peru that far exceeds outdoor air pollution-related mortality burden for migrants, it can be considered a priority area for targeted ambient air pollution control measures, particularly for migrating populations.
Previous studies have described the effects of PM2.5 in non-communicable diseases (NCD), and respiratory diseases68. In Peru, increased risk of asthma68,69 and influenza70 were described in urban cities and migrant population, mediated by high values of PM2.5. Conditions such as soil organic matter, industry, and traffic have been suggested as drivers to the increased outdoor air pollution level which is attributed as a major determinant to the quality of life in the megacity of Lima71. As portrayed in the spatial analysis, hotspots of ambient air pollution are located on the coast of the country. Furthermore, these areas are located near main ports and heavily industrialized areas. These findings urge for new environmental health strategies to control these detrimental conditions. This study was able to exploit the different migration patterns and its associated health burden driven by changes in ambient air pollution exposure. Political commitment to address these issues will have a positive effect in reducing environmental-related health outcomes and the social and environmental gap observed in the migrant population.
This study is the first to describe a positive relation between internal migration and ambient air pollution exposure, and quantify the associated burden. Is important to mention that the social structure and social capital is also altered in the migrant population72. These conditions may deter the response capacity of the migrant population to affront environmental hazards for which recent migrants are exposed. However, it is important to acknowledge that migrants, and particularly those moving from rural to urban areas, may also experience increased economic opportunities and accessibility to healthcare. For example, financial reasons and other motivations related to improving people’s well-being is a strong driver of out-migration which may have a positive impact on the overall health of the migrant62. Although there are some nuances in the health effects of migration, it was beyond the scope of this study to consider these other factors, as the main purpose of this study was to quantify the outdoor air pollution-related health burden. Ultimately, it is well established that migrant populations in Peru are highly vulnerable to diseases due to environmental, social, and economic frailty24,37, and ambient air pollution exposure adds to this existing burden.
This manuscript focuses specifically on changes in outdoor ambient air pollution. However, indoor pollution from different sources such as cookstoves, is also a major health concern in Peru and globally73,74,75,76,77,78. Migration from rural to urban areas for example may have a beneficial effect on exposure to indoor air pollution due to changes in cooking fuels. Although we did not have access to such data, previous studies in Peru have found that indoor biomass stove can increase exposure to polycyclic aromatic hydrocarbons and particulate matter74,79. Additionally, while these are two different sources of exposure, interventions aimed at reducing residential wood burning have also been shown to reduce outdoor particulate matter concentrations showing important health benefits80.
Additional work could expand the exploration of other drivers of health and health changes, particularly for migrant populations, including other environmental exposures, potential positive changes in accessibility to healthcare and services as well as changes in PM2.5 exposure related to other internal migrant groups or external migration. However, in comparison to refugee migration, internal migration can be more precisely estimated81 due to the fact that mechanisms that influence internal migration follow long-term trends. However, the technical challenges to harmonize temporal and spatial data of internal displacements often prevents accurate quantification of internal migrants1,67. Furthermore, limited evidence showed the impact of internal migration on exposure to deleterious environments. The spatial autocorrelation analysis in this study has shown the large spatial effects in the relation between migration and PM2.5. These spatial effects might be due to social, economic, environmental (topological), or behavioral characteristics in the districts that receive the most migrants. This elucidates important evidence that geographically targeted interventions may have a great impact at the macro- and micro- scales.
