
Abstract
Women with estrogen-receptor (ER)-positive breast cancer and no axillary lymph-node involvement are considered to have excellent overall prognosis. However, this population is not homogeneous with regard to risk of recurrence; in fact, some of these patients have a prognosis no better than that of many women with ER-negative tumors or positive axillary nodes. Consequently, better tumor markers and better use of those currently available are needed to distinguish patients who would benefit from more aggressive therapy from those for whom such therapy is unnecessary.
A well-defined cohort of over 4000 breast cancer patients from National Surgical Adjuvant Breast and Bowel Project (NSABP) Protocol B-14 who had ER-positive tumors and no axillary lymph-node involvement was analyzed to ascertain the usefulness of tumor cell S- phase fraction for prognosis. The significance of clinical tumor size, patient age at surgery, ER and progesterone receptor (PgR) expression, and nuclear grade was also explored. Statistical methods based on smoothing splines were used to relate treatment failure and mortality rates to patient and tumor characteristics. Models for 5- and 10-year disease-free survival (DFS) and overall survival were developed and summarized. The attenuation of the prognostic importance of covariates over time was investigated.
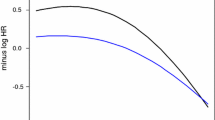
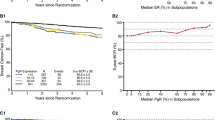
After other characteristics were accounted for, a strong association was found between S-phase fraction and DFS, as well as survival. Tumor size, patient age at surgery, and PgR status were also significantly associated with outcome. The diversity of risk in the B-14 population was more extreme than is generally recognized. The prognostic capabilities of S-phase, tumor size, and PgR status were sharply attenuated as the time from surgery increased.
Similar content being viewed by others

References
Fisher B, Costantino J, Redmond C, Poisson R, Bowman D, Couture J, Dimitrov NV, Wolmark N, Wickerham DL, Fisher ER, Margolese R, Robidoux A, Shibata H, Terz J, Paterson AHG, Feldman MI, Farrar W, Evans J, Lickley HL, Ketner M: A randomized clinical trial evaluating tamoxifen in the treatment of patients with node-negative breast cancer who have estrogen-receptor-positive tumors. N Engl J Med 320:479–484, 1989
Fisher B, Dignam J, Bryant J, DeCillis A, Wickerham DL, Wolmark N, Costantino J, Redmond C, Fisher ER, Bowman DM, Deschenes L, Dimitrov NV, Margolese RG, Robidoux A, Shibata H, Terz J, Paterson AHG, Feldman MI, Farrar W, Evans J, Lickley HL: Five versus more than five years of tamoxifen therapy for breast cancer patients with negative lymph nodes and estrogen receptor-positive tumors. J Natl Cancer Inst 88:1529–1542, 1996
Early Breast Cancer Trialists' Collaborative Group: Tamoxifen for early breast cancer: an overview of the randomised trials. Lancet 351:1451–1467, 1988
Fisher B, Dignam J, Wolmark N, DeCillis A, Emir B, Wickerham DL, Bryant J, Dimitrov NV, Abramson N, Atkins JN, Shibata H, Deschenes L, Margolese RG: Tamoxifen and chemotherapy for lymph node-negative, estrogen receptor-positive breast cancer. J Natl Cancer Inst 89:1673–1682, 1997
Clinical practice guidelines for the use of tumor markers in breast and colorectal cancer. Adopted on May 17, 1996, by the American Society of Clinical Oncology. J Clin Oncol 14:2843–2877, 1996
1997 update of recommendations for the use of tumor markers in breast and colorectal cancer. J Clin Oncol 16:793–795, 1998
Fisher B, Gunduz N, Costantino J, Fisher ER, Redmond C, Mamounas EP, Siderits R: DNA flow cytometric analysis of primary operable breast cancer: Relation of ploidy and S-phase fraction to outcome of patients in NSABP B-04. Cancer 68:1465–1475, 1991
Wilcoxon F: Individual comparisons by ranking methods. Biometrics 1:80–83, 1945
Kaplan EL, Meier P: Nonparametric estimation from incomplete observations. J Am Stat Assoc 53:457–481, 1958
Mantel N: Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother Rep 50:163–170, 1966
Gray RJ: Flexible methods for analyzing survival data using splines, with application to breast cancer prognosis. J Am Stat Assoc 87:942–951, 1992
Cox DR: Regression models and life tables. J R Stat Soc 34:187–220, 1972
Fisher B, Redmond C, Caplan R: Relative worth of estrogen or progesterone receptor and pathologic characteristics of differentiation as indicators of prognosis in node-negative breast cancer patients: findings from National Surgical Adjuvant Breast and Bowel Project B-06. J Clin Oncol 6:1076–1087, 1988
Ewers SB, Attewell R, Baldetorp B, Borg A, Fernö M, Långström E, Killander D: Prognostic significance of flow cytometric DNA analysis and estrogen receptor content in breast carcinomas — A 10 year survival study. Breast Cancer Res Treat 24:115–126, 1992
Costantino J, Fisher B, Gunduz N, Fisher E, Mamounas E, Paik S, Dimitrov N, Bowman D, Margolese R, Kavanah M, Shibata H: Tumor size, ploidy, S-phase, and erbB-2 markers in patients with node-negative, ER-positive tumors: Findings from NSABP B-14 [abstract]. Proc Am Soc Clin Oncol 13:64, 1994
Stål O, Dufmats M, Hatschek T, Carstensen J, Klintenberg C, Rutqvist L-E, Skoog L, Sullivan S, Wingren S, Nordenskjöld B: S-phase fraction is a prognostic factor in stage I breast carcinoma. J Clin Oncol 11:1717–1722, 1993
Shankey TV, Rabinovitch PS, Bagwell B, Bauer KD, Cox C, Duque RE, Hedley DW, Mayall BH, Wheeless L: Guidelines for the implementation of clinical DNA cytometry. Breast Cancer Res Treat 28:61–68, 1993
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Bryant, J., Fisher, B., Gündüz, N. et al. S-phase fraction combined with other patient and tumor characteristics for the prognosis of node-negative, estrogen- receptor-positive breast cancer. Breast Cancer Res Treat 51, 239–253 (1998). https://doi.org/10.1023/A:1006184428857
Issue Date:
DOI: https://doi.org/10.1023/A:1006184428857