Several limitations should be acknowledged in this study. First, migration estimates were computed based on whether the participant lived in the same district five years before. This cutoff is based on the census questionnaire and may represent a threat to consistency, due to the wide range from 5 years before to recent migrants (~1 day). Second, there is no question to check if participants are currently living in a permanent or temporary household, thus we cannot ascertain if they had a chronic exposure to these levels of outdoor air pollution. In the same way, migrants may arrive at a different place than where they were interviewed, and thus they may carry over the environmental exposures of all previous places where they had been settled that may yield to exposure misclassification. Third, as detected in the high-resolution images (Fig. 2 for reference), high variability of outdoor air pollution was observed within each district. Due to the lack of spatial resolution of migration status, ambient air pollution data was aggregated at the district level to be harmonized with migration data. This may yield biased conclusions due to PM2.5 and migration being non-stationary processes within districts. Further studies are suggested that account for fine-scale estimation of the relationship between migration and outdoor air pollution exposure. Also, despite residency exposure being a standard measure for ambient air pollution, this does not account for total exposure to air pollutants. This study did not include the exposure during work or leisure activities due to the lack of this data in the census. Additionally, we assumed a exposure-response relationship of PM2.5 based on existing literature on long-term effects of particulate matter based on studies primarily conducted in North America and Europe, while the true relationship may be different in the Peruvian context. However, the risk would be likely to be an underestimation as the majority of studies in the meta-analysis were from North America or Europe while impacts have been shown to be higher in Peru and other underrepresented countries82. Lastly, the baseline mortality rate considered for calculating attributable mortality risk was available only at the departmental level, therefore we had to assume homogeneity in mortality rates for districts within each department.
Conclusion
This study was able to demonstrate the effect of migration on change in exposure to air pollution and quantify the mortality burden from this change. The clustered co-occurrence of high values of migration and PM2.5 suggest this relation might be shaped also by social and economic inequalities. Results suggest that internal migration in Peru drives an increase in mortality from air pollution exposure, with rural-urban migrants as one of the most vulnerable migrant groups, as well as the most prevalent. The findings of this study may represent the first steps to tailor strategies to improve the health of vulnerable populations such as internal migrants. Additionally, our results demonstrate the importance of considering air pollution as an environmental risk factors when studying migrant health in Peru and beyond.
Data availability
Census data was provided by the National Institute of Statistics and Informatics (INEI in Spanish) via the REDATAM platform available in http://censos2017.inei.gob.pe/redatam/. Air pollution data (PM2.5) was provided by the NASA - Socioeconomic Data and Applications Center (SEDAC) available in https://sedac.ciesin.columbia.edu/data/set/sdei-global-annual-gwr-pm2–5-modis-misr-seawifs-aod.
Change history
24 November 2020
An amendment to this paper has been published and can be accessed via a link at the top of the paper.
References
Hanefeld, J. et al. A global research agenda on migration, mobility, and health. The Lancet 389, 2358–2359 (2017).
McKay, L., Macintyre, S. & Ellaway, A. Migration and health: a review of the international literature. (2003).
Bhopal, R. Unity in the fields of migration, ethnicity, race and health. Lancet Public Health 3, e13 (2018).
Wickramage, K., Vearey, J., Zwi, A. B., Robinson, C. & Knipper, M. Migration and health: a global public health research priority. BMC Public Health 18, 987 (2018).
McAuliffe, M. & Ruhs, M. World Migration Report 2018. Geneva Int. Organ. Migr. (2017).
Ebrahim, S. et al. The Effect of Rural-to-Urban Migration on Obesity and Diabetes in India: A Cross-Sectional Study. PLOS Med. 7, e1000268 (2010).
Delavari, M., Sønderlund, A. L., Swinburn, B., Mellor, D. & Renzaho, A. Acculturation and obesity among migrant populations in high income countries – a systematic review. BMC Public Health 13, 458 (2013).
Jackson, S. E., Kirschbaum, C. & Steptoe, A. Hair cortisol and adiposity in a population-based sample of 2,527 men and women aged 54 to 87 years. Obes. Silver Spring Md 25, 539–544 (2017).
Anikeeva, O. et al. The health status of migrants in Australia: a review. Asia. Pac. J. Public Health 22, 159–193 (2010).
Bradby, H., Humphris, R., Newall, D. & Phillimore, J. Public health aspects of migrant health: a review of the evidence on health status for refugees and asylum seekers in the European Region. (2015).
Brandenberger, J., Tylleskär, T., Sontag, K., Peterhans, B. & Ritz, N. A systematic literature review of reported challenges in health care delivery to migrants and refugees in high-income countries - the 3C model. BMC Public Health 19, 755 (2019).
Gushulak, B. D. & MacPherson, D. W. The basic principles of migration health: population mobility and gaps in disease prevalence. Emerg. Themes Epidemiol. 3, 3 (2006).
Juárez, S. P. et al. Effects of non-health-targeted policies on migrant health: a systematic review and meta-analysis. Lancet Glob. Health 7, e420–e435 (2019).
Matlin, S. A., Depoux, A., Schütte, S., Flahault, A. & Saso, L. Migrants’ and refugees’ health: towards an agenda of solutions. Public Health Rev. 39, 27 (2018).
Black, R. et al. The effect of environmental change on human migration. Glob. Environ. Change 21, S3–S11 (2011).
Hunter, L. M. Migration and Environmental Hazards. Popul. Environ. 26, 273–302 (2005).
Qin, Y. & Zhu, H. Run away? Air pollution and emigration interests in China. J. Popul. Econ. 31, 235–266 (2018).
Bakhtsiyarava, M. & Nawrotzki, R. J. Environmental Inequality and Pollution Advantage among Immigrants in the United States. Appl. Geogr. Sevenoaks Engl. 81, 60–69 (2017).
Health Effects Institute. State of Global Air 2019. (Health Effects Institute, 2019).
Cohen, A. J. et al. The global burden of disease due to outdoor air pollution. J. Toxicol. Environ. Health A 68, 1301–1307 (2005).
Mannucci, P. M., Harari, S., Martinelli, I. & Franchini, M. Effects on health of air pollution: a narrative review. Intern. Emerg. Med. 10, 657–662 (2015).
Kampa, M. & Castanas, E. Human health effects of air pollution. Environ. Pollut. Barking Essex 1987 151, 362–367 (2008).
Abubakar, I. et al. The UCL–Lancet Commission on Migration and Health: the health of a world on the move. The Lancet 392, 2606–2654 (2018).
Najera, H., Nandy, S., Carrillo-Larco, R. M. & Miranda, J. J. Within-country migration and obesity dynamics: analysis of 94,783 women from the Peruvian demographic and health surveys. BMC Public Health 19, 263 (2019).
Reátegui Carrillo, F., Ciurlizza Contreras, J. & Peralta Ytajashi, A. Hatun Willakuy. Versión abreviada del Informe Final de la Comisión de la Verdad y Reconciliación. (Pontificia Universidad Católica del Perú. Instituto de Democracia y Derechos …, 2004).
Coral, I. Desplazamiento por violencia política en el Perú, 1980-1992. (1994).
Chan, L. Rapid Rural-to-Urban Migration to Lima: A Need for a Sustainable Housing Reform. Vol. 35 - Leveraging Perus Econ. Potential 2017 (2017).
Han, X. et al. Traffic-related Occupational Exposures to PM2.5, CO, and VOCs in Trujillo, Peru. Int. J. Occup. Environ. Health 11, 276–288 (2005).
Pearce, J. L., Rathbun, S. L., Aguilar-Villalobos, M. & Naeher, L. P. Characterizing the spatiotemporal variability of PM2.5 in Cusco, Peru using kriging with external drift. Atmos. Environ. 43, 2060–2069 (2009).
Romieu, I., Weitzenfeld, H. & Finkelman, J. Urban Air Pollution in Latin America and the Caribbean. J. Air Waste Manag. Assoc. 41, 1166–1171 (1991).
Tashiro, Y. & Taniyama, T. Atmospheric NO2 and CO concentration in Lima, Peru. Environ. Int. 28, 227–233 (2002).
Miranda, J. J., Gilman, R. H., García, H. H. & Smeeth, L. The effect on cardiovascular risk factors of migration from rural to urban areas in Peru: PERU MIGRANT Study. BMC Cardiovasc. Disord. 9, 23 (2009).
Mola, C. Lde et al. Body Mass Index and Self-Perception of Overweight and Obesity in Rural, Urban and Rural-to-Urban Migrants: PERU MIGRANT Study. PLOS ONE 7, e50252 (2012).
Miranda, J. J., Gilman, R. H. & Smeeth, L. Differences in cardiovascular risk factors in rural, urban and rural-to-urban migrants in Peru. Heart Br. Card. Soc. 97, 787–796 (2011).
Antiporta, D. A., Smeeth, L., Gilman, R. H. & Miranda, J. J. Length of urban residence and obesity among within-country rural-to-urban Andean migrants. Public Health Nutr. 19, 1270–1278 (2016).
Lazo-Porras, M. et al. Low HDL cholesterol as a cardiovascular risk factor in rural, urban, and rural-urban migrants: PERU MIGRANT cohort study. Atherosclerosis 246, 36–43 (2016).
Burroughs Pena, M. S. et al. Migration, urbanisation and mortality: 5-year longitudinal analysis of the PERU MIGRANT study. J. Epidemiol. Community Health 69, 715–718 (2015).
Carrillo-Larco, R. M. et al. Obesity risk in rural, urban and rural-to-urban migrants: prospective results of the PERU MIGRANT study. Int. J. Obes. 2005 40, 181–185 (2016).
Masterson Creber, R. M., Smeeth, L., Gilman, R. H. & Miranda, J. J. Physical activity and cardiovascular risk factors among rural and urban groups and rural-to-urban migrants in Peru: a cross-sectional study. Rev. Panam. Salud Publica Pan Am. J. Public Health 28, 1–8 (2010).
Bernabe-Ortiz, A. et al. Rural-to-urban migration and risk of hypertension: longitudinal results of the PERU MIGRANT study. J. Hum. Hypertens. 31, 22–28 (2017).
Gonzales, I. et al. Seizures, cysticercosis and rural-to-urban migration: the PERU MIGRANT study. Trop. Med. Int. Health TM IH 20, 546–552 (2015).
Taype-Rondan, A. et al. Smoking and heavy drinking patterns in rural, urban and rural-to-urban migrants: the PERU MIGRANT Study. BMC Public Health 17, 165 (2017).
Carrillo-Larco, R. M. et al. Cohort Profile: The PERU MIGRANT Study-A prospective cohort study of rural dwellers, urban dwellers and rural-to-urban migrants in Peru. Int. J. Epidemiol. 46, 1752–1752f (2017).
Atkinson, R. W., Kang, S., Anderson, H. R., Mills, I. C. & Walton, H. A. Epidemiological time series studies of PM2.5 and daily mortality and hospital admissions: a systematic review and meta-analysis. Thorax 69, 660–665 (2014).
Xing, Y.-F., Xu, Y.-H., Shi, M.-H. & Lian, Y.-X. The impact of PM2.5 on the human respiratory system. J. Thorac. Dis. 8, E69-E74–E74 (2016).
van Donkelaar, A. et al. Global Annual PM2. 5 Grids from MODIS MISR and SeaWiFS Aerosol Optical Depth (AOD) with GWR 1998–2016. NASA Socioecon. Data Appl. Cent. SEDAC (2018).
van Donkelaar, A. et al. Global Estimates of Fine Particulate Matter using a Combined Geophysical-Statistical Method with Information from Satellites, Models, and Monitors. Environ. Sci. Technol. 50, 3762–3772 (2016).
Vu, B. N. et al. Developing an Advanced PM2.5 Exposure Model in Lima, Peru. Remote Sens. 11 (2019).
Brauer, M. et al. Ambient Air Pollution Exposure Estimation for the Global Burden of Disease 2013. Environ. Sci. Technol. 50, 79–88 (2016).
Gorelick, N. et al. Google Earth Engine: Planetary-scale geospatial analysis for everyone. Remote Sens. Environ. 202, 18–27 (2017).
World Health Organization. Air quality guidelines: global update 2005: particulate matter, ozone, nitrogen dioxide, and sulfur dioxide. (World Health Organization, 2006).
Ministerio de Salud del Peru. Análisis de las causas de mortalidad en el Perú, 1986 − 2015. https://www.gob.pe/institucion/minsa/informes-publicaciones/279665-analisis-de-las-causas-de-mortalidad-en-el-peru-1986-2015.
Hoek, G. et al. Long-term air pollution exposure and cardio- respiratory mortality: a review. Environ. Health Glob. Access Sci. Source 12, 43 (2013).
Benjamini, Y. & Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple. Testing. J. R. Stat. Soc. Ser. B Methodol. 57, 289–300 (1995).
Caldas de Castro, M. & Singer, B. H. Controlling the False Discovery Rate: A New Application to Account for Multiple and Dependent Tests in Local Statistics of Spatial Association. Geogr. Anal. 38, 180–208 (2006).
Rue, H., Martino, S. & Chopin, N. Approximate Bayesian Inference for Latent Gaussian Models by Using Integrated Nested Laplace Approximations. J. R. Stat. Soc. Ser. B Stat. Methodol. 71, 319–392 (2009).
Besag, J., Green, P., Higdon, D. & Mengersen, K. Bayesian Computation and Stochastic Systems. Stat. Sci. 10, 3–41 (1995).
Lowe, R. et al. Nonlinear and delayed impacts of climate on dengue risk in Barbados: A modelling study. PLOS Med. 15, e1002613 (2018).
Boldo, E. et al. Apheis: Health Impact Assessment of Long-Term Exposure to $\text{PM}_{2.5}$ in 23 European Cities. Eur. J. Epidemiol. 21, 449–458 (2006).
Künzli, N. et al. Public-health impact of outdoor and traffic-related air pollution: a European assessment. Lancet Lond. Engl. 356, 795–801 (2000).
Krzyzanowski, M., Cohen, A. & Anderson, R. Quantification of health effects of exposure to air pollution. Occup. Environ. Med. 59, 791–793 (2002).
Hear, N. V., Bakewell, O. & Long, K. Push-pull plus: reconsidering the drivers of migration. J. Ethn. Migr. Stud. 44, 927–944 (2018).
Schoolman, E. D. & Ma, C. Migration, class and environmental inequality: Exposure to pollution in China’s Jiangsu Province. Ecol. Econ. 75, 140–151 (2012).
Downey, L., Dubois, S., Hawkins, B. & Walker, M. Environmental Inequality in Metropolitan America. Organ. Environ. 21, 270–294 (2008).
Milan, A. & Ho, R. Livelihood and migration patterns at different altitudes in the Central Highlands of Peru. Clim. Dev. 6, 69–76 (2014).
Royuela, V. & Ordóñez, J. Internal migration in a developing country: A panel data analysis of Ecuador (1982–2010). Pap. Reg. Sci. 97, 345–367 (2018).
Bell, M. et al. Internal Migration and Development: Comparing Migration Intensities Around the World. Popul. Dev. Rev. 41, 33–58 (2015).
Romero, K. et al. Role of Socio-Economic Status as a Modifier of Air Pollution and Asthma Control in a Population-Based Cohort of Peruvian Children. in A16. Air Pollution And Pediatric Asthma A1022–A1022, 10.1164/ajrccm-conference.2018.197.1_MeetingAbstracts.A1022 (American Thoracic Society, 2018).
Robinson, C. L. et al. The Peru Urban versus Rural Asthma (PURA) Study: methods and baseline quality control data from a cross-sectional investigation into the prevalence, severity, genetics, immunology and environmental factors affecting asthma in adolescence in Peru. BMJ Open 2, e000421 (2012).
Tinoco, Y. O. et al. Burden of Influenza in 4 Ecologically Distinct Regions of Peru: Household Active Surveillance of a Community Cohort, 2009–2015. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 65, 1532–1541 (2017).
Bose, S. et al. Association of traffic air pollution and rhinitis quality of life in Peruvian children with asthma. PloS One 13, e0193910 (2018).
Loret de Mola, C. et al. The effect of rural-to-urban migration on social capital and common mental disorders: PERU MIGRANT study. Soc. Psychiatry Psychiatr. Epidemiol. 47, 967–973 (2012).
Helen, G. S. et al. Exposure of Pregnant Women to Cookstove-Related Household Air Pollution in Urban and Periurban Trujillo, Peru. Arch. Environ. Occup. Health 70, 10–18 (2015).
Li, Z. et al. Biomonitoring Human Exposure to Household Air Pollution and Association with Self-reported Health Symptoms – A Stove Intervention Study in Peru. Environ. Int. 97, 195–203 (2016).
Siddharthan, T. et al. Association between Household Air Pollution Exposure and Chronic Obstructive Pulmonary Disease Outcomes in 13 Low- and Middle-Income Country Settings. Am. J. Respir. Crit. Care Med. 197, 611–620 (2018).
Martin, W. J. et al. Household Air Pollution in Low- and Middle-Income Countries: Health Risks and Research Priorities. PLoS Med. 10, (2013).
Gajate-Garrido, G. The Impact of Indoor Air Pollution on the Incidence of Life Threatening Respiratory Illnesses: Evidence from Young Children in Peru. J. Dev. Stud. 49, 500–515 (2013).
Hartinger, S. M. et al. Improving household air, drinking water and hygiene in rural Peru: a community-randomized–controlled trial of an integrated environmental home-based intervention package to improve child health. Int. J. Epidemiol. 45, 2089–2099 (2016).
Commodore, A. A. et al. A Pilot Study Characterizing Real Time Exposures to Particulate Matter and Carbon Monoxide from Cookstove Related Woodsmoke in Rural Peru. Atmospheric Environ. Oxf. Engl. 1994 79 (2013).
Bailey, J., Gerasopoulos, E., Rojas-Rueda, D. & Benmarhnia, T. Potential health and equity co-benefits related to the mitigation policies reducing air pollution from residential wood burning in Athens, Greece. J. Environ. Sci. Health Part A Tox. Hazard. Subst. Environ. Eng. 54, 1144–1151 (2019).
Raleigh, C., Jordan, L. & Salehyan, I. Assessing the impact of climate change on migration and conflict. in Paper commissioned by the World Bank Group for the Social Dimensions of Climate Change workshop, Washington, DC 5–6 (2008).
Cohen, A. J. et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. Lancet Lond. Engl. 389, 1907–1918 (2017).
Acknowledgements
We thank the National Institute of Statistics and Informatics (INEI in Spanish) for for providing such useful data freely-available to researchers. Gabriel Carrasco-Escobar was supported by NIH/Fogarty International Center Global Infectious Diseases Training Program (D43 TW007120). J.J.M. acknowledges having received support from the Alliance for Health Policy and Systems Research (HQHSR1206660), the Bernard Lown Scholars in Cardiovascular Health Program at Harvard T.H. Chan School of Public Health (BLSCHP-1902), Bloomberg Philanthropies, FONDECYT via CIENCIACTIVA/CONCYTEC, British Council, British Embassy and the Newton-Paulet Fund (223-2018, 224-2018), DFID/MRC/Wellcome Global Health Trials (MR/M007405/1), Fogarty International Center (R21TW009982, D71TW010877), Grand Challenges Canada (0335-04), International Development Research Center Canada (IDRC 106887, 108167), Inter-American Institute for Global Change Research (IAI CRN3036), Medical Research Council (MR/P008984/1, MR/P024408/1, MR/P02386X/1), National Cancer Institute (1P20CA217231), National Heart, Lung and Blood Institute (HHSN268200900033C, 5U01HL114180, 1UM1HL134590), National Institute of Mental Health (1U19MH098780), Swiss National Science Foundation (40P740-160366), Wellcome (074833/Z/04/Z, 093541/Z/10/Z, 103994/Z/14/Z, 107435/Z/15/Z, 205177/Z/16/Z, 214185/Z/18/Z, 218743/Z/19/Z) and the World Diabetes Foundation (WDF15-1224). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Conceived and designed the study: G.C.E., T.B. Data collection and analysis: G.C.E., and L.S. Wrote the manuscript: G.C.E., L.S., J.J.M., and T.B. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Carrasco-Escobar, G., Schwarz, L., Miranda, J.J. et al. Revealing the air pollution burden associated with internal Migration in Peru. Sci Rep 10, 7147 (2020). https://doi.org/10.1038/s41598-020-64043-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-64043-y
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